
Abstract
Abstract
Purpose:
A prospective and retrospective work to evaluate management of post-cholecystectomy biliary injuries.
Patients and Methods:
From March 2000 to February 2010, 419 patients (224 females and 195 males) complaining of post-cholecystectomy biliary injuries were managed using surgery in 135 patients and endoscopy in 317 patients, in addition to percutaneous techniques in 32 patients.
Results:
Endoscopy was very successful initial treatment of 317 patients (76%), as being less invasive, with low morbidity and mortality, and being competitive with surgery in treatment of mild/moderate biliary leakage (82%) and biliary stricture (74%). Its success increased by 2.8% and 8.3% for leakage and stricture, respectively, by addition of percutaneous techniques. However, surgery was needed for major leakage and massive stricture in 19% and 14% of cases, respectively. Surgery remains the choice in common bile duct transection, ligation, and combined injuries of stones, stricture, and leakage in 60% of cases. Bilio-enteric anastomosis was the procedure of choice, done in 76 cases, with trans-anastomotic stent in 30 cases with unhealthy or small ducts. Stricture was encountered in 5 cases (6.5%), treated by the percutaneous route in 3 cases and repeat surgery in 2 cases. The learning curve seems influential in both endoscopy and surgery. The cumulative experience increased the success of endoscopy from 60% to 95%. Also, surgery improved with decreased morbidity and mortality.
Conclusions:
Endoscopy was competitive with surgery in initial treatment of simple problems, but in major leak, ligation, transection, and complex problems, surgery plays the main treatment with its invasiveness and high morbidity and morbidity. Cumulative experience influences endoscopic and surgical treatment of such challenging problems.
Introduction
Biliary injuries continue to be a significant problem following cholecystectomy, 5 liver transplant, 7 trauma, 8 or infection. 9 Traditionally, surgery has been the gold standard for the management of biliary injuries. Recently, various endoscopic methods have been used as the preferred modalities of these patients,8,10 as it permitted a less invasive approach, with similar or reduced morbidity rates at surgical treatment.11,12 Since the 1990s these endoscopic approaches have nearly replaced surgical treatment. 13
Endoscopic intervention is a safe and effective method of treatment of post-cholecystectomy biliary injuries as it can combine both the investigative and therapeutic arms in one common procedure. 14 However, management should be individualized based on factors such as outpatient or inpatient and presence of stone, stricture, ligature, or coagulopathy. 15 However, new endoscopic approaches allow less invasive treatment, 16 therefore postponing or even avoiding surgical treatment, 17 and should be the initial management of choice. 18
Surgical treatment still is the cornerstone of treatment; it involves anastomosing an isolated loop of jejunum to the healthy, vascularized and unscarred part of the bile duct, as conventional surgical wisdom dictates avoiding the scarred and unhealthy part of the stricture for anastomosis. Roux-en-Y hepaticojejunostomy is a one-time, proven-effective, and durable method of treating postoperative bile duct injuries, even for recurrent strictures, and has been shown to give good long-term results, 19 sometimes with the use of trans-anastomotic stents according to the individual characteristics of each patient and the experience of each surgeon. However, its use is recommended when unhealthy (ischemic, or scarred) and small (<4 mm) ducts are found. 20
Compared with surgery, endoscopic treatment has the advantage of being less "invasive," but it is less effective, sometime needs multiple sessions, and is certainly not suitable for all patients. In patients with strictures affecting the region of biliary bifurcation and in those with significant loss of length of bile duct, endoscopic stenting has a high chance of failure. 21
The aim of the present article is to emphasize and evaluate the role of both endoscopy and surgery, whether it is competitive or complementary in management of each aspect of post-cholecystectomy problems, relative to the experience curve for more than 10 years in this field in a major referral center in upper Egypt.
Patients and Methods
A random sample of 419 patients was evaluated in this study for about a 10-year period from the surgery department and the gastrointestinal endoscopy unit of Assuit University Hospitals (a major tertiary referral center in Upper Egypt). All patients complained of post-cholecystectomy complex biliary injuries (patients with nonbiliary problems or problems associated with vascular injuries were excluded). Patients were encountered with variable presentation and timing from the surgical insult until referred to our center for management.
Cases were subjected to:
• Thorough detailed history taking • Meticulous clinical examination • Investigations needed to diagnose the problem, such as liver function tests and abdominal ultrasonography, were done for all cases. • Computed tomography or magnetic resonance imaging was done in some cases. • Cholangiogram was done in all cases (the gold standard evaluation of biliary injuries
14
) as a trans-tube cholangiogram (with a T-tube in place), an endoscopic cholangiogram (endoscopic retrograde cholangiopancreatography [ERCP]) in most cases, or percutaneous transhepatic cholangiogram in some selected cases in which endoscopic approaches failed.
Patients were categorized according to the presentation into the biliary leakage group and the biliary stricture group as diagnosed by the previous tools. Each group was managed according to its circumstances by a stepwise manner of treatment, starting with the minimally invasive tools (endoscopic treatment, alone or in addition to percutaneous manipulation in difficult cases) to the more invasive surgical treatment.
Endoscopic approaches
Endoscopy was attempted in 322 patients using a side-viewing Pentax videoscope, with regular instruments, and blended current was used in sphincterotomy; however, balloon sphincteroplasty was also used in some cases.
Biliary leakage
Biliary leakage, classified according to the classification of Strasberg et al., 3 was treated endoscopically by sphincterotomy in mild cases and/or stenting in moderate to major leakage, with concomitant stone extraction if present within the common bile duct (CBD) (retrieval using basket, balloon extractor, or manual mechanical lithotripsy), and also dilation of the associated stricture.
Biliary stricture
Biliary stricture, categorized according to the classification of Strasberg et al., 3 was treated endoscopically by dilatation and stenting in repeated endoscopic sessions with upgrading of stents until a cure was obtained (after full dilatation of the stricture segment as evident by loss of the waist in the cholangiogram or after full dilation for 2 years from the initial session).
Percutaneous manipulation
Percutaneous manipulation was attempted in 32 cases of endoscopic failure to opacify the proximal biliary tree as in major CBD injuries, transection, or ligation through percutaneous transhepatic cholangiogram prior to surgery, percutaneous manipulations and guide wire deployment through the CBD prior to combined procedures (rendezvous technique), or percutaneous dilatation and stenting for stricture or injury.
Surgical approaches
The surgical approach was attempted in 131 cases for the following maneuvers:
• Peritoneal lavage and drainage for biliary peritonitis • CBD repair on a T-tube splint in a minor laceration injury of the CBD • Choledocholithotomy procedure in associated CBD stones • Undoing of ligation and stricturoplasty with a T-tube splint if CBD ligation was discovered very soon • Bilio-enteric shunt operation and anastomosis is done as a Roux-en-Y loop choledochojujenostomy side-to-side, single interrupted layer of 3/0 or 4/0 Vicryl® (Ethicon) sutures, tension free, mucosa to mucosa, 2–3-cm stoma, splinted in very small ducts by a biliary stent. It is done for CBD injury, transection, stricture fibrosis, or bad patient compliance to repeated endoscopic sessions.
Follow-up
Parenteral antibiotics were prescribed for all cases (ciprofloxacin).
Endoscopically and percutaneously treated cases were discharged at the next day after assurance of the stable condition of the patient. Surgically treated cases were followed up in the hospital for a variable period prior to discharge (3–10 days) with the appropriate treatment and follow-up. All cases were followed up for a period of 2–5 years post-procedure, and complications were recorded.
Data of all patients were collected and categorized, with thorough discussion of the detailed results of treatment for each category to reach a consensus on whether endoscopic maneuvers can substitute for surgery as a definitive treatment of such a problem (a competitive treatment), or whether surgery still is needed for definitive treatment and these maneuvers are just complementary tools prior to surgery.
Results
From March 2000 to February 2010, 419 cases of post-cholecystectomy biliary injuries were evaluated for this study. The mean patient age was 45.3 years, with a range of 18–68 years, 224 of the 419 were females, and only 50 of the 419 cases (12%) were operated on in our center. Cases presented either early within a month postoperatively in 240 of the 419 cases or late after surgery in 179 of the 419 cases.
Most of our cases (317 cases [76%]) presented after open access approaches (cholecystectomy alone in 210 cases and with CBD exploration in 107 cases), versus 102 cases presented after laparoscopic approaches.
Investigations
Cholangiogram was the main step of diagnosis in these cases and was done for nearly all patients (380 of 419 cases [91%]), by endoscopy in 322 patients (77%), complemented by the percutaneous transhepatic route in 32 patients (8%) and magnetic resonance cholangiopancreatography in 77 patients (18%), as shown in Table 1.
CBD, common bile duct.
Management
Cases were categorized into the following groups and managed accordingly. Treatment was done by either endoscopic approaches alone or in conjunction with percutaneous approaches in some cases or surgical approaches as follows.
Biliary leakage (245 cases)
Cholangiogram demonstrated leakage to a minor degree in 80 cases (55%), major leakage in 46 cases (32%), and possible CBD transection injury in 18 cases (4.3%), leakage with CBD stone shadow in 65 cases (15.5%), and leakage with CBD stricture in 17 cases (4.1%), but in 19 patients evident leakage clinically failed to be demonstrated by cholangiogram (13%), probably from minor ductules or from the gallbladder bed. Management of such injuries was done as shown in Table 2.
Biliary stricture group (174 cases)
Results of management of strictures by either endoscopy or surgery are shown in Table 3.
Percutaneous manipulations in biliary injuries
This approach was done in 32 patients, either in conjunction with endoscopy (rendezvous techniques) in 16 cases or with other percutaneous techniques in the rest of the cases, where it was therapeutic in 5, and prior surgery in the other 11 patients as shown in Table 4.
PTC, percutaneous transhepatic cholangiogram; PTD, percutaneous transhepatic dilatation.
Surgical treatment for biliary injuries
Surgery was attempted in 135 cases (Table 5), either urgently done in 30 patients with biliary peritonitis or electively in the rest. In 26 cases, it was only peritoneal drainage prior to further treatment; however, it was a definitive treatment in 109 cases, preceded by magnetic resonance cholangiopancreatography in 87 cases, percutaneous transhepatic dilatation in 5 cases, or percutaneous transhepatic cholangiogram in 6 cases.
Follow-up data
Post-procedure follow-up data were collected for all cases and are shown in Table 6.
The learning experience curve of ERCP and biliary reconstructive surgery
The endoscopic learning curve of the cumulative experience appeared progressively to be in direct proportion to increasing numbers of referral cases to the center (10–20 cases for ERCP per month in 2000 to 10–15 cases daily in 2010) with increasing numbers of successful cases (with an incidence of 60% at initial attempts of ERCP at 2000, reaching about 90%–95% in 2010). Experience was enhanced in 2003 by the introduction of percutaneous manipulation techniques that help to avoid failure of ERCP cases (e.g., difficult cannulation, dilatation of a tough tight stricture segment, delineation of the proximal biliary tree, and stenting for a stricture not reached by ERCP). Simultaneously, the learning curve of experience of surgical treatment also extended in a similar fashion with a cumulative manner for 10 years with treatment of such problems, with more than 76 operations of bilio-enteric shunt procedures in these challenging cases of relatively nondilated biliary channels, with sepsis and fibrous scarring of the field. Experience was revealed by decreasing complications, especially anastomotic stricture, which was encountered in early cases.
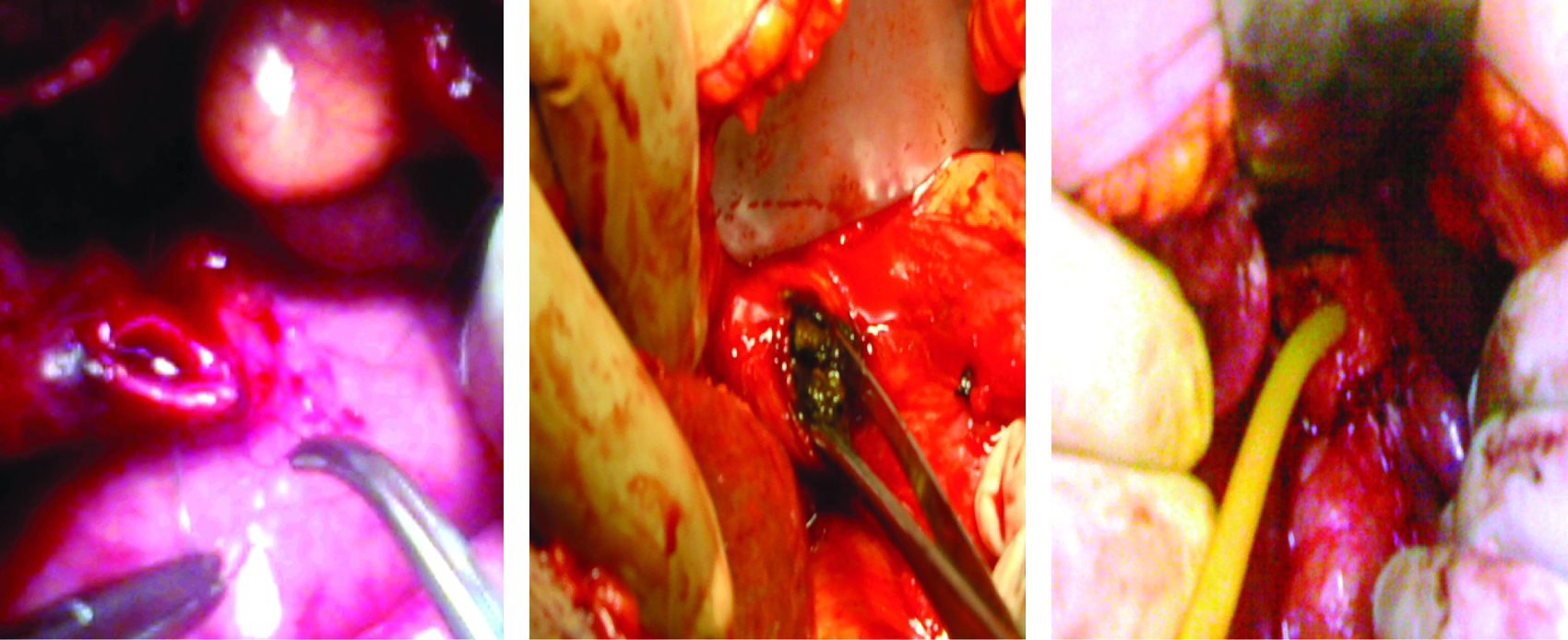
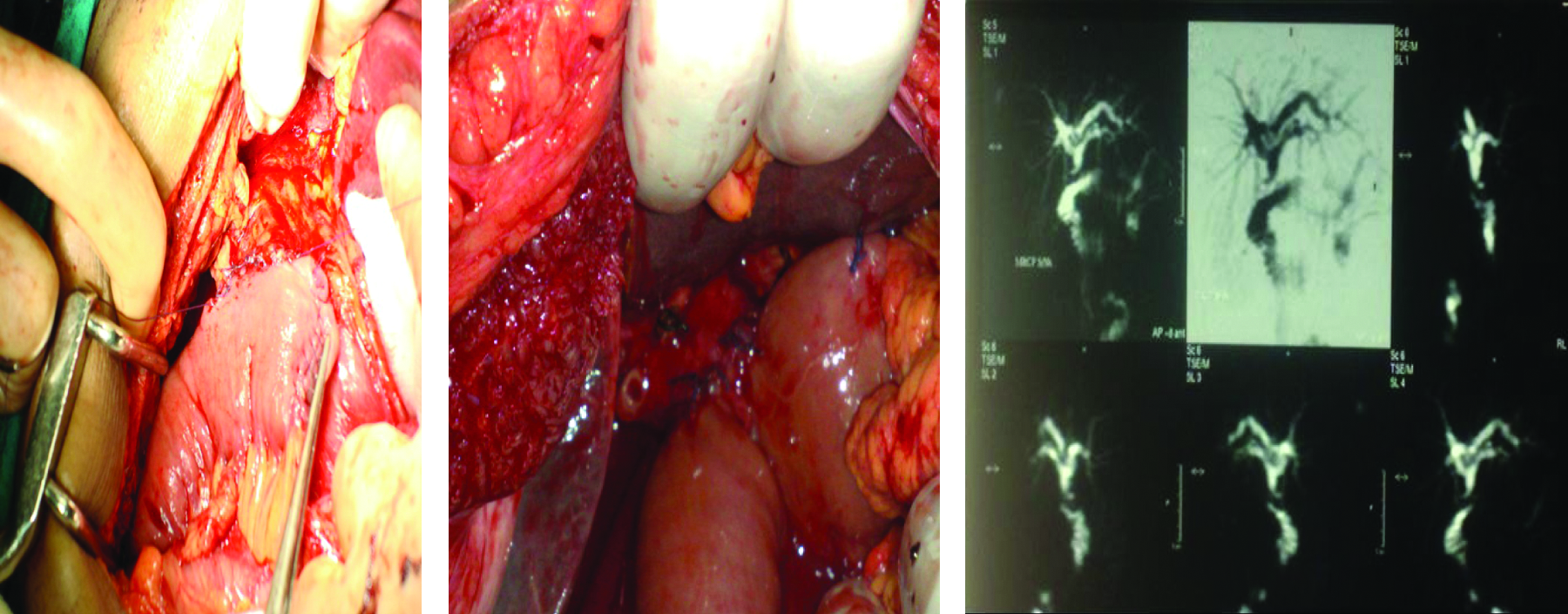
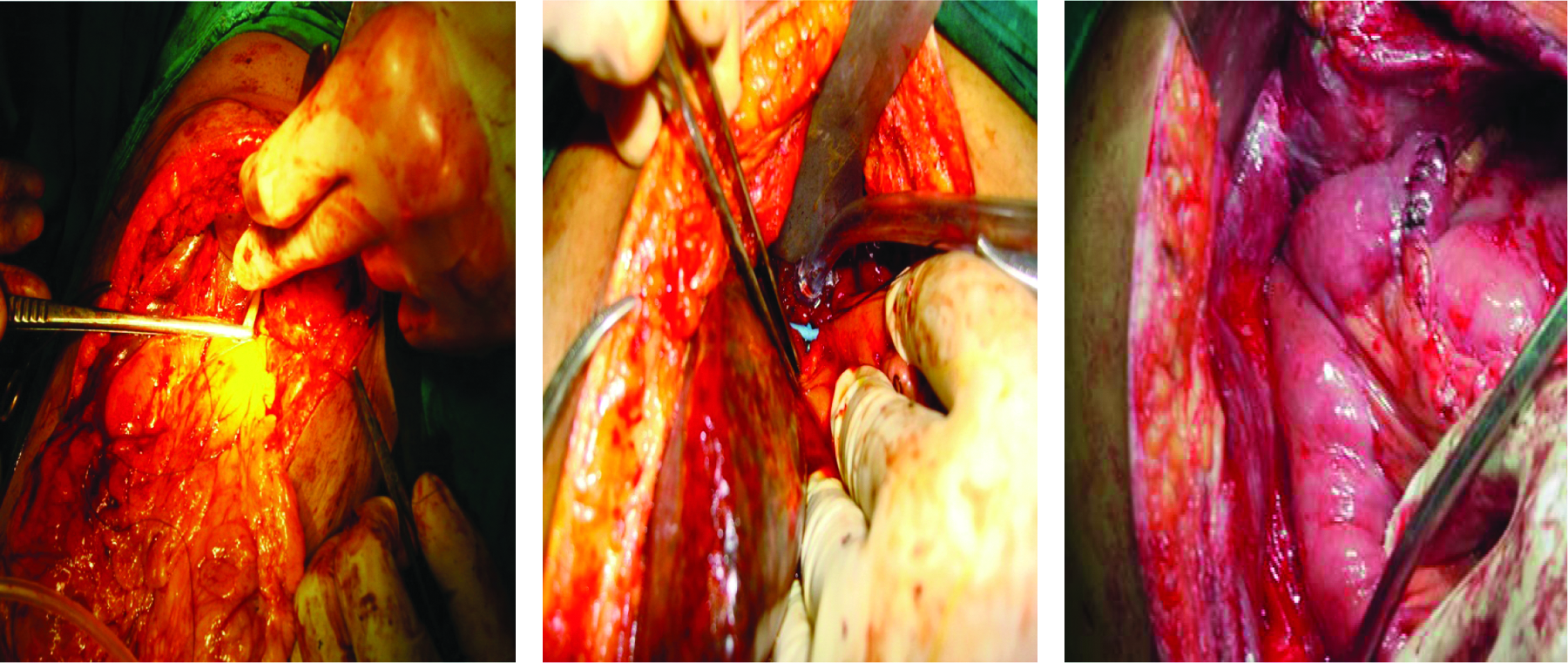
The various surgical and percutaneous techniques used in this case series are illustrated in Figures 1–11.
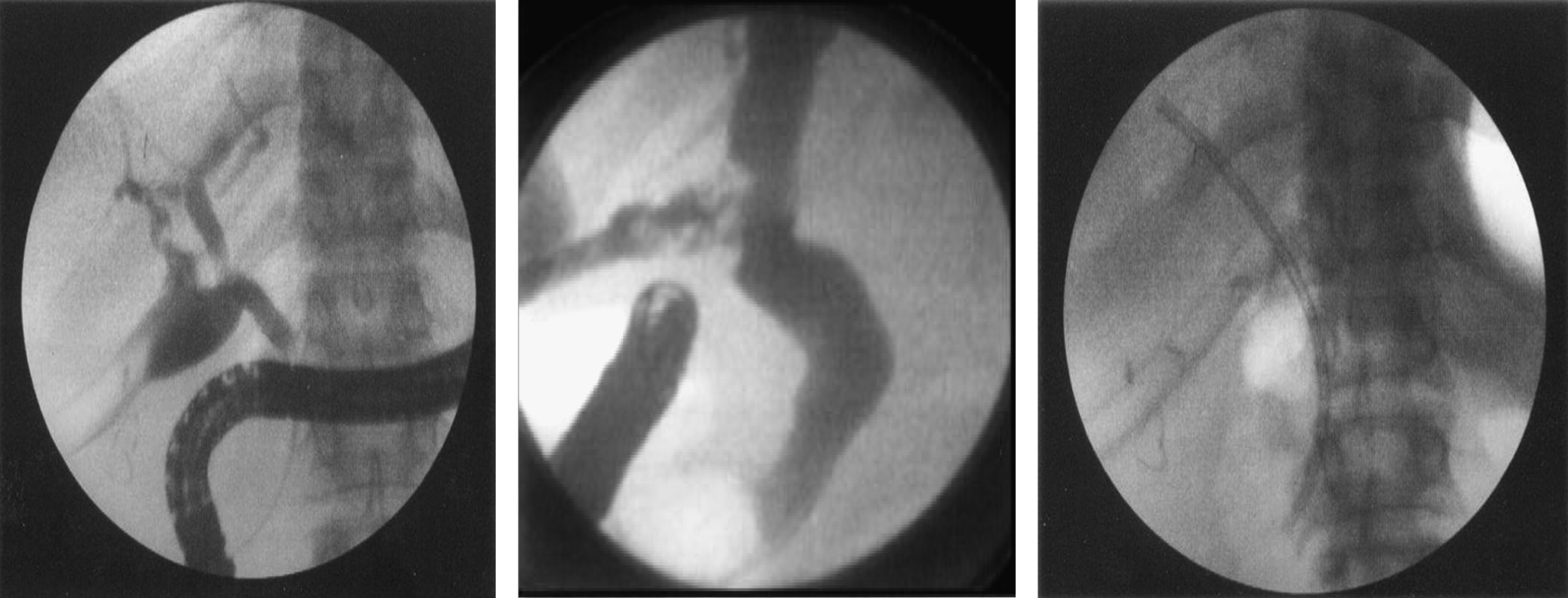
Endoscopic retrograde cholangiopancreatography showing biliary leakage, treated by sphincterotomy and stenting.
Endoscopic retrograde cholangiopancreatography showing a ligated common bile duct and a transected common bile duct with major leakage.

Endoscopic retrograde cholangiopancreatography showing common bile duct stricture treated by dilation and stenting.
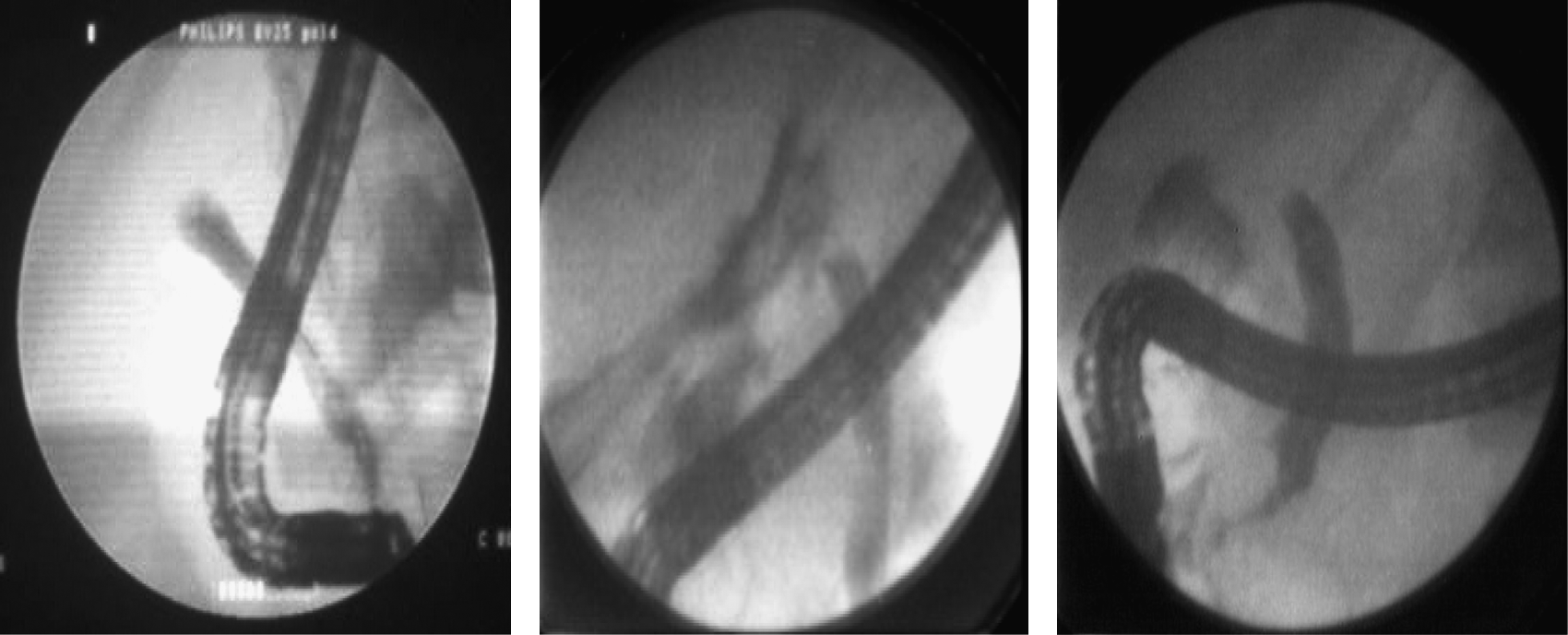
Rendezvous techniques with endoscopic stenting for common bile duct stricture.
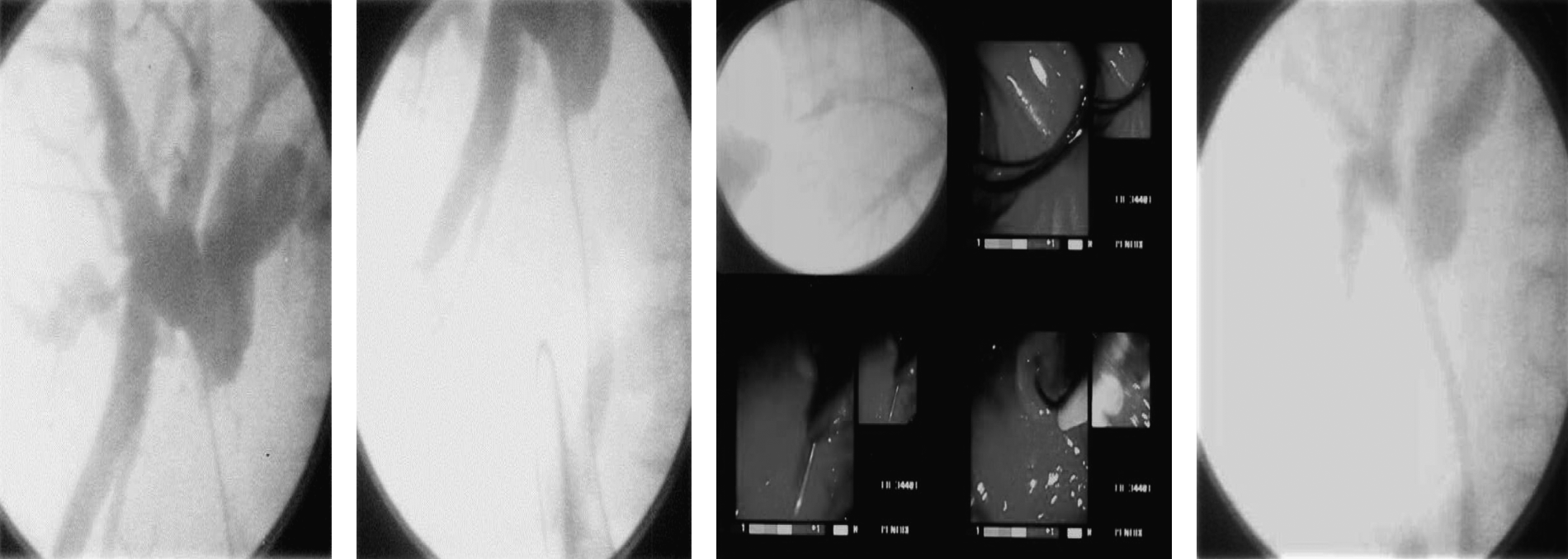
Percutaneous transhepatic cholangiogram for a ligated common bile duct and percutaneous transhepatic stenting for a postoperative anastomotic stricture.
Operative photograph of biliary injury and leakage, with a common bile duct stone, and repair over the T-tube.
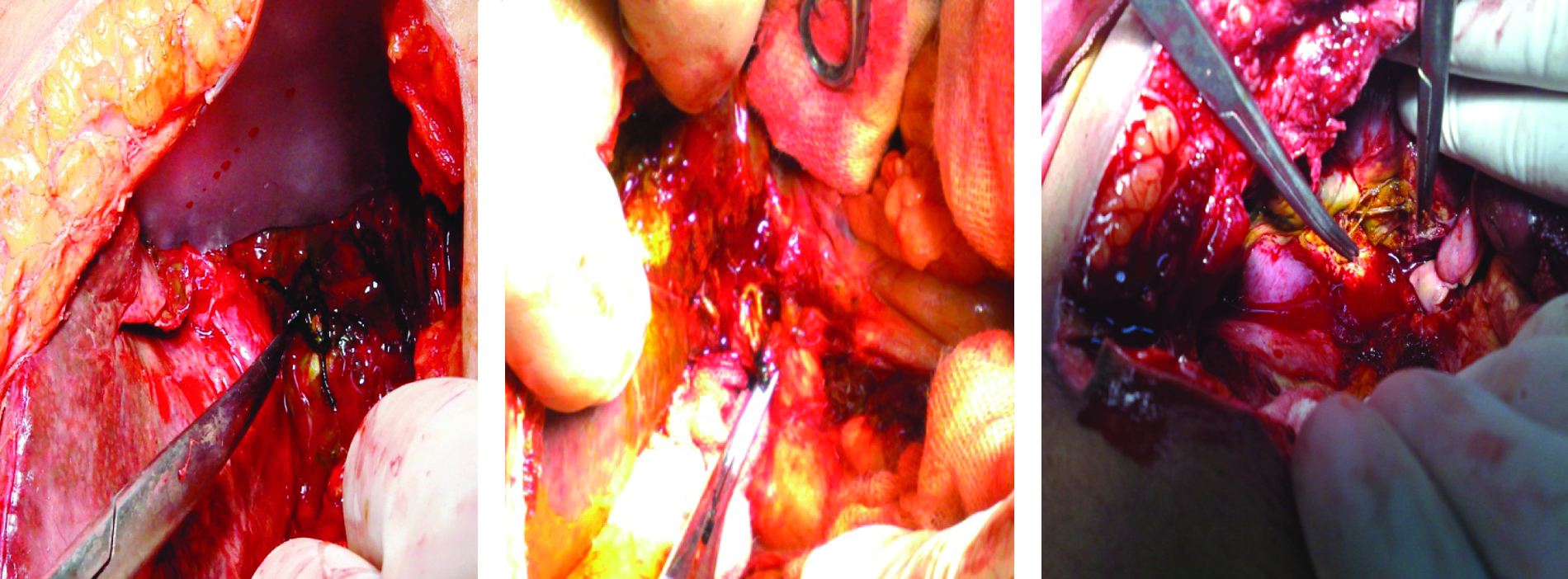
Operative field showing ligated, excised common bile duct, and field with many stitches in the porta hepatis.
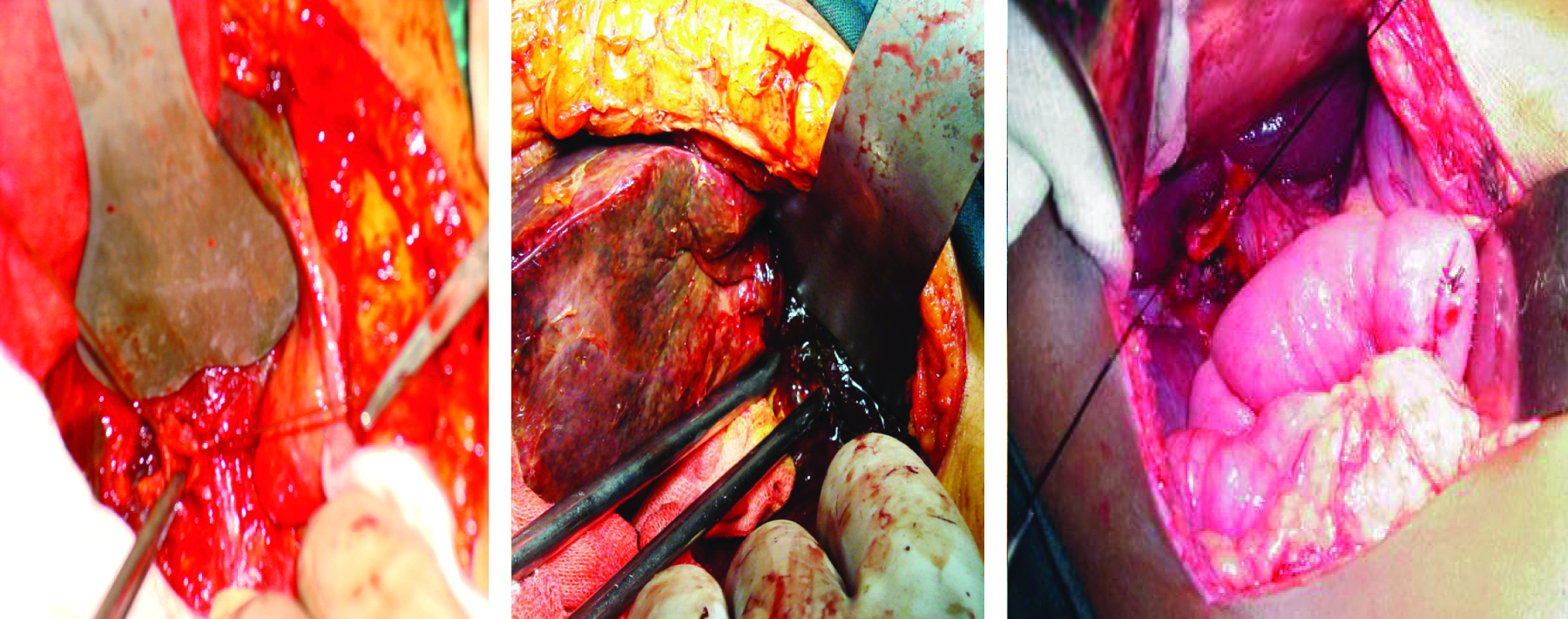
Operative dissection of hepatic ducts with Roux-en Y loop hepaticojejunostomy anastomosis.
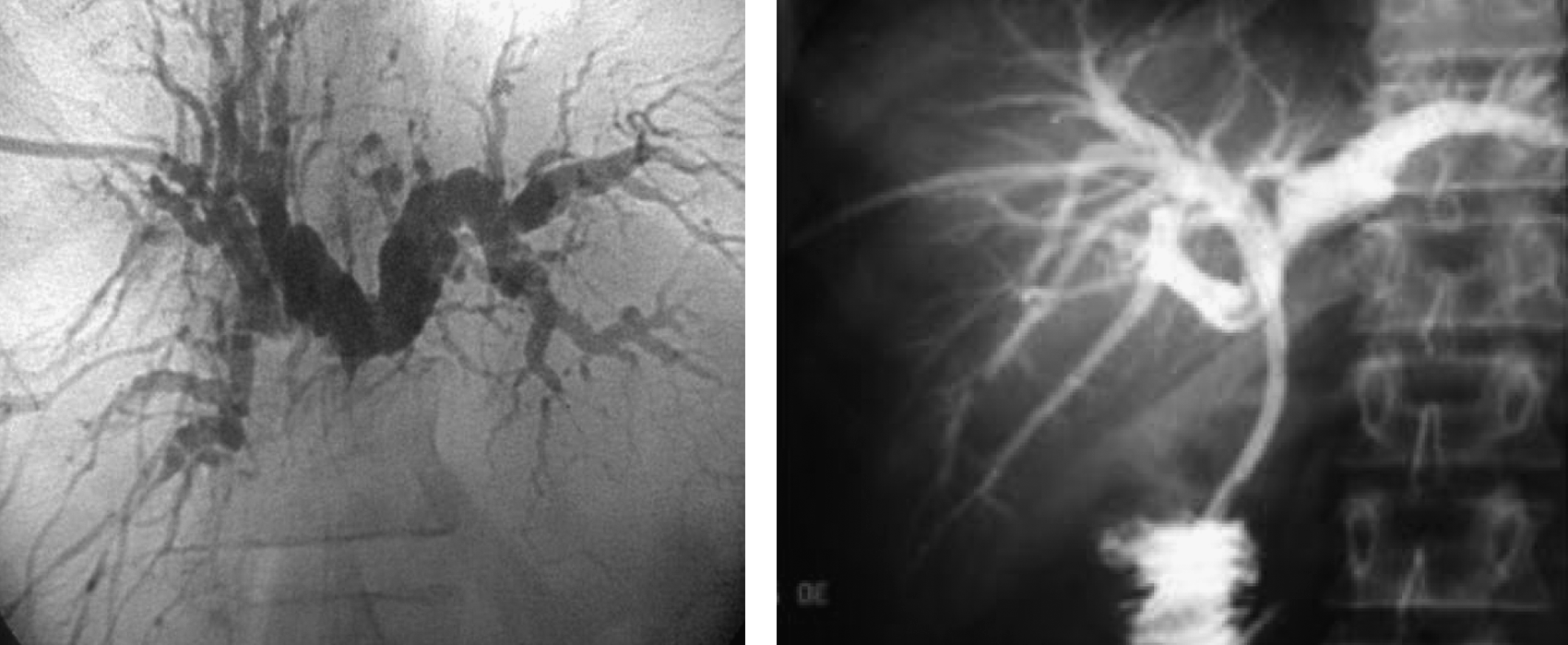
Roux-en-Y hepaticojejunostomy completed with postoperative magnetic resonance cholangiopancreatography assurance.
Roux-en-Y hepaticojejunostomy loop splinted by trans-anastomotic stents.
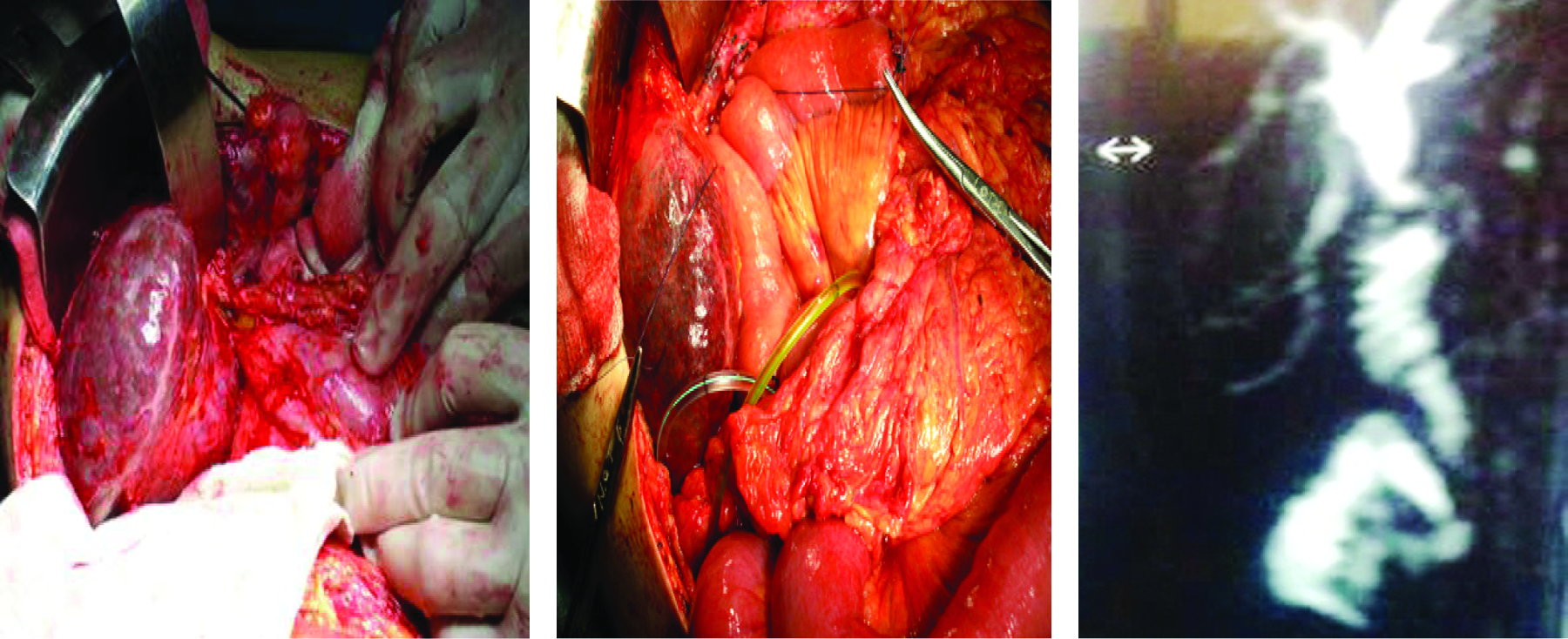
Operative picture for anastomotic stricture treated by repeat anastomosis and postoperative magnetic resonance cholangiopancreatography.
Discussion
The incidence of post-cholecystectomy biliary injury cannot be assessed as the total number of cholecystectomies done within this period is unknown, but the total number of injuries encountered in this work was higher after open cholecystectomy (317 cases) than after laparoscopic cholecystectomy (102 cases), in contrast to the generally accepted higher incidence after laparoscopic cholecystectomy (0.6%) more than after open cholecystectomy (0.3%). 3 This may be attributed to the low incidence and affinity for laparoscopic procedures in the Upper Egypt locality, and open cholecystectomy is still practiced in most district hospitals.
Bile leakage (245 patients)
Bile leakage was a common presentation among our patients (58.5%) and was seen as bile leakage in 204 patients or bile fistula in 41 patients. 5 Usually the leakage originated from the liver bed or biliary injury, as documented by previous studies, 22 and can be explained also as the sphincter of Oddi creates a pressure gradient that result in bile spillage to outside rather than into the duodenum. 23 Leakage was demonstrated by cholangiogram in most cases (226 of 245 patients); however, the spillage was very mild and not evident by contrast injection in 7.8% (19 cases). Such mild cases of biliary leak may resolve spontaneously according to the literature. 5
Endoscopic treatment was based on the degree of leakage. Patients with mild and moderate degree leakage were types A, B, C, and D in the Strasberg classification, with leaks from the cystic duct stump, the intrahepatic bile duct, the lateral section of the CBD/right hepatic duct, and gallbladder bed. It was treated efficiently by endoscopic sphincterotomy and stenting for at least a month as agreed by many reports11,24–27; subsequently leakage ceased within 3–5 days in most of cases in this work for mild and moderate leakage (19 of 19 and 75 of 80, respectively) with success rates of 100% and 94%, respectively. As explained in the literature, endoscopic treatment accelerates the healing period by decompressing the biliary system; in addition, it closes the defect physically and acts as a bridge at the site of extravasation. Stenting also acts as a mold and prevents stricture formation during the recovery period and should be the preferred treatment. 27
In major leakage (types D and E in the Strasberg classification), endoscopic treatment with sphincterotomy and stenting was successful in only 67% of cases (31 of 46). This incidence was comparable to other incidences reported in the literature.24,28–30 Moreover, another session of ERCP and stenting was needed to dilate a resulting stricture and upgrade stenting at a later date in 15 out of 31 patients treated; this result is also comparable with literature results. 27
A CBD stone was found to be exacerbating leakage in 65 cases and was successfully treated by sphincterotomy and stone extraction in conjunction with stenting in 60 patients with good results in agreement with other work.31,32 Also, CBD stricture was found with leakage and treated by appropriate bougies or balloon dilation and stenting in 12 of 17 patients, in agreement with findings by other authors.33,34 Unfortunately, the role of endoscopy is weak in CBD transection injuries with leakage as only 2 of 18 patients were endoscopically treated, in agreement with other studies demonstrating this low incidence of endoscopic treatment of such problems.26,30
Surgery was done urgently in 30 cases of biliary leakage complicated by biliary peritonitis as practiced by other authors.15,35 On the other hand, surgery was needed as elective surgery in 48 patients, especially after failure of other minimally invasive tools, and it was effective in ligation of slipped cystic ligature or clips, CBD repair over a T-tube splint, choledocholithotomy and CBD repair over a T-tube splint, and bilio-enteric anastomosis, which was done in 29 cases as the operation of choice as documented by most studies.20,36–39 Trans-anastomotic stent was done in 15 cases in this work with unhealthy (ischemic, or scarred) or small ducts (<4 mm) as practiced by other authors.20,40,41 Thus surgery was redone as the treatment of choice in spite of being used in only 31.8% of cases (78 of 245); without doubt it has its associated morbidity and mortality, prerequisites, and necessary facilities.
Good long-term surgical results are obtained with Roux-en-Y hepaticojejunostomy as documented in the literature.20,36–39 In this work, it was done with mucosa-to-mucosa, tension free, at least a 2-cm stoma, single-layer techniques using Vicryl 3/0 or 4/0, in conjunction with a trans-anastomotic stent selectively to guard against postoperative stricture complications.
Biliary stricture (174 cases)
Endoscopic treatment was successful in 118 patients (67.8%) with sphincterotomy, bougies or balloon dilation, and convenient stenting. It was performed in conjunction with CBD stone extraction in 11 of 19 patients and in repeated ERCP sessions to replace or subsequently upgrade the stent in 80 cases, in agreement with other previous reports that ERCP and stenting have comparable efficacy with surgery with lower rates of morbidity and mortality.30,33,34 So endoscopy is the preferable initial therapy,42,43 but it needs a long period (about 24 months) and repeated endoscopic sessions 26 with progressive increment in the number of stents to better calibrate the stricture. Stents should be replaced every 3 months before possible clogging could cause cholangitis, and the patient should be informed about the risk of stenting and the duration of treatment.18,44–46 Otherwise surgery is indicated as the treatment of choice, especially in surgically suitable patient. 26 However, Davids et al. 42 reported equal relapses of 17% for both treatment. Surgery was redone in 56 cases in this study (32.2%), for stricturoplasty, choledocholithotomy, and bilioenteric anastomosis, which was done in 47 patients.
Post-procedure mortality and morbidity and follow-up data
Fortunately, no death occurred after endoscopic treatment, 16 but some minor complications were seen as cholangitis, pancreatitis, stent clogging, and bad patient compliance. Unfortunately, two deaths occurred following surgery (one due to respiratory complications and one due to cirrhotic liver failure), as well as some complications such as wound infection, bile leaks, incisional hernia, and post-anastomotic stricture, which were encountered in 5 cases, with intrahepatic stones in 2 of them as documented in the literature that stenosis occurs in about 10% of cases.18,20,36,40,41 All complications were managed conservatively except incisional hernia and postoperative anastomotic stricture, which were treated by other tools. Anastomotic stricture was managed by percutaneous dilation and stenting in 3 of 5 cases as it is very beneficial in such cases as documented by other authors,47,48 and surgery was repeated in 2 patients.
Conclusions
Management of such problematic cases must be individualized as stated previously, 15 when the need for surgery becomes essential because of the nature of injury or of nonresponse to other forms of treatment. Surgery should be undertaken in a specialized unit with expert surgeons as the results are affected greatly by the learning curve, 14 and this was evident in this work by improvement of the results with time and experience accumulation in both endoscopy and surgery. Endoscopy is the preferable initial treatment18,44 that effectively managed most bile duct injuries 49 ; however, its use is limited to incomplete biliary strictures 26 and biliary leakage29,30,32 and for surgically unsuitable patients, 26 and, if successfully done, its results are similar to surgical results, 46 with less mortality. 16 But, surgery remain the gold standard treatment, especially in leakage with biliary peritonitis, ligated bile duct, complete biliary stricture, bile duct transection, or stricture after bilio-enteric anastomosis,15,42 as patients with total obstruction are not amenable to endoscopic approaches. 16
Footnotes
Disclosure Statement
No competing financial interests exist.