
Abstract
Abstract
Purpose:
Performing laparoscopic nephrectomy in the setting of previous renal surgery may be challenging and associated with a higher complication rate. We conducted this study to assess the feasibility and safety of laparoscopic nephrectomy among patients with a history of ipsilateral renal surgery.
Patients and Methods:
We reviewed the chart of 193 patients who underwent transperitoneal laparoscopic nephrectomy for nonfunctioning kidney between April 2007 and March 2011. The study population was divided into two groups: Group 1 comprised 37 patients with a history of ipsilateral renal surgery, and Group 2 consisted of 156 patients with no history of previous renal surgery.
Results:
Baseline characteristics and preoperative variables were similar in both groups. Mean operative time, complication rate, and hospital stay were comparable between the two groups. A nonstatistically significant trend toward a higher transfusion rate was noted in Group 1 patients. The operation was converted to open nephrectomy in 1 (2.7%) and 3 (1.9%) patients of Groups 1 and 2, respectively (P=.765).
Conclusions:
Laparoscopic nephrectomy of the nonfunctioning kidney is a feasible and safe procedure in the setting of previous renal surgery and is not associated with a significant increase in operative time and complication rate compared with patients with no prior ipsilateral renal surgery.
Introduction
We performed this study to compare the overall outcome of the LN between patients with prior history of ipsilateral renal surgery and those without previous history of renal surgery.
Patients and Methods
Study population
Between April 2006 and March 2011, 1055 patients underwent LN in our institution (Fig. 1). Patients who underwent LN for renal tumor or kidney donation were excluded from the analysis, and charts of 193 patients who underwent LN for a nonfunctioning kidney were reviewed. The study population was divided into two groups: 37 patients had a history of either percutaneous or open ipsilateral renal surgery (Group 1), and 156 patients had no history of previous renal surgery (Group 2). The target renal unit was confirmed to be nonfunctioning if the split renal function was less than 10% in 99mTc dimercaptosuccinic acid renal scan. Patients with obstruction in the affected renal unit underwent the 99mTc dimercaptosuccinic acid scan with a delay of 3–6 weeks after decompression. History of prior abdominal surgeries, other than ipsilateral renal surgery, was also evaluated as it may be associated with intra-abdominal adhesions. The Institutional Review Board approved the study.
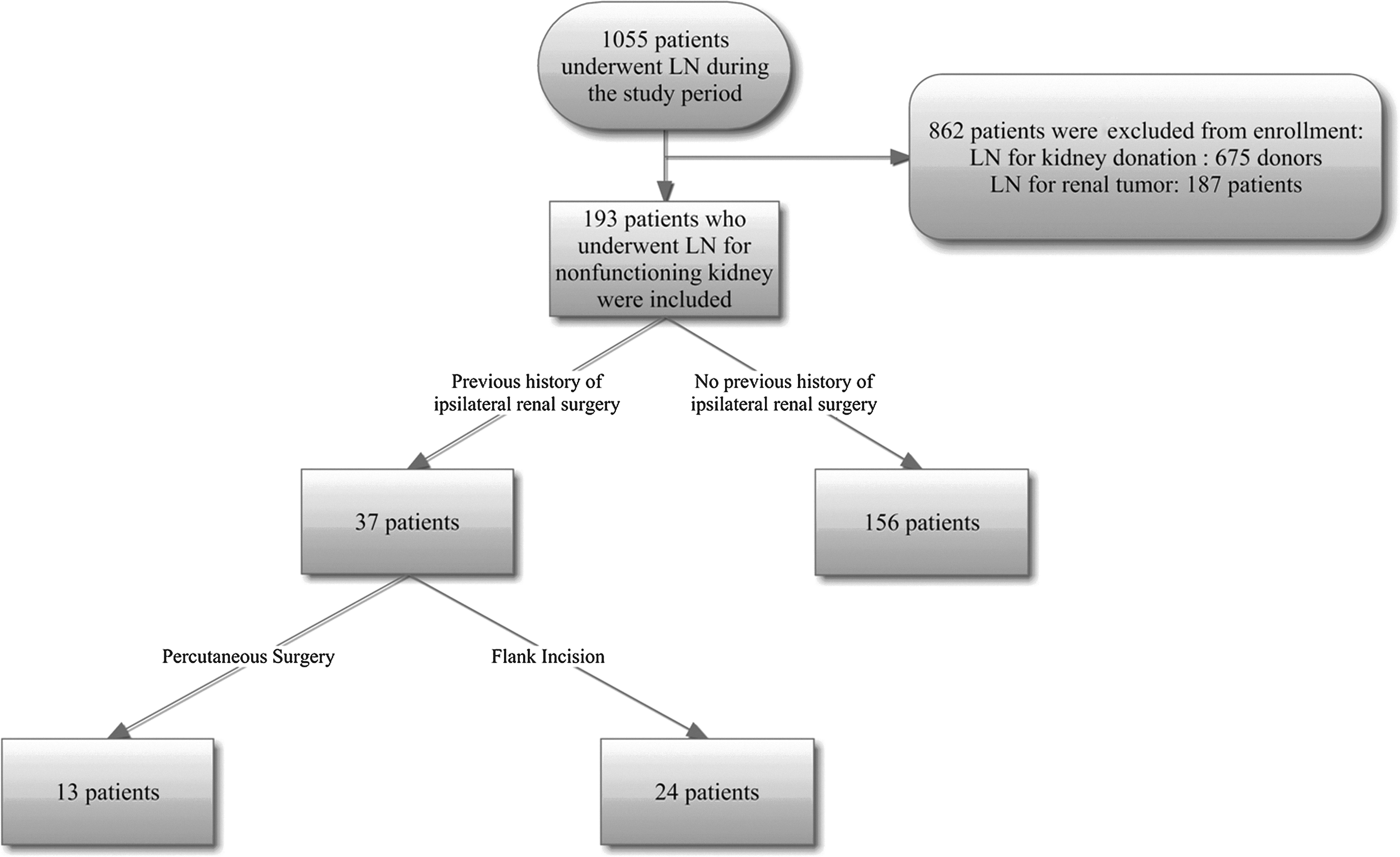
Flow chart of examination of patients in this study.
Surgical technique
Under general anesthesia the patients were placed in a modified lateral position with 15° posterior rotation. The transperitoneal approach was used in all patients. A 12-mm trocar, as the camera port, was inserted through the umbilical incision with the open access technique. In obese patients the camera port was inserted along the pararectal line. To perform a left side nephrectomy, two 5-mm trocars were inserted along the midclavicular line, 2 cm beneath the costal margin and below the level of the umbilicus. A 10-mm trocar was also placed in the anterior axillary line, halfway between the costal margin and the iliac crest. In the case of a right side nephrectomy, a 10-mm trocar was placed along the midclavicular line, 2 cm beneath the costal margin, while the 5-mm trocar was applied in the anterior axillary line, halfway between the costal margin and the iliac crest. After mobilization of the colon medially, renal vessels were exposed and dissected. The renal vessels were double-ligated with Hem-o-Lok® (Weck Surgical Instruments, Teleflex Medical, Durham, NC) clips separately. The ureter was divided, and the kidney was mobilized outside Gerota's fascia and extracted through a Pfannenstiel incision.
Statistical analysis
Statistical analysis was performed using SPSS (Chicago, IL) version 12 software. Comparison of quantitative data was performed using independent and paired t tests, and when the data were not normally distributed according to the Kolmogorov–Smirnov test we applied the Wilcoxon or Mann–Whitney test. Qualitative data were also compared using chi-squared or Fisher's exact test with two-tailed P<.05 considered statistically significant.
Results
During the study period, a total of 193 patients with a mean±standard deviation age of 41.2±16.5 years underwent LN for a nonfunctioning kidney including 37 patients with prior history of ipsilateral renal surgery (Group 1) and 156 patients with no history of previous renal surgery (Group 2). Nephrectomy was indicated based on the presence of intractable pain, uncontrolled hypertension, and recurrent urinary tract infections. In addition to ipsilateral renal surgery, 9 (24.3%) patients in Group 1 also had a history of other abdominal surgeries, including appendectomy, hysterectomy, cholecystectomy, cesarean section, and tubal ligation. Similarly, 32 (20.5%) patients in Group 2 had a history of abdominal surgery at a different anatomical site. Table 1 shows baseline characteristics in the study population. Comparing study groups, we noted no significant difference in preoperative variables.
UPJO, ureteropelvic junction obstruction.
The operation time was slightly longer in Group 1 patients, but this difference did not attain statistical significance (182.9±64.2 versus 168.1±45.7 minutes in Groups 1 and 2, respectively; P=.222). Furthermore, intraoperative blood loss was higher in Group 1 patients (473±359 mL versus 359±296 mL in Groups 1 and 2, respectively; P=.026). Although not statistically significant a trend toward a higher transfusion rate was noted in Group 1 patients: 6 (16.2%) patients in Group 1 and 12 (7.7%) in Group 2 required transfusion (P=.103). The postoperative serum creatinine level revealed no significant difference between the groups (1.17±0.36 versus 1.16±0.37 mg/dL for Group 1 and 2, respectively; P=.623). Hospital stay was also comparable between the study groups (3.7±1.2 versus 4.2±1.6 days in Groups 1 and 2, respectively; P=.1780).
The operation was converted to open nephrectomy in 1 (2.7%) and 3 (1.9%) patients of Groups 1 and 2, respectively (P=.765). Surgical and medical complications encountered did not differ significantly between the study groups (Table 2).
Furthermore, we assessed patients in Group 1 to see if the outcome of the LN differed between patients with previous percutaneous surgery (n=13) and those with a history of open renal surgery (n=24). Mean operative time, blood loss, hospital stay, and complication rate were similar irrespective of type of previous ipsilateral renal surgery.
Discussion
Intra-abdominal adhesions from a previous surgery have been reported to occur in 35%–90% of patients. 3 History of surgery at the same or a different site may adversely affect the subsequent LN. Several studies have investigated the impact of previous abdominal surgery at a site other than the ipsilateral renal unit on the outcome of LN. Some authors have reported serious complications relevant to the previous surgery,2,4–6 whereas others have shown that previous surgery at a different site does not affect the outcome of the subsequent urological laparoscopic surgery.7–9 However, published data assessing the impact of previous renal surgery on the outcome of LN are limited.
Abou-Elela et al. 4 reported 5 conversions to open surgery associated with major complications (i.e., injury to the liver and bleeding) in a series of 18 patients with a history of ipsilateral renal surgery; extensive adhesion between the renal pelvis and the posterior abdominal wall has been elucidated to be the main problem in LN in their study. Parsons et al. 2 in a retrospective cohort analyzed 399 patients who underwent LN and noted a higher transfusion rate in patients with a history of surgery at either the same or different anatomical site compared with patients who had no history of previous surgery; in addition, operation time and duration of admission was significantly longer in patients with a history at the same anatomical site compared with patients with a history of surgery at a different anatomical site and those with no previous surgery. Chen et al. 5 also reported 24 patients with a history of previous renal or abdominal surgery who underwent laparoscopic renal surgery; 5 patients with a history of surgery encountered major complications, including vena caval laceration and small bowel fistula.
In contrast to the studies that have shown an association between previous renal surgery and increased complication rate during subsequent LN, in a recent prospective study Aminsharifi et al. 7 evaluated 25 patients with a history of ipsilateral renal surgery and 50 patients without a history of surgery and noted comparable complication rate between the two groups; nevertheless, the operative time was longer among patients with a history of renal surgery. Furthermore, Turna et al. 10 reported 25 patients who underwent uneventful laparoscopic partial nephrectomy in spite of having a history of ipsilateral renal surgery. They reported the laparoscopic procedure to be more difficult technically among patients with a history of open partial nephrectomy because of circumferential mobilization of the renal vessels. However, it has not been associated with complication or conversion to open surgery.
Because our institution is a tertiary referral center and patients are referred specifically for laparoscopic surgery from all over the country, a relatively large number of patients underwent LN for a nonfunctioning kidney within this 5-year period. Twenty percent of patients who underwent LN in our study had had previous ipsilateral renal surgery. Therefore LN in patients with a history of ipsilateral renal surgery is not an uncommon procedure.
Baseline characteristics and preoperative variables were comparable between the two groups in our study. As was expected, the mean patient age was higher in Group 1 patients. However, this difference was not statistically significant. Because LN for renal tumors has been considered to be associated with a higher complication rate in comparison with benign conditions, 11 we excluded patients who underwent LN for renal tumor. A history of previous abdominal surgery at a different anatomical site is another confounding factor that may affect the outcome of the laparoscopic procedure. However, in our study a similar proportion of patients in Groups 1 and 2 had had previous abdominal surgery.
Applying the open access technique, we noted no access-related complications in either Group 1 or Group 2 patients. Conversion to open surgery was necessary in 1 patient in Group 1 and 3 in Group 2 (P=.765). Conversion to open surgery was performed because of nonprogression due to fibrosis and adhesions related to renal pathology (i.e., xanthogranulomatous pyelonephritis) or previous surgery. Intense fibrosis was evident in the posterior surface of the kidney with adhesion to the psoas muscle in the majority of patients. Dissection of the vascular pedicle was not associated with serious difficulty, and neither of the patients required conversion as a result of uncontrollable bleeding or other complications.
Surgical outcome was comparable between the two groups in our study, and we noted no significant difference in surgical and medical complications, operative time, and duration of hospitalization between study groups.
Injury to the spleen occurred in 2 patients in Group 1 and 2 patients in Group 2. The liver was also injured in 1 patient in Group 2. All these inadvertent injuries were small lacerations and were managed with either electrocauterization or a hemostatic agent.
Transfusion was required approximately two times more commonly in Group 1 than in Group 2 patients. Nonetheless, the difference was not statistically significant, which may be related to the limited power of the study. The transfusion rate in LN for a nonfunctioning kidney varies significantly in different studies. Aminsharifi et al. 7 reported a transfusion rate of 3.4% and 2% during LN in patients with and without a history of previous ipsilateral renal surgery, respectively. In another study by Parsons et al., 2 the transfusion rate was 1% among patients with no history of previous surgery, whereas 7.5% of patients with a history of previous surgery at the same site and 11.4% of patients with a history of surgery at a different site required transfusion. Hsiao and Pattaras 12 also reported a transfusion rate of 9.5% among patients with no history of prior surgery who underwent LN secondary to a benign pathology. Injury to the minor vessels (i.e., gonadal and lumbar vessels) was the leading cause of hemorrhage in our patients, and no injury to the major vessels was recorded. The amount of intraoperative blood loss (473±359 mL versus 359±296 mL in Groups 1 and 2, respectively) was not as high as expected to account for the high rate of transfusion in our study. Using a higher hemoglobin threshold for transfusion and relative anemia in our patients (mean preoperative hemoglobin in transfused patients was 12.2±1.2 g/dL) may explain the high transfusion rate in our study.
Type of previous renal surgery (i.e., percutaneous versus open surgery) does not seem to affect the outcome of subsequent LN.2,7 Percutaneous surgery is not associated with extensive defatting of the kidney and dissection of the renal vessels and is expected to result in less scarring. However, it should be considered that perinephric hematoma associated with percutaneous procedures may occasionally lead to serious adhesions and fibrosis. Subclassification of our patients by type of previous renal surgery (percutaneous versus open surgery) also did not reveal significant difference between the two subgroups.
The present study is retrospective in nature and associated with shortcomings pertinent to the retrospective studies. Our study may be associated with selection bias according to the nonrandomized design of the study, and the majority of patients with preoperative clinical and radiologic findings in favor of extensive adhesion may have been considered for open surgery. Furthermore, three different surgeons performed the LN procedures in our study, and this may affect the outcome of laparoscopic surgery. Nevertheless, it should be considered that the present study has been performed in a high-volume tertiary endourologic center, and therefore the difference in the level of experience among surgeons may be insignificant. Further studies of large-scale and high-quality design are also required to confirm our results.
Conclusions
LN in patients with a history of ipsilateral renal surgery is a feasible and safe procedure. Although higher intraoperative blood loss and transfusion rate were noted among patients with a history of ipsilateral renal surgery, the rate of other complications were comparable between the groups. Further studies with large sample size and high-quality design are also required to confirm our results.
Footnotes
Disclosure Statement
No competing financial interests exist.