
Abstract
Abstract
Background and Aim:
Laparoscopic-assisted distal gastrectomy (LADG) has recently become an alternative treatment option for gastric cancer. Although LADG is safe and feasible in terms of short-term patient results and oncological outcomes, the long-term oncological efficacy of LADG has yet to be demonstrated. To that end, the long-term results and the survival of patients who underwent LADG are described in this study. We also evaluated the oncological safety of using this approach for the treatment of gastric cancer.
Subjects and Methods:
Between January 2006 and December 2009, 133 patients with lower-third gastric cancer underwent LADG performed by a single surgeon. The clinicopathologic characteristics, long-term survival, and relapse-free survival were estimated using the Kaplan–Meier method.
Results:
Postoperative morbidity occurred in 5.6% of the patients. One patient died within 30 days of undergoing the operation (0.8%). The median overall survival (OS) of patients who underwent LADG was 45.0 months (range, 1.0–69.0 months). The median follow-up period of all patients was 37.0 months (range, 1.0–69.0 months). The 3-year OS rates according to cancer stage were 94.8% at Stage I, 84.6% at stage II, and 50.0% at Stage III. The median OS in patients who had a recurrence and those who had not had a recurrence was 27.0 (6.0–62.0) and 45.0 (1.0–69.0) months, respectively.
Conclusions:
LADG with lymph node dissection for gastric cancer is a valuable procedure from technical and oncological perspectives with acceptable long-term outcomes. Therefore, LADG can be substituted for open distal gastrectomy with similar effectiveness.
Introduction
Laparoscopic-assisted distal gastrectomy (LADG) for EGC was first reported in 1994 by Kitano et al. 2 Since then, many researchers have reported their experiences with the use of LADG in EGC and have provided evidence of the advantages of LADG, including less pain, a shorter recovery period, shortened hospital stay, and a good quality of life, with adequate resection margins and lymph node clearance.3,4 Additionally, although the frequency is not high, a few studies have also shown the efficacy of LADG in managing advanced gastric cancer.5,6 For these reasons, LADG has recently become an alternative treatment option for gastric cancer. However, laparoscopic surgery for gastric cancer remains controversial because there are insufficient studies on the long-term outcomes of LADG. Although LADG is safe and feasible in terms of short-term patient results and oncological outcomes, the long-term oncological efficacy of LADG has yet to be assessed. In this study, the long-term outcomes and survival of patients who underwent LADG were investigated, and the oncological safety of this approach in the treatment of gastric cancer was evaluated.
Subjects and Methods
Between January 2006 and December 2009, 133 patients with lower-third gastric cancer underwent LADG performed by a single surgeon at the Department of Surgery, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. Only tumors located in the lower third of the stomach and confined to the subserosal layer (T2b) in terms of depth of invasion as seen on preoperative examination were included in this study. Patients with a T4 tumor, distant metastases, or obvious serosal cancer involvement upon preoperative examination were excluded from this study. Because of severe adhesion (9 cases) and a bleeding tendency (1 case) during LADG, 10 cases were converted to open gastrectomy and excluded from this study. Thus, 123 patients who underwent LADG were ultimately enrolled.
Prior to the operation, we assessed the depth of invasion by endoscopy and endoscopic ultrasonography, as well as the presence or absence of lymph node metastases using extracorporeal ultrasonography and computed tomography (CT). Patients with advanced gastric cancer received chemotherapy with intravenous 5-fluorouracil and cisplatin, and patients with EGC received oral 5-fluorouracil. This study protocol was approved by our hospital's ethics committee. Demographics and perioperative and postoperative data were retrospectively collected from hospital records and analyzed. Follow-up data were obtained from patients' clinic records, as well as postoperative CT and endoscopy results.
All patients were placed in the supine position under general anesthesia. Two 12-mm trocars, three 5-mm trocars, and a flexible laparoscope were used during surgery. The surgeon stood on the left side of the patient. A CO2 pneumoperitoneum was achieved through a 12-mm umbilical trocar and set at 15 mm Hg. According to the Japanese Classification of Gastric Carcinoma, 7 extended lymph node dissection (D2) and D1+β (D1 + numbers 7, 8a, and 9) lymph node dissection were the preferred procedures. D1+α (D1 + number 7) lymph node dissection was also performed in older and high-risk patients, with the aim of reducing postoperative complications.
During surgery, separation of the greater omentum from the transverse colon was initiated from the left and continued rightward to the hepatic flexure with a Harmonic® scalpel (Ethicon Endo-Surgery, Cincinnati, OH). The superior leaf of the mesocolon was resected. The superior mesenteric vein, right colic vein, and right gastroepiploic vein were exposed in order to dissect lymph node number 14v. The right gastroepiploic vein and artery were clamped with titanium clips and divided individually at their roots, and the infrapyloric lymph nodes (number 6) were dissected. The left gastroepiploic vessels were divided at their origin for dissection of lymph node number 4sb. The right gastric vessels were divided, and the nodes along the proper hepatic artery in the hepatoduodenal ligament were dissected (number 12a). The suprapyloric lymph nodes (number 5) were dissected after the right gastric vessels were cut. The duodenum was transected 3 cm distal to the pylorus with an endoscopic linear stapler. The lesser omentum was opened, and the stomach was turned headward to expose the gastropancreatic fold. The splenic artery was first exposed on the left side for lymph node dissection (number 11p). Once lymph node number 11p was dissected, the dissection was continued rightward along the artery to remove the nodes along the celiac trunk, left gastric artery, and common hepatic artery (numbers 7, 8a, and 9). The left gastric artery was clamped with titanium clips and cut at its origin from the celiac trunk. The perigastric nodes were dissected along the upper lesser curvature to the esophagocardial junction. The trocar incision in the epigastrum was extended vertically or horizontally to 5 cm. The laparotomy wound was protected and retracted using a wound retractor (Alexis®, Applied Medical, Rancho Santa Magarita, CA). The stomach was resected through the window, and Billroth I reconstruction was performed with a circular 29-mm stapler. When Billroth I was technically impossible, Billroth II reconstruction was performed with hand sutures. A closed-suction drain was placed in Morrison's pouch with closure of the port site and the incision site at the end of the operation.
All patients were monitored postoperatively by physical examination and laboratory tests, including those for tumor markers, chest radiography, abdominopelvic CT, and endoscopy, every 6 months for the first 2 years and then annually. If necessary, further evaluation, such as positron emission tomography or magnetic resonance imaging, was initiated to better clarify a recurrence.
Overall survival (OS) and relapse-free survival were estimated using the Kaplan–Meier method. OS was calculated from the day of surgery until death or until the end of follow-up. Relapse-free survival was calculated from the day of surgery to the day of recurrence or death. Multivariate analyses for survival were conducted using Cox's proportional hazard model. A P value of <.05 (two-sided) was considered statistically significant. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 18.0 for Windows (SPSS, Inc., Chicago, IL).
Results
The clinicopathologic characteristics of the patients are summarized in Table 1. The study group consisted of 80 men and 43 women with a mean age of 61.1±11.8 years (median, 61.0 years; range, 31.0–89.0 years). According to the Sixth Edition of the American Joint Committee on Cancer TNM classification system, 102 patients had Stage I (82 IA + 20 IB), 13 patients had Stage II, and 8 patients had stage III (3 IIIA + 5 IIIB) gastric cancer.
AGC, advanced gastric cancer; EGC, early gastric cancer.
Postoperative surgical results are summarized in Table 2. Most of the patients underwent a D1+β or D2 lymph node dissection (91.1%). The mean number of retrieved lymph nodes was 29.3±12.9 (median, 28.0; range, 6.0–68.0). Postoperative morbidity occurred in 5.6% of the patients. One patient died within 30 days of undergoing the operation (0.8%). The patient presented with a duodenal stump leakage after 5 days and underwent a second operation but died of sepsis.
BI and BII, Billroth I and Billroth II, respectively; LN, lymph node; R0, no residual tumor/complete resection; R1, microscopic residual tumor.
The median OS of patients who underwent LADG was 45.0 months (range, 1.0–69.0 months). The median follow-up period for all patients was 37.0 months (range, 1.0–69.0 months). During the follow-up period, 13 patients died (10.5%). Causes of death were gastric cancer (n=8), gallbladder cancer (n=1), pneumonia (n=1), and old age (n=3). The median OS of the deceased patients was 22.0 months (range, 1.0–52.0 months). The 3-year OS rate for all of the patients was 90.5%. The 3-year OS rates according to cancer stage were 94.8% for Stage I, 84.6% for Stage II, and 50.0% for Stage III (Fig. 1). However, because 5 patients had passed away due to other causes, the disease-specific 3-year OS was 93.9%, and the disease-specific 3-year OS rates according to cancer stage were 98.0% for Stage I, 84.6% for Stage II, and 58.3% for Stage III.
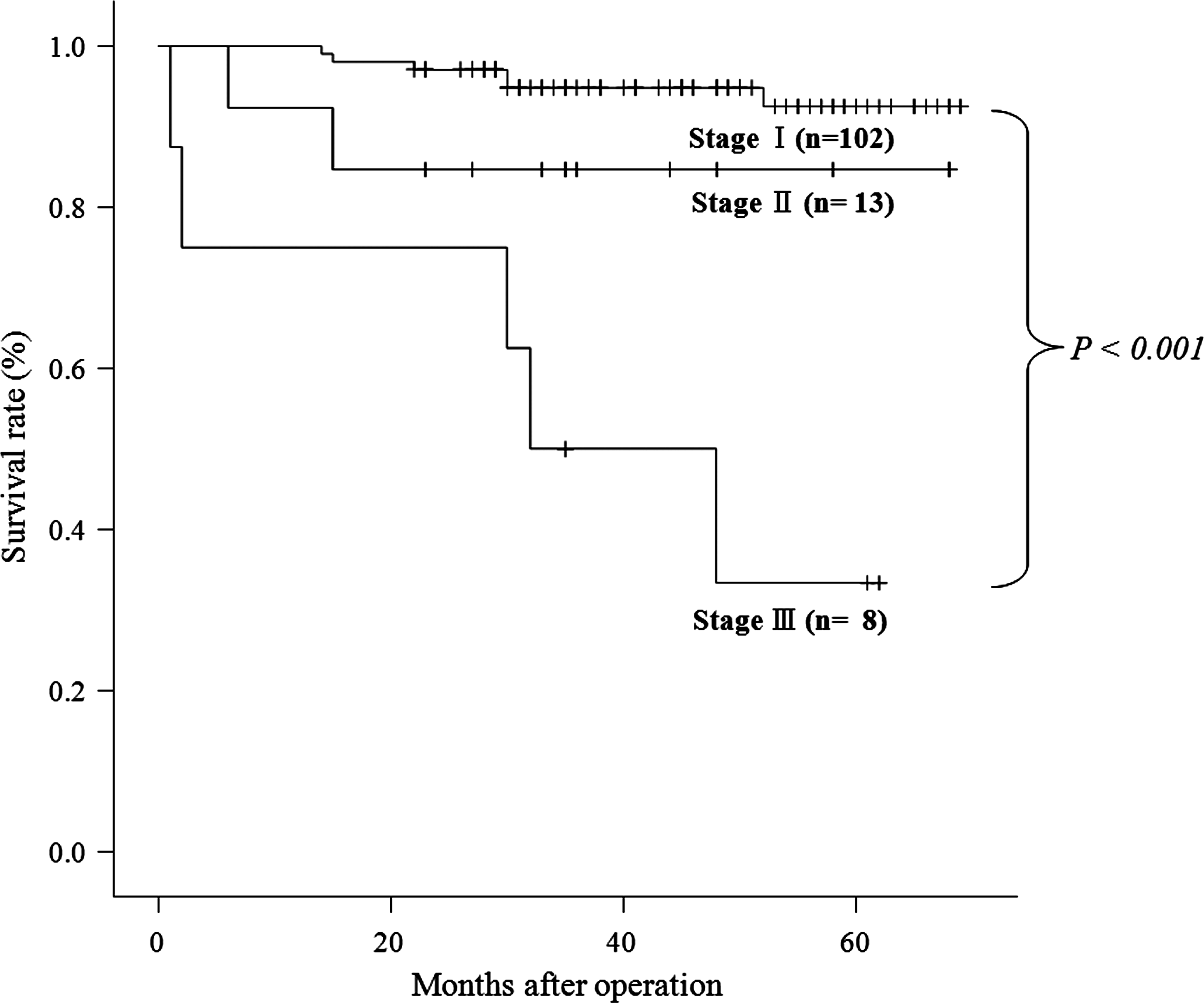
Overall survival curve for each stage (Stages I, II, and III) (P<.001).
Postoperative recurrence occurred in 9 patients (7.3%). Recurrence was found in three distant organs (two in the liver and one in the right adnexa), three in the lymph nodes, two in the peritoneum, and one in an anastomosis site. Two patients with EGC (IA, IB) had liver and lymph node recurrence, respectively. Most of the recurrences (7 patients) occurred within 3 years of the operation, and 7 of the 9 patients who had a recurrence died (77.8%). The median relapse-free survival in patients who had a recurrence was 16.0 months (range, 6.0–58.0 months).
This study compared the characteristics of the recurrent group and the non-recurrent group. There were no significant differences in age, sex, postoperative day, differentiation of tumor, tumor size, and length of the proximal and distal margins between the groups. However, T stage, N stage, TNM stage, number of retrieved lymph nodes, number of metastatic lymph nodes, lymphatic invasion, venous invasion, and perineural invasion were significantly different between the two groups (P<.05). The median OS in patients who had a recurrence and those who did not was 27.0 (6.0–62.0) and 45.0 (1.0–69.0) months, respectively, and this difference was also significant (P=.005).
T stage, N stage, lymphatic invasion, and perineural invasion were significant prognostic factors on univariate analysis (Table 3). In addition, although venous invasion was not analyzed as a prognostic factor, it qualified as such, with a P value of .059. We also identified independent prognostic factors using multivariate analysis (with the covariates of T stage, N stage, lymphatic invasion, perineural invasion, venous invasion, age, and sex) using the enter method. Based on the multivariate analysis (Table 4), N stage was the most powerful prognostic factor.
CI, confidence interval; HR, hazard ratio.
Discussion
Because of the better cosmetic effect, improved quality of life, less intense pain, shortened hospital stay, faster rehabilitation, and early return to social activity, many patients with gastrointestinal disease prefer laparoscopic surgery. 8 Since Kitano et al. 2 first applied and described LADG as a possible treatment for EGC in 1994, the use of LADG has rapidly increased, with remarkable advances in laparoscopic surgical techniques and instruments, including laparoscopic coagulating shears. 9 With the increasing number of laparoscopic gastrectomies, many studies have reported on the short-term outcomes and the safety of this procedure with favorable results in treating EGC.10–12 Additionally, a few studies have shown the efficacy of LADG in the management of advanced gastric cancer.5,6,10 However, the use of LADG in gastric cancer has not yet met with widespread acceptance because of the lack of evidence regarding the oncological adequacy of laparoscopic procedures and the long-term results. Therefore, the aim of this study was to investigate the oncological adequacy and long-term outcomes of LADG in gastric cancer patients.
Bonenkamp et al. 13 failed to show that D2 dissection had a survival benefit over D1 dissection. Ichikura et al. 14 reported that D1+β (D1 + 7, 8a, 9) dissection resulted in a survival rate almost equal to that of D2 dissection in T2 or more advanced gastric cancer, and D1+β dissection may be preferable to D2 dissection in terms of operative morbidity and mortality. The majority of patients in this study were treated using laparoscopic D2 or D1+β lymph node dissection. However, D1+α dissection was also performed in order to reduce postoperative complications in high-risk patients. The number of retrieved lymph nodes is the most objective index when judging the relevance of lymph node dissection. Previous studies reported that 20–40 lymph nodes were retrieved.15–18 Median values of 28 (range, 6.0–68.0) lymph nodes were retrieved by LADG in this study, and this number is comparable to that reported by previous studies on the use of open distal gastrectomy and LADG.
Previous studies have reported the range of postoperative mortality rates for laparoscopic gastrectomy as being between 0% and 7%.4,16,18 In the present study, 1 patient (0.8%) died within 30 days after LADG, and the postoperative morbidity rate was 5.6% (7 patients), which is comparable to rates reported in other studies.19,20 Huscher et al. 4 reported that the 3-year survival rate of patients with gastric cancer, including those with advanced gastric cancer, who underwent LADG was 69% during the follow-up period, which averaged 46 months (median, 25 months). Yoo et al. 21 reported that the 3-year OS rate of 182 patients with EGC who underwent LADG was 97.3%. In this study, the disease-specific 3-year OS rates according to cancer stage were 98.0% for Stage I, 84.6% for Stage II, and 58.3% for Stage III. These rates are comparable to those found in other LADG4,21 and conventional open gastrectomy for advanced gastric cancer 22 studies. Additionally, the risk factors for survival after LADG were not different from those of conventional open gastrectomy.23,24
In our study, recurrence manifested in a variety of ways. Peritoneal recurrence, regional lymph node recurrence, and recurrence of remnant stomach rates were 1.6%, 2.4%, and 0.8%, respectively. These rates and patterns are comparable to those of previous open gastrectomy studies.24,25 Although both the recurrent and non-recurrent groups were similar in terms of preoperative condition and postoperative results, the recurrent group had a significantly shorter median OS (P=.005) and more risk factors (P<.05). These differences were likely not due to a technical defect but a result of the many risk factors inherent to gastric cancer. Therefore, LADG is an acceptable treatment for gastric cancer even in light of the complications in patients who experience a recurrence. Given that, in general, long-term survival is evaluated over 5 years, 37 months (range, 1.0–69.0 months) for a median follow-up period and an analysis of 3-year OS may be considered insufficient to develop definitive conclusions with regard to the effectiveness of LADG. However, because most recurrences of gastric cancer occur within 3 years, 26 a median follow-up period of 37 months is adequate to evaluate long-term results.
In conclusion, this study confirms that LADG with lymph node dissection for gastric cancer is a valuable procedure in terms of both technical and oncological results, with acceptable long-term outcomes. Therefore, LADG can be substituted for open distal gastrectomy with similar effectiveness. Nevertheless, a multicenter, prospective, randomized controlled study is needed to overcome the limitations of the present study, including the use of a single surgeon, a relatively small sample size, and a biased patient distribution.
Footnotes
Disclosure Statement
No competing financial interests exist.