
Abstract
Abstract
Purpose:
The laparoscopic surgery for a choledochal cyst in children is technically challenging because of its high degree of complexity despite its possibility. In an attempt to overcome this laparoscopic weakness and to facilitate the difficult steps in the minimally invasive surgery for choledochal cyst resection in children, we have performed the robot-assisted resection of the choledochal cyst. The aim of this study is to report lessons and tips obtained from our experience of the robot-assisted choledochal cyst resection in children.
Patients and Methods:
From July 2008 to October 2011, we have attempted robot-assisted resections of choledochal cyst for 14 children using the da Vinci Robotic Surgical System® (Intuitive Surgical, Sunnyvale, CA). We analyzed retrospectively reviewed medical records for patients' clinical characteristics, operative methods, and postoperative outcomes including operative time, hospital days, and complications.
Results:
In 3 early consecutive cases, we encountered serious technical problems and complications. However, after the operator underwent the robot system off-site training program, complete resection of the choledochal cyst and Roux-en-Y hepaticojejunostomy were performed successfully without difficulty and any complication in the 11 later consecutive cases. The important technical developments of our late-period operations include placing the patient's body above the operative table, performing the extracorporeal jejunojejunostomy through an umbilical incision, omitting the operative cholangiography with magnetic resonance cholangiopancreatography substitution, exposure of the porta hepatis by lateral retractions of the gallbladder and the falciform ligament with anchoring sutures to the abdominal wall, and using a third robotic arm for counter-traction of tissues for careful dissection.
Conclusion:
We believe that the techniques of pediatric robotic choledochal cyst resection have evolved from the previous experiences to be safer and easier.
Introduction
Patients and Methods
From July 2008 to October 2011, we have attempted robot-assisted resection of choledochal cysts using the da Vinci Robotic Surgical System® (Intuitive Surgical, Sunnyvale, CA) for 14 children at Severance Children's Hospital (Seoul, Korea). The diagnoses of choledochal cyst in all patients were made by abdominal ultrasonography and magnetic resonance cholangiopancreatography. To prevent long-term complications from the incomplete removal of impacted stones or protein plugs in the common channel or bleeding from inflamed pericholedochal tissue, those patients either with impacted protein plugs or stones in the common channel or with cholangitis were not recommended for robotic surgery and underwent conventional open resection. However, patients with floating protein plugs or stones were recommended to undergo robotic surgery.
Using the medical record of these 14 patients, we reviewed and analyzed the clinical data regarding patients' demographics, types of choledochal cyst, operative procedure and time, and treatment outcomes. Descriptive statistics were performed using SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL) to evaluate the mean values.
Locations of ports
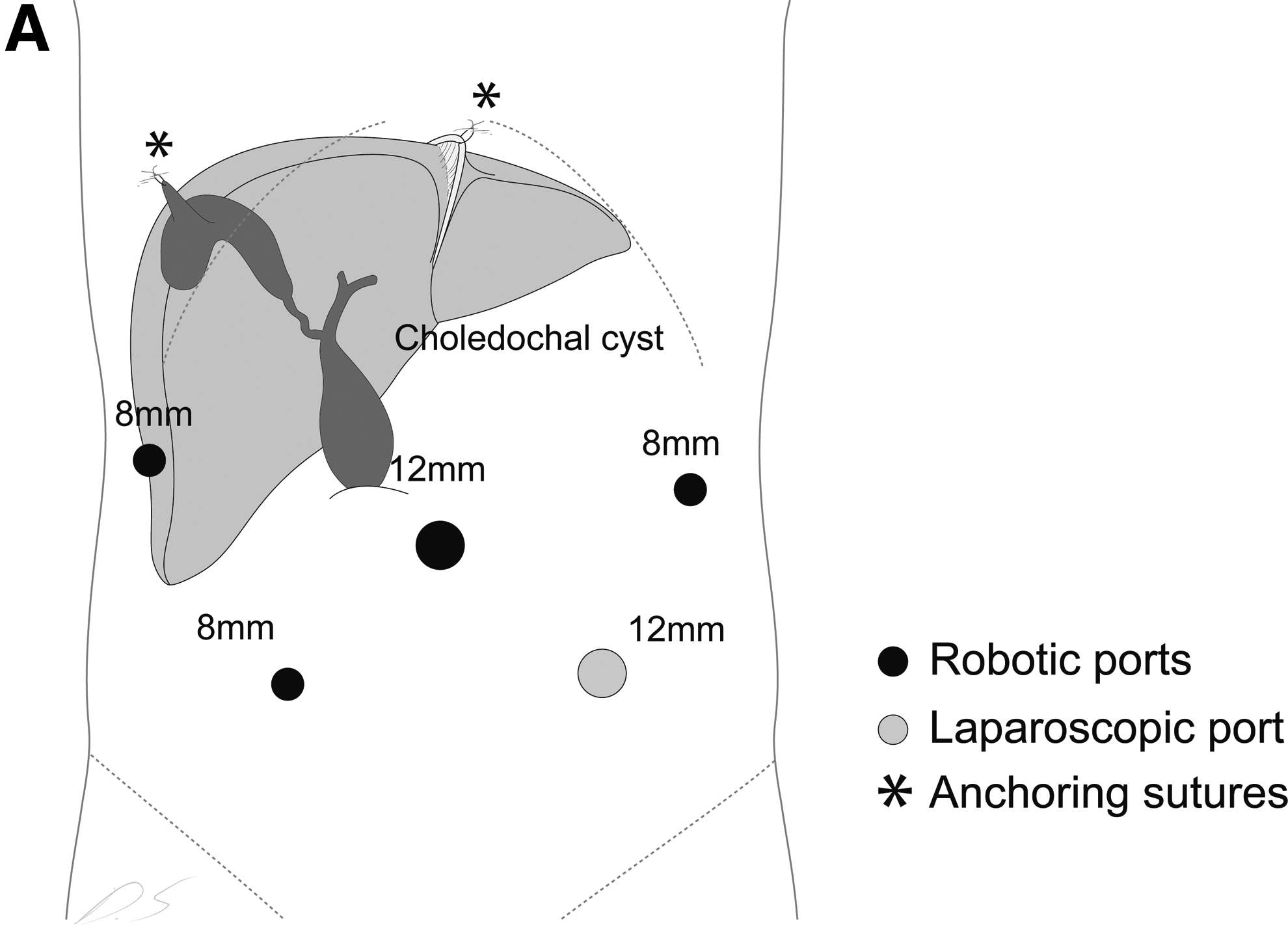
First, a 12-mm camera port was placed through a supraumbilical semicircular incision using the open method 2 (Fig. 1A). Pneumoperitoneum was established by CO2 insufflation, which kept the intraperitoneal pressure below 12 mm Hg. Three 8-mm robotic working ports were placed in the left upper quadrant, right lower quadrant, and right lateral subcostal area. In early cases, we used two robotic working arms because of the small body cavity of pediatric patients. However, we experienced difficulties during dissecting the intrapancreatic portion of the choledochal cyst, so we used a third robotic arm for assisting in the retraction of the liver, pancreas, and tissue as long as sufficient space was available. Additionally, a 12-mm laparoscopic assist port was placed in the left lower quadrant for tissue retrieval, irrigation, and suction and as a passage of suture materials. Positioning of the laparoscopic port at this location was established based upon numerous experiences. The previous locations of the laparoscopic assistant port were at the left upper quadrant or the left lateral side of the abdominal wall. Assistance through these port sites, however, was very difficult and ineffective because the assistant's movements were restricted by the first robotic arm. After the site of the laparoscopic port was changed to the left lower abdomen, more efficient manipulation of the laparoscopic assistance was possible. By using the same-size trocar as the camera port (12-mm), the laparoscopic assistant port was able to be used as a camera port temporarily, such as when delivering out the jejunal loop through the umbilical port to perform an extracorporeal jejunojejunostomy.
Operative techniques
Our operative techniques and outcomes for robotic resection of the choledochal cyst in children were continuously analyzed and improved until consistently good results were attained. Currently, the procedures have been established into two stages (predocking stage and docking stage) as shown in Figure 2.
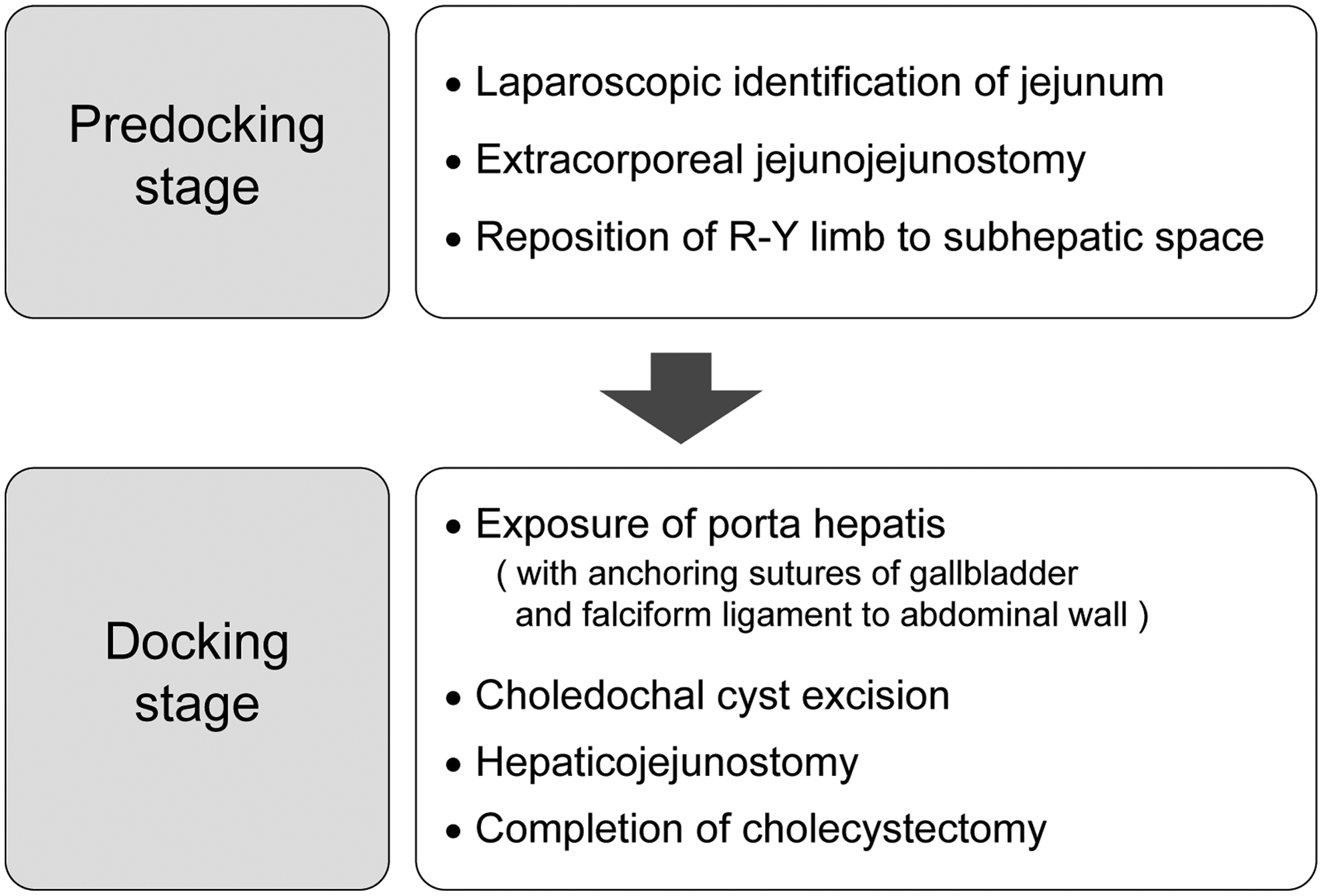
Operative flowchart of robot-assisted choledochal cyst resection in children. R-Y, Roux-en-Y.
Predocking stage
A Foley catheter and a nasogastric tube were inserted into the patient under general anesthesia. To prevent restricting the robotic arm's movement from the operative table, the patient was laid on the operative bed and was raised about 12 cm from the table by insertion of several sheets.
As a first step, port insertion, laparoscopic jejunal identification, and extracorporeal jejunojejunostomy were performed. For jejunojejunostomy, the intracorporeal procedure was achieved in only 1 case of our early robotic surgeries. In later cases, however, extracorporeal procedures were used because the narrow intraperitoneal space of the pediatric patients was not sufficient for safe and easy intracorporeal jejunojejunostomy and mesenteric repair. For extracorporeal jejunojejunostomy, the jejunum was identified 20 cm distal from the ligament of Treitz by laparoscopy and was marked by gentian violet to track the direction of the bowel movement. While the marked jejunum was grasped, CO2 gas was pushed out, and the camera port was removed. After extension of the fascial incision to the cephalad direction in the midline from the umbilical port site, the jejunum was delivered out from the peritoneal cavity via the extended umbilical opening. By the general method, end-to-side jejunojejunostomy was created extracorporeally with mesenteric repair, and the reconstructed jejunum was returned into the peritoneal cavity and was placed in the subhepatic space. The umbilical opening was closed to adjust to the 12-mm camera port so that CO2 gas would not leak.
Docking stage
The patient was placed in the reverse Trendelenburg position. After the operative table was rotated to align the robotic main body with the longitudinal axis of the choledochal cyst (Fig. 1B), the robotic surgical system was docked. For liver retraction, in early cases, a 5-mm laparoscopic liver retractor was used through the port in the left upper quadrant or the right upper quadrant. However, this port was abandoned in later cases because of inhibition of robotic arms' movement and ineffective retraction of the liver. Instead, two traction sutures were used in the gallbladder fundus and the falciform ligament to the abdominal wall, and, occasionally, a robotic third arm assisted the retraction (Fig. 1A). By acquiring a three-dimensional magnified view of the surgical site, we dissected the anterior side of the choledochal cyst nearest to the surface layers. The cyst was divided completely into two parts, and the posterior side of the cyst was dissected. Through the lumen of the proximal part of the cyst, hepatic duct bifurcation was identified, and the cyst below the confluence was resected. The distal part of the cyst was ligated by surgical looping or clipping after dissecting the most distal common bile duct to the pancreatic duct. For intracorporeal hepaticojejunostomy, the premade Roux-en-Y limb was placed in the porta hepatis area. In earlier cases, we used the antecolic route for pull-up of the Roux-en-Y limb. However, in later cases the retrocolic route was used through the window of the transverse mesocolon. Hepaticojejunostomy was performed by using Vicryl® (Ethicon) 5-0 interrupted sutures. A tip in this step is making the opening of the jejunal end of its anterior side to facilitate easier hepaticojejunostomy when extracorporeal jejunojejunostomy is performed. The sutures in the gallbladder and the falciform ligament were removed, and cholecystectomy was done. All resected specimens were retrieved via a 12-mm laparoscopic port. As the last step after dedocking the robotic surgical system, the abdominal cavity was irrigated, and a closed suction drain was inserted near the anastomosis. All ports were removed, and the port sites were closed.
Postoperative progress
An oral diet was initiated when the patient's bowel movement became normal. The patient was discharged after verification that normal diet was given and no complications existed. All patients were followed up at our clinic at 1 week postoperatively. The next follow-up intervals were scheduled at 3 months, 6 months, and annually.
Results
During the study period, robot-assisted resections of choledochal cysts in children were attempted in 14 cases. The clinical characteristics of all cases are shown in Table 1. Among them, 13 cases were treated successfully by the robotic system. Postoperative complications developed in 3 earlier consecutive cases: one open-conversion, one anastomotic stricture, and one anastomotic leakage. Anastomotic stricture was resolved by reoperation, but anastomotic leakage was recovered by conservative treatment. During the recent follow-up, no other complication was reported from any patient (mean follow-up period, 14.2 months; range, 4.7–43.2 months). The changes of operative procedures are shown in Figure 3. Jejunojejunostomy was created intracorporeally in 1 case and extracorporeally in the rest. Roux-en-Y hepaticojejunostomy was fashioned by the antecolic method in early cases, but the retrocolic method was used in the late cases. Operative cholangiography was performed just in 2 early cases and was abandoned in later cases. A third robotic arm was used in 5 later cases.
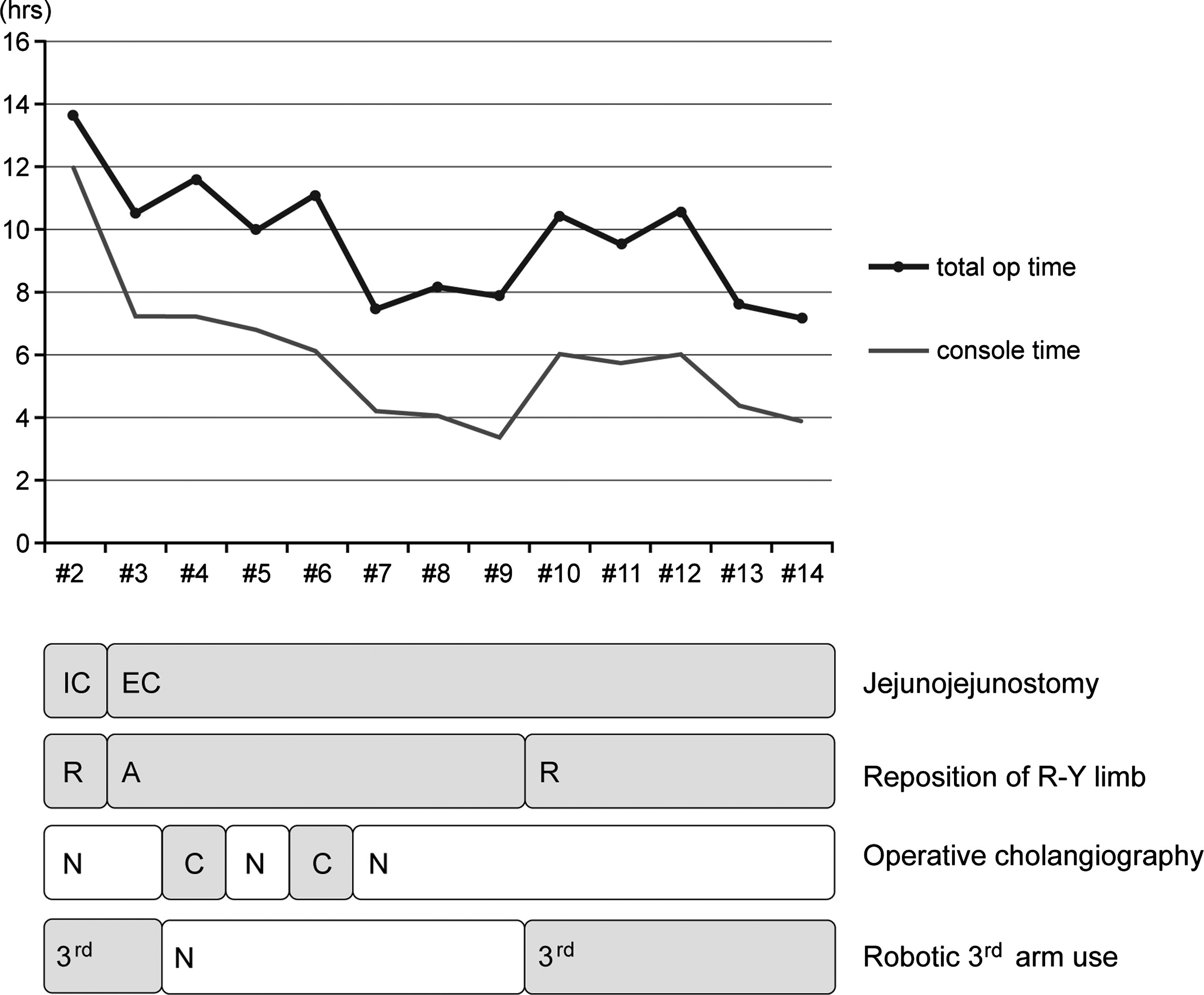
Changes of operative time and procedures with increasing number of cases. Overall 13 cases were successfully finished using the robotic system and are shown in the chart. The first case (Case 1) was excluded because of open conversion due to failure of the robotic surgery. In general, the operative time decreased with the accumulation of cases. The changes in operative time according to the application of several operative techniques are shown. 3rd, robot-3rd arm use; A, antecolic; C, operative cholangiography; EC, extracorporeal; IC, intracorporeal; N, no use; R, retrocolic.
The mean operation time was 9.5 hours (range, 7.2–13.6 hours). The mean console time was 5.4 hours (range, 3.3–7.3 hours). Postoperative mean hospital stay was 9.0 days (range, 8–18 days). The total operation time and console time decreased until Case 9. During the following 3 cases (Cases 10, 11, and 12), the operation time increased again because the retrocolic hepaticojejunostomy was applied and a third robotic arm was used. In the last 2 cases, however, the operation time decreased again.
Discussion
Recently, minimally invasive surgery has been introduced to treat the pediatric choledochal cyst because of the advantages such as better cosmesis, less postoperative pain, early comeback to social life, and less postoperative adhesion. In 1995, a successful laparoscopic surgery for choledochal cyst was performed, 1 but the active performance of laparoscopic surgery has been limited to a few institutions. 3 The laparoscopic surgery for a choledochal cyst is slower in adaptation than other laparoscopic operations such as laparoscopic appendectomy because a complex procedure such as hepaticojejunostomy needs considerable experiences and efforts.
To overcome this limitation of laparoscopic surgery for the hepaticojejunostomy during choledochal cyst excision, some surgeons have performed hepaticoduodenostomy instead of hepaticojejunostomy. 3 However, hepaticoduodenostomy was reported as a potential cause for the “sump syndrome” due to the reflux of duodenal contents to the biliary tract and the progression to more serious conditions. Hepaticojejunostomy has the structure of the Roux-en-Y limb that can prevent the reflux of bowel contents to the biliary tract, so it has less possibility of causing the sump syndrome.3–8 We believe that the most important principle of treatment for a choledochal cyst is the total resection of the pathological cyst and the safe reconstruction of the biliary tree (hepaticojejunostomy), and these principles should be applied for minimally invasive surgery of the choledochal cyst. We believed that despite the high cost, the robotic surgical system is the alternative minimally invasive surgery that is able to overcome the limitations of laparoscopic surgery in complex biliary procedures. A robotic camera can provide three-dimensional images of the operative field magnified up to 12 times, and the vision can be controlled by the operator. Robotic arms can also allow intuitive manipulations with tremor filtration, motion scaling, and endo-articulation of robotic instruments. For this reason, robotic surgery can perform a complex operation that cannot be carried out easily in laparoscopic surgery.9–12 Especially in children, whose organs are smaller than those in adults, the robotic system is valuable in performing a complex hepatobiliary operation. 13 However, several complications and operative failures reported in early studies of robotic surgery for the choledochal cyst might give rise to a skeptical view. 14 Recently, as the experience of robotic surgery in children has been accumulating, it is highly encouraging that successful robotic surgery can be performed in children less than 10 kg with a choledochal cyst. 15
We also underwent a learning curve to successfully apply the robotic system for operation on a choledochal cyst in children. In 3 early cases, we experienced one open conversion and two complications. The first case was open-converted because surgeons were inexperienced with the robotic system and were unable to secure the operative view. In the second case, despite the success of robotic surgery, postoperative stricture at the site of hepaticojejunostomy developed and was resolved by reoperation. An anastomotic leakage occurred in the third case, but it was spontaneously closed by conservative management. In subsequent cases, no further complication was observed in our follow-up. The operation time was relatively long in early cases. After 14 cases of robot-assisted choledochal cyst excision, however, we achieved our own organized steps for the procedure as shown in Figure 2. The robotic system was initially designed for adult patients; therefore, this system may present some limitations when it is applied to pediatric patients who have a relatively small intra-abdominal space. Thus we suggest the following measures until the new robotic system adequate for children is introduced.
First, the patient should be positioned at least 12 cm above the operative table. This is to prevent the operative table from limiting the robotic arm's movement. Second, extracorporeal jejunojejunostomy through the umbilical incision is safe and time saving. In many reports, extracorporeal jejunojejunostomy was performed because intracorporeal jejunojejunostomy in the small intra-abdominal space of children is often time consuming, has a poor operative view, and cannot achieve secure anastomosis.14–17 Third, the anchoring sutures of the gallbladder and falciform ligament are advantageous in children. For the exposure of the porta hepatis, two traction sutures in the gallbladder fundus and the falciform ligament to the abdominal wall can be used effectively without requiring an additional laparoscopic port for a liver retractor. Fourth, operative cholangiography may be dispensed with because this procedure requires robot-dedockng and is time consuming. Instead, confirming the bile duct anatomy through magnetic resonance cholangiopancreatography should be done preoperatively. Lastly, we recommend the use of a third robotic arm when feasible because it can be used to assist the liver retraction or counter-traction of tissues, particularly during the dissection of the intrapancreatic bile duct. We did not use a third robotic arm in our early cases because of limited space to use it in the pediatric abdominal cavity. However, we were able to complete resection of a dilated distal cyst of type IVa and create the retrocolic Roux-en-Y limb in later cases by using a third robotic arm.
However, a technical limitation of robot-assisted choledochal cyst resection in children still remained. We excluded patients with an impacted protein plug or stones in the distal common channel from robotic surgery because we thought it would be hard to remove the impacted protein plug from the distal common channel. We checked the status of the distal common channel fastidiously by ultrasonography or magnetic resonance cholangiopancreatography preoperatively. If the impacted stone in the distal common channel was identified, open surgery was recommended for complete removal of the stones or plug from the common channel. However, floating stones and debris in the cyst and intrahepatic ducts were easily removed by transecting the cyst during dissection of the choledochal cyst. We also excluded patients with acute cholangitis from robotic surgery because it is difficult to control bleeding from inflamed friable pericholedochal tissue during robotic surgery. The last technical limitation of the current robotic system in children to overcome is the small size of the patient's body. Although the data are not included in the current study, we found that robot-assisted choledochal cyst resection can be successfully performed without difficulty in babies with a weight of 7 kg.
Conclusions
Robotic surgery of a choledochal cyst in children is safe and feasible. For successful operations in small-sized pediatric patients, the adjusted method can be helpful. Also, further application of robotic surgery in children can be a good prospect.
Footnotes
Acknowledgments
This study was supported by the 2011 Robotic Surgery Activation Fund from the Yonsei University College of Medicine. The authors thank Mr. D.S. Jang for his excellent support with medical illustration.
Disclosure statement
No competing financial interests exist.