
Abstract
Abstract
Background:
Isolated torsion of the Fallopian tube, without ovarian torsion, is a rare cause of lower abdominal pain. We report our experience with 4 recent cases, along with data from a 20-year review of the pediatric literature.
Subjects and Methods:
The records of 4 cases encountered during a 3-year period were reviewed. A literature review was completed by searching Medline, Medline in Process, Embase, Current Contents, and BIOSIS from 1990 to 2010.
Results:
All 4 patients were diagnosed on laparoscopy. Laparoscopic salpingectomy was performed in 3 cases and laparoscopic detorsion in 1. All three resected specimens revealed hemorrhage and gangrene of the salpinx, with an associated cyst in one. The pediatric literature review, including our report, revealed 33 case reports and case series with 45 patients. Fifty-six percent of cases represented primary torsion, and 44% were secondary to underlying tubal pathology. Thirty percent of girls were premenarchal. The mean age at presentation and symptom duration were 13.2±2.1 years and 5.8±12.5 days, respectively. Fever and leukocytosis were present in 27% and 63%, respectively. Ultrasound, computed tomography scan, and magnetic resonance imaging showed a sensitivity of 22% (8/36), 14% (1/7), and 40% (2/5), respectively. A correct preoperative diagnosis was considered in only 13%. Eighty-eight percent of cases were treated by salpingectomy, and 12% were treated by tubal detorsion. Long-term outcomes of detorsion were not reported.
Conclusions:
Isolated salpingeal torsion in girls is rarely diagnosed preoperatively, regardless of imaging technique. Laparoscopy is the intervention of choice for definitive diagnosis and management. Salpingectomy is the most frequent treatment. Detorsion without resection may be considered for selected cases, but the long-term outcomes of this approach are unknown.
Introduction
Subjects and Methods
The study was triggered by 4 cases encountered during a 32-month period, September 2008–April 2011. One case (Case 1) was treated by the senior author (S.E.) in Long Beach, California. Per hospital policy, a letter was submitted to the Memorial Health System Research Administration informing them of the chart review for publication purposes. The other 3 cases were treated at the Montreal Children's Hospital: 2 by S.E. and 1 by J.M.L. Per hospital policy, the Director of Professional Services approved the retrospective chart review of all 3 patients (protocol 2011-25).
A literature review was completed using the following databases: Medline, Medline in Process, Embase, Current Contents, and BIOSIS. The key words used were “Fallopian tube,” “uterine tube,” “oviduct,” “salpinx,” “torsion abnormalities,” and “torsion.” The search was conducted on articles from 1990 to the present and limited to the English language and the pediatric population (0–18 years of age).
Results
Case series
Case 1
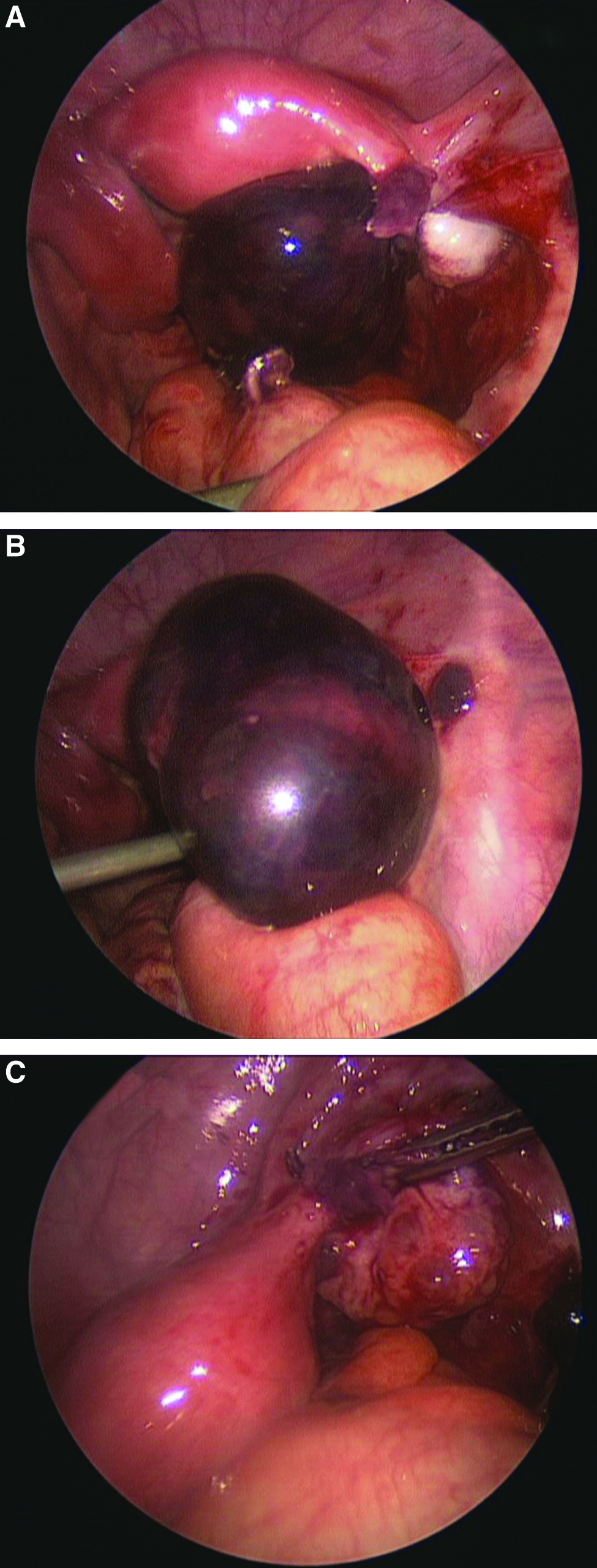
A 13-year-old, previously healthy, recently menarchal girl presented with a 3-day history of abdominal pain, gradually intensifying and localizing to both lower quadrants. The pain was accompanied by nausea, vomiting, dysuria, and diarrhea. Her last menstrual period was 4 weeks prior to presentation. The patient was afebrile, and her abdomen was diffusely tender to palpation but more prominently in the right lower quadrant. Peritoneal signs were elicited. Laboratory work-up revealed a white blood cell count of 14×103/μL and a normal β-human chorionic gonadotropin level. Ultrasound imaging revealed a thickened appendix. The patient underwent laparoscopy for presumed appendicitis. At laparoscopy, a large, torsed, hemorrhagic, gangrenous right Fallopian tube, with a normal ipsilateral ovary and contralateral adnexae, was seen (Fig. 1). A laparoscopic detorsion followed by right salpingectomy was performed, using an endostapler (Fig. 1). Histopathological examination revealed extensive diffuse congestion and hemorrhage of the Fallopian tube consistent with torsion, with no associated lesions. The patient was discharged the following day and was asymptomatic on 2-week follow-up.
Case 1.
Case 2
A 13-year-old, previously healthy, recently menarchal female presented with a 5-day history of intermittent abdominal pain migrating to the right lower quadrant, occasionally associated with nausea and vomiting. Her last menstrual period was approximately 4 weeks prior to presentation. The patient was afebrile, with mild rebound tenderness in the right lower quadrant. Laboratory work-up revealed a white blood cell count of 11×103/μL and normal β-human chorionic gonadotropin. Pelvic ultrasound revealed a moderate amount of free fluid and did not visualize the appendix. A computed tomography (CT) scan revealed a 5-cm complex lesion in the pouch of Douglas, without calcification or fat stranding, interpreted as a pelvic abscess versus complex paraovarian mass. On laparoscopy, the appendix appeared mildly inflamed secondary to contact with a large, gangrenous, torsed right Fallopian tube with a normal right ovary. The left tube and ovary were normal. We proceeded with a 360° counterclockwise detorsion, which allowed us to isolate a narrow pedicle, amenable to control with two endoloops. Histopathological examination confirmed the intraoperative diagnosis of IST and revealed hemorrhagic and ischemic changes of the Fallopian tube without an associated lesion. The patient was discharged the following day and was asymptomatic on 2-week follow-up. She did not present to our hospital with any further episodes of abdominal pain over the ensuing 3 years.
Case 3
A 13-year-old previously healthy premenarchal girl presented with a 3-week history of intermittent severe right lower quadrant pain. Laboratory work-up revealed a white blood cell count of 11.5×103/μL and normal β-human chorionic gonadotropin. An ultrasound demonstrated a complex adnexal cyst measuring 5.7×3.8×4.2 cm, thought to be of ovarian origin. There was no evidence of calcification or significant solid component. The pain spontaneously resolved, and she was discharged with a planned follow-up. On follow-up ultrasound 2 weeks later, there was no change, and the patient continued to be asymptomatic. Observation was continued. However, several days later, the patient presented with recurrent symptoms. She was afebrile and had right lower quadrant tenderness to deep palpation without rebound tenderness. A third ultrasound showed persistence of the adnexal mass, and the patient proceeded to laparoscopy. An ischemic, torsed, right Fallopian tube was seen with at least three twists of the pedicle, without ovarian involvement (Fig. 2). The proximal portion of the tube appeared to be spared (Fig. 2). The tube was detorsed with improvement in its appearance. The tube was dilated and filled with clots but otherwise appeared nonpathologic. The surgeon elected not to perform a resection. The patient was discharged on the second postoperative day and was asymptomatic at 2-week follow-up. She has not presented again with any symptoms to our hospital during the 18 months following the procedure. Unfortunately, she missed multiple appointments for a follow-up ultrasound.

Case 3.
Case 4
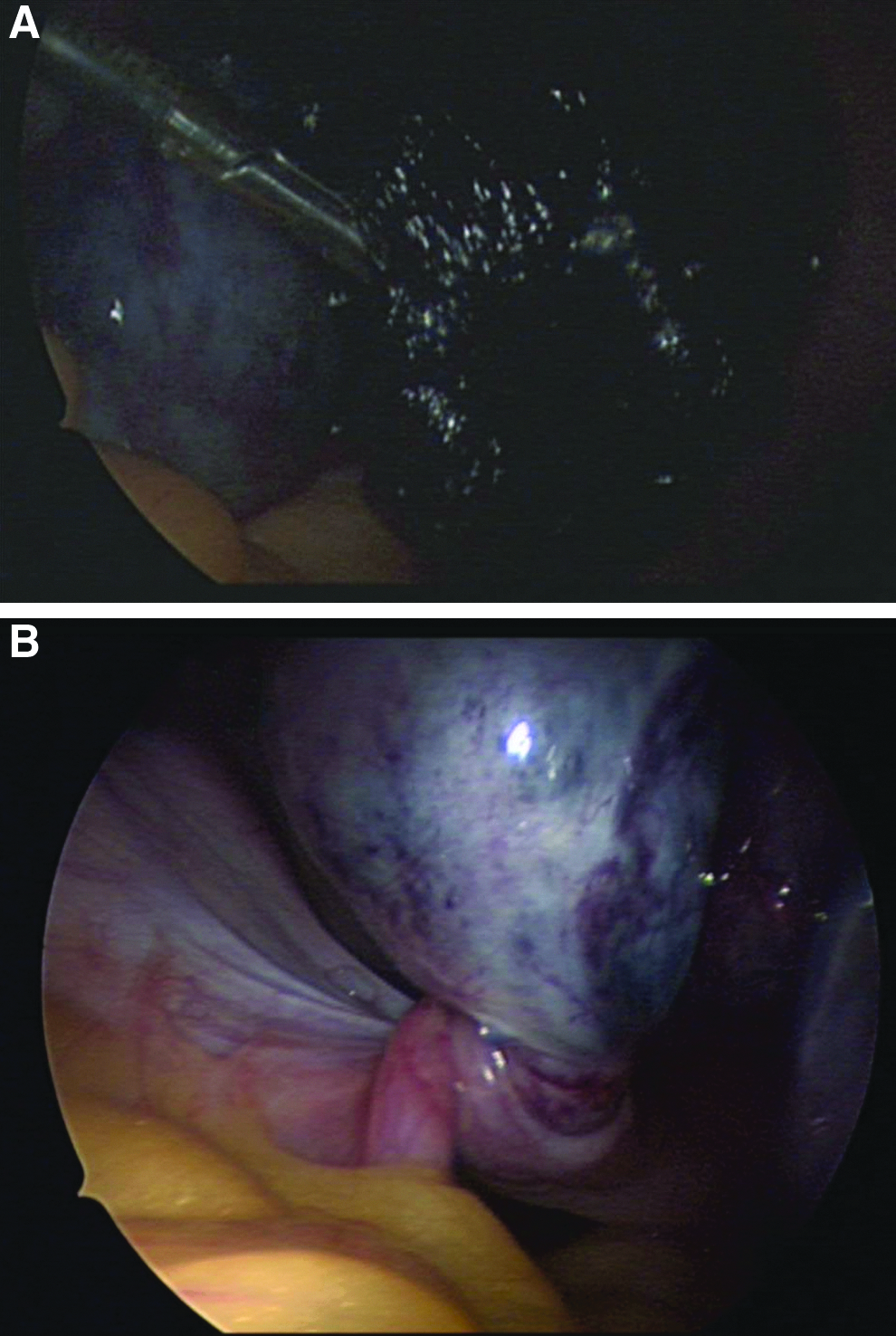
A 15-year-old morbidly obese girl presented with left lower abdominal pain for 24 hours, associated with nausea and vomiting. She was menstruating at the time of presentation. The patient was afebrile with left lower quadrant tenderness to deep palpation but no rebound tenderness. Laboratory investigations revealed an elevated white blood cell count of 15.9×103/μL and normal β-human chorionic gonadotropin. An abdominal ultrasound showed a large adnexal mass. A CT scan revealed a cystic mass to the right of the midline, in between the ovaries, superior to the bladder, measuring 12×7×10 cm (Fig. 3). At laparoscopy, a hemorrhagic pelvic mass was seen, consisting of a very large paratubal cyst that had caused 720° torsion of the left Fallopian tube along with the ovary (Fig. 4). The tube and associated cyst appeared grossly necrotic. Although the left ovary appeared hemorrhagic and ischemic, it regained its normal color upon detorsion. The paratubal cyst was decompressed, releasing a large amount of clear fluid. An endostapler was then used to transect the tube and attached cyst, while preserving the ovary. The right adnexa, tube, and uterus were normal with no other identifiable pathology. Histopathological examination confirmed a simple paratubal cyst in addition to hemorrhagic necrosis of the Fallopian tube consistent with torsion. On a 2-week follow-up, the patient was asymptomatic. She has not presented to our hospital with any further episodes of abdominal pain during the 8 months following the procedure.

Case 4. Computed tomography scan showing a large cystic mass slightly to the right of the midline and superior to the bladder.
Case 4.
Literature review
The pediatric literature review, including our report, revealed 33 case reports and case series2,4–34 of IST with a total of 45 patients. We classified IST as primary when no associated congenital or acquired lesions of the tube were identified during surgery or on histopathologic examination and secondary when such lesions were identified. Although congenital anatomic anomalies, such as an elongated tube, have been previously described as potential predisposing factors for torsion, we did not consider this secondary torsion. With this classification, 25 cases (55.6%) represented primary IST, whereas 20 cases (44.4%) were secondary to underlying adnexal pathology. Menstrual history was available for 40 patients, 30% of whom were premenarchal and 70% were menarchal. The mean age at presentation was 13.2±2.1 years, with the youngest patient reported being 4 years old. 8 The chief presenting symptom was abdominal pain in all patients, localized to the right lower quadrant in 13 (39.4%), left lower quadrant pain in 12 (36.4%), and nonspecific in 8 (24.2%). The laterality of the pain corresponded to the side of torsion in all patients with localization. Nausea, vomiting, or both were associated findings in 24 patients (53%). The mean symptom duration prior to presentation was 5.8 days, with a minimum of 2 hours and a maximum of 2 months. Chronic tubal torsion was reported in 2 patients,11,28 presenting with intermittent abdominal pain for several months.
Nine febrile patients (27%) were identified, with an average temperature of 38.0±0.5°C on presentation. Seventeen patients (63%) had documented leukocytosis with a mean white blood cell count of 15.5±4.8×103/μL. On ultrasound, a tortuous tube or a tubular structure was identified in 8 patients,5,6,11,13,22,26,27,33 representing a sensitivity of 21.6% in identifying a tubal abnormality. Adnexal cysts or masses were the most common finding on ultrasonography, seen in 28 of 37 patients (75.7%). Doppler ultrasound, done on 2 patients,22,30 revealed “no blood flow” in both of them. Only 1 of 7 patients who had a CT scan17,19,26,29 was suspected to have tubal torsion based on imaging, representing a sensitivity of 14.3%. Magnetic resonance imaging was performed on 5 patients,5,15,19,28,34 of whom 25,34 demonstrated suspicion of tubal torsion, representing a sensitivity of 40%; however, evidence of tubal pathology was identified on ultrasound on the same 2 patients. A correct diagnosis was made preoperatively by imaging in only 6 patients (13.3%); the remainder was diagnosed at surgical exploration (84.4%), and, in 1 case, the diagnosis was made by histopathological examination. 18
Torsion of the Fallopian tube was right-sided in 25 patients (59.5%) and left-sided in 17 (40.5%). Laparoscopy was used for diagnosis and treatment in 28 patients (78%), with conversion to laparotomy in 5. Laparotomy was the operative approach in 8 patients (22.2%). Salpingectomy was by far the most common surgical intervention, performed in 38 cases (88.4%). Fallopian tube salvage with detorsion was accomplished in 5 cases (11.6%).
Discussion
IST is very rare in the pediatric population, with only 45 cases reported in the literature over the past 20 years. The first case in a child was reported by Hansen 35 in 1922 and cited by Blum and Sayre 36 in 1937. As depicted in our patients and in the literature review, the clinical presentation of tubal torsion has no pathognomonic features, with the only consistent symptom being lower abdominal pain. The high incidence of nausea and vomiting represents a common visceral response to torsion and further serves to confuse this entity with acute appendicitis. Diarrhea and dysuria, if present, typically represent irritation from a pelvic hemorrhagic or necrotic process. Fever is uncommon, but mild leukocytosis is frequent. A history of spontaneously resolving pelvic pain and presentation during or close to the time of menstruation are perhaps the only symptoms that increase the likelihood of IST.
Our review identified two reports of chronic tubal torsion.11,28 Chronicity is thought to be an outcome of alternative phases of mild spontaneous torsion and detorsion. 28 Atypical presentations have also been described. IST may mimic presentation of Müllerian duct anomalies with severe unilateral pelvic pain and a pelvic mass. 15 Maynard et al. 11 reported on a case mimicking pelvic inflammatory disease, with a palpable mass, vaginal discharge, and fever. Kopec et al. 34 reported an IST associated with a congenital uterine anomaly and ipsilateral renal agenesis. Karcaaltincaba et al. 24 reported a Fallopian tube torsion following trauma through a broad ligament tear. Raziel et al. 13 reported the first case of recurrent salpingeal torsion 2 years following the initial incident.
The extent and duration of torsion generate a spectrum of pathophysiologic alterations. Initially, venous return is perturbed, leading to engorgement and thrombosis. If torsion is unrelieved, arterial occlusion ensues, leading to necrosis and gangrene and increasing the risk for hemoperitoneum, superinfection, and peritonitis.2,5,37 Treatment is also indicated to relieve the acute pain associated with the condition. Potential predisposing factors for IST were first reported by Youssef et al. 38 and supported by Provost 39 and Filtenborg and Hertz. 40 These factors include intrinsic as well as extrinsic mechanisms. Intrinsic factors include anatomical malformations such as a long tube and mesosalpinx, hydatids of Morgagni, hydrosalpinx, hematosalpinx, tubal neoplasm, and physiological disturbances resulting in mesosalpingeal venous congestion and alteration of the normal peristalsis of the Fallopian tube. Extrinsic factors include abnormalities in the neighboring organs, such as ovarian and paraovarian masses, uterine enlargement due to tumors or pregnancy, peritubal adhesions, sudden changes in body position, trauma, and previous tubal surgery such as tubal ligation.2,16 In our review, paratubal cyst was the predisposing lesion in one of our 4 cases and in 9 reported cases,2,23,26,29,32 while paraovarian cysts were reported in 4 patients.9,20,26 These lesions represented approximately 70% of adnexal pathologies predisposing to torsion. Paratubal cysts or hydatid cysts of Morgagni, thought to be Wolffian duct remnants, are usually attached by a small pedicle to the fimbriated end of the Fallopian tube. As the cyst grows the tube becomes heavier and more prone to rotation. They are typically simple cysts, benign in nature, and rarely exceed 1 cm in diameter. Salpingeal torsion with evidence of paratubal cysts on the contralateral tube has been reported in 3 patients.11,22,32 Following gangrenous degeneration of a twisted tube, some pathologies such as paratubal cysts may not be evident on histologic examination, falsely decreasing the incidence of secondary torsion. Unlike omental torsion, IST does not appear to be associated with obesity.
IST is reported to have a right-sided predilection with a right-to-left ratio of 3:2–2:1. Our review supports this predilection, which has been attributed to the cushioning effect of the sigmoid colon and the slightly longer right mesosalpinx and to the more frequent exploration of patients with right lower quadrant pain for presumed appendicitis.2,13,26 In some reports, IST appeared more frequently during the premenstrual phase because of the congestion of the mesosalpingeal veins at that time.2,6 In our series, the three menarchal girls were expecting their menses around the time of presentation.
Tekant et al. 41 reported on isolated torsion of accessory Fallopian tubes in two premenarchal girls. This very rare adnexal lesion is diagnosed and managed like IST. However, in view of the high incidence of bilateral accessory tubes, a detailed exploration of the contralateral adnexa has been recommended with excision of accessory tubes, if found. Some reports attribute the absence of a Fallopian tube to asymptomatic or missed tubal torsion10,23 or even an antenatal event.42,43
Numerous imaging modalities have been described to aid in the preoperative evaluation of IST in the pediatric population, including ultrasound with or without Doppler, CT, and magnetic resonance imaging. Conventional ultrasonography, typically the first-line investigation for abdominal pain in girls, may occasionally point to a diagnosis of IST, as supported by our review. Strong suspicion should be raised if the following triad is present6,16: (1) a long tubular, convoluted cystic structure that tapers toward the uterine cornua; (2) a thin-walled cystic structure with variable septations and mixed internal echoes, suggestive of hydrohematosalpinx; and (3) visualization of a normal ipsilateral ovary. Other findings include a cystic mass located in the midline, either in the cul-de-sac or superior to the uterus, and a deviated uterus toward the side of the torsion secondary to shortening of the tube.26,29 Color Doppler ultrasonography may demonstrate unilateral absence of blood flow (high impedance waveform with reversal of diastolic flow corresponding to the torsed adnexa).16,33 However, the presence of normal blood flow does not necessarily rule out tubal torsion. 44
The value of CT and magnetic resonance imaging in diagnosing IST has been controversial. Some reports advocate its usefulness in detecting a twisted vascular pedicle, thickened Fallopian tubes, and hemorrhagic infarction, 45 as well as rarely associated congenital uterine anomalies. 34 Others15,27 regard them as unnecessary interventions adding little, if any, detail to what is visualized on ultrasonography as well as resulting in unnecessary delay to surgical intervention. Two of our 4 patients underwent CT scans without the ability to make the correct diagnosis. Laparoscopy appears to be the “gold standard” for establishing the diagnosis and allows concurrent treatment with minimal morbidity. Laparoscopic detorsion can be completed using two graspers, and the pelvis and adnexae can be visualized accurately to rule out additional pathology. The surgeon will then need to decide whether to resect or preserve the tube. The majority of patients reported underwent salpingectomy, but there are no large outcome studies evaluating both options. Laparoscopic resection with ovarian preservation can be easily accomplished using standard techniques. Because the pathology is uniformly benign in children, aspirating associated cysts or breaking the specimen within a retrieval bag limits the need to convert or enlarge laparoscopic incisions. As opposed to ovaries, which are known to recover from severe ischemia, the outcomes of tubal ischemia are not known. Concern that scarring and adhesions may form, possibly increasing the risk of ectopic pregnancy, has led most authors to recommend salpingectomy. In cases of secondary IST, a third option may be resection of the associated pathology, such as a paratubal cyst, while preserving the tube. However, this has not been reported in the literature.
Laparoscopic intervention for IST in a child was first been reported by Maynard et al. 11 in 1996. Detorsion of the tube, without resection, was first reported by Kurzbart et al. 8 This is typically performed in cases of recent onset or incomplete torsion, when there is evidence of potentially viable tubal tissue.46,47 Promising results were reported following adnexal detorsion.48–51 In 1962, Blair 48 reported bilateral patent tubes on salpingography and subsequent normal pregnancy in a woman in whom the twisted tube was saved. Despite the theoretical risk of pulmonary embolism following detorsion and thrombosis of the tubal vascular supply, there is no evidence supporting this hypothesis. The incidence of pulmonary embolism following adnexal resection has been shown to be in fact the same as following adnexal detorsion, estimated at 0.2%. 52 Fixation of the tube may, at least in theory, alter the normal anatomy of the pelvis by either moving the adnexa outside the pelvis or distorting the delicate relationship between the tubal fimbria and the ovary. 13 Nevertheless, some have advocated tubal fixation. 16 A period of observation after detorsion in the operating room is warranted. The surgeon should strongly consider resection if there is frank necrosis of the tube without evidence of vascular recovery, or if there is an associated lesion. Girls treated by detorsion without resection should be investigated with follow-up ultrasound to document resolution of the cystic process. A hysterosalpingogram may be considered prior to initiation of sexual intercourse to evaluate the tube for patency. Unfortunately, the single patient who underwent detorsion without resection in our series was noncompliant with follow-up and never returned for tubal evaluation. All girls treated for IST, whether by salpingectomy or detorsion only, should be instructed to seek urgent medical attention for lower abdominal pain to minimize a missed recurrence and potential compromise of fertility.
In conclusion, IST in girls is rarely diagnosed preoperatively, regardless of imaging technique. It should be considered within the differential diagnosis of lower abdominal pain in a female, particularly if presenting close to the time of menstruation and associated with a pelvic or adnexal mass on imaging. Laparoscopy is the intervention of choice for definitive diagnosis and management. Salpingectomy has been the standard treatment if a clearly necrotic tube is found, nonreversible ischemia is seen, or there is evidence of secondary IST. Laparoscopic detorsion without resection may be considered for selected cases, but the long-term outcomes of this approach are unknown.
Footnotes
Disclosure Statement
No competing financial interests exist.