
Abstract
Abstract
Objective:
The aim of this study is to report early and intermediate outcomes of laparoscopic surgery for choledochal cysts with 400 cases.
Patients and Methods:
The operation was performed using four ports. The cystic duct was identified and divided. The liver was suspended by two stay-sutures: one on the round ligament and the other on the distal cystic duct. The choledochal cyst was isolated and removed completely, and biliary–digestive continuity was reestablished by hepaticoduodenostomy (HD) or hepaticojejunostomy (HJ).
Results:
From January 2007 to June 2011, 400 patients were operated on. There were 305 girls and 95 boys. Ages ranged from 1 month to 16 years (mean, 47.5±2.1 months). Cystic excision and HD were performed in 238 patients and HJ in 162 patients. The mean operating time was 164.8±51 minutes for the HD group and 220±60 minutes for the HJ group. Conversion to open surgery was required in 2 patients. There were no perioperative deaths. Postoperative biliary leakage occurred in 8 patients (2%), resolving spontaneously in 7 and requiring a second operation in 1 patient. The mean postoperative hospital stay was 6.4±0.3 days for the HD group and 6.7±0.5 days for the HJ group. Follow-up between 5 months and 57 months postdischarge (mean, 24.2±2.7 months) was obtained in 342 patients (85.5%). Cholangitis occurred in 5 patients (1.5%) in the HD group and 1 patient (0.6%) in the HJ group. Gastritis due to bilious reflux was 3.8% in the HD group.
Conclusions:
Laparoscopic repair is a safe and effective procedure for choledochal cyst. The rate of cholangitis and anastomotic stenosis is low.
Introduction
Since 2007, laparoscopic surgery has been routinely used in our hospital for choledochal cyst. 11 The aim of this study is to present early and intermediate outcomes of laparoscopic surgery for choledochal cyst with 400 cases.
Patients and Methods
Criteria for inclusion
All children from 1 month to 16 years old with choledochal cyst of Type I or IVa according to the Todani classification who underwent laparoscopic repair for choledochal cyst from January 2007 to June 2011 at the National Hospital of Pediatrics, Hanoi, Vietnam, were included.
Criteria for exclusion
Patients with biliary atresia Type I were excluded. Laparoscopic operation was not indicated for patients with perforated cyst or previous biliary surgery.
Procedures
From January 2007 to November 2007, cystectomy plus hepaticoduodenostomy (HD) was carried out. From December 2007 to June 2010, both techniques of HD and hepaticojejunostomy (HJ) were performed. Cystectomies were performed by one of four senior laparoscopic surgeons. All biliary–digestive anastomoses were performed by the same (most experienced) surgeon. The main variables studied were patient age, cyst diameter, surgical technique, conversion rate, operative time, perioperative complications, and follow-up results.
Surgical techniques
Cystectomy plus HD
The patient was placed in a 30° head-up supine position, with the surgeon standing at the lower end of the table between the patient's legs (Fig. 1). A 10-mm trocar was inserted through the umbilicus for the scope. Three additional 5-mm trocars (or 3-mm for infants) were placed for instruments: one at the right flank, one at the left flank, and the fourth 2 cm below the left costal margin.

Patient position.
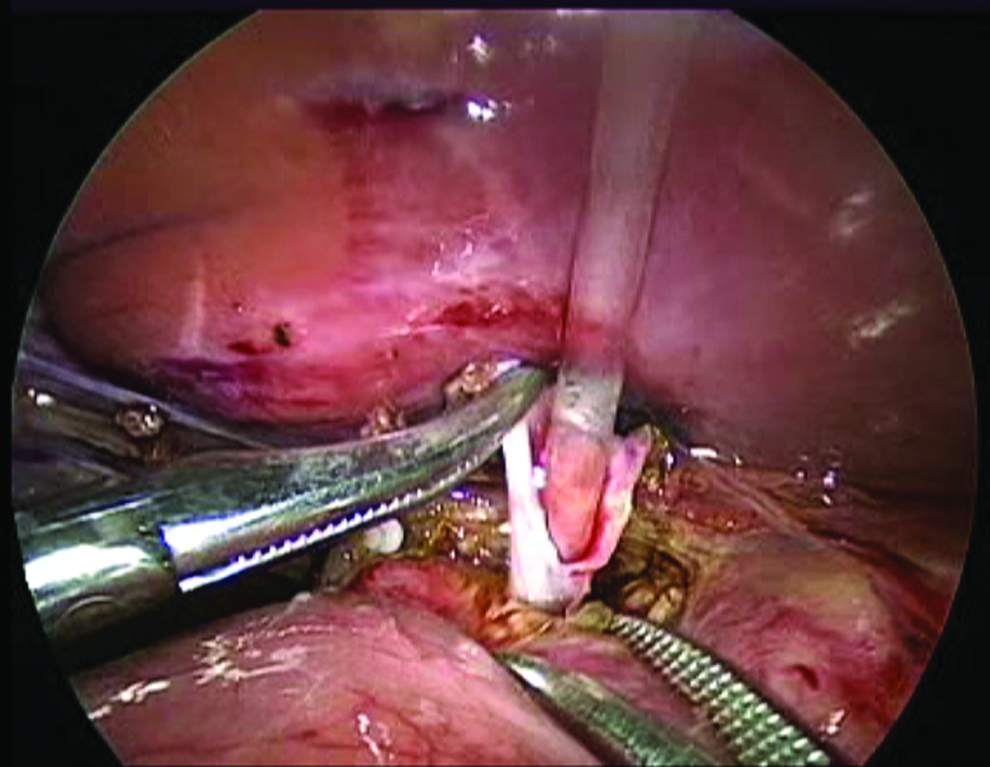
A carbon dioxide pneumoperitoneum was maintained at a pressure of 8–12 mm Hg. The liver was suspended from the abdominal wall by a suture placed at the round ligament. The cystic artery was isolated, clipped, and divided. The cystic duct was also isolated, clipped, and divided. A second traction suture was placed at the distal cystic duct and gallbladder to elevate the liver and to expose the liver hilum (Fig. 2). The midportion of the cyst was dissected circumferentially. Separation of the left and posterior wall of the cyst from the hepatic artery and portal vein was meticulously and progressively carried out until a dissecting forceps could be passed through the space between the posterior wall of the cyst and the portal vein, going from the left to the right side (Fig. 3).

Second traction suture.

A dissecting forceps passes through the space between the posterior wall of the cyst and portal vein.
The duodenum was retracted downward using an intestinal grasper inserted through the left flank trocar. The lower part of the cyst was detached from surrounding tissue and pancreatic tissue using a 3-mm dissecting forceps for dissection and cautery. The distal cyst was removed progressively and then opened longitudinally to identify the opening of the choledochus to the common biliopancreatic channel. A small catheter was inserted into the common channel to irrigate with normal saline to eliminate debris and biliary stones (Fig. 4). The distal choledochus was then clipped and divided (Fig. 5). The upper part of the cyst was further dissected up to the common hepatic duct and divided under the cystic duct. The orifices of the common hepatic duct and the right and left hepatic ducts were inspected internally and identified. The upper part of the cyst was then divided from the common hepatic duct 5–10 mm under the hepatic bifurcation. The hepatic ducts were also irrigated via the small catheter to eliminate debris and biliary stones. The duodenum was mobilized, and an HD was constructed 2 cm from the pylorus using running sutures (if the diameter of the common hepatic duct was larger than 1 cm) or with polydioxanone 5/0 interrupted suture (if the diameter was smaller than 1 cm).
A small catheter is inserted into the common channel.

The distal choledochus is clipped and divided.
A cholecystectomy was then carried out. Different parts of the cyst were removed through the 10-mm trocar. A subhepatic drain was inserted.
Cystectomy plus HJ
The patient and trocars were positioned the same way as for complete cyst excision plus HD. The ligament of Treitz was identified by laparoscopy. A 5/0 silk stay-suture was placed 30.0 cm distal to the ligament of Treitz. A second 5/0 polydioxanone suture was placed 2.0 cm below the first suture to mark the jejunal limb, which would later be anastomosed to the hepatic duct. The jejunal segment with two sutures was grasped with an intestinal grasper. The trocar at the umbilicus was withdrawn. The transumbilical vertical incision was extended 1.0 cm above the umbilicus. The jejunum was exteriorized, and the jejunojejunostomy was carried out extracorporeally. The jejunum was then reintroduced into the abdominal cavity. The extended incision was closed. The laparoscopic instruments were repositioned, and the choledochal cyst was dissected and removed. The Roux limb was brought retrocolic to the porta hepatis. An HJ was fashioned.
Results
From January 2007 to June 2010, laparoscopic cystectomy and biliodigestive anastomosis were performed for 400 children with choledochal cysts, including 305 girls and 95 boys. The patient mean age was 47.5±2.1 months (range, 1 month–192 months). Clinical manifestations on admission are presented in Table 1.
The mean diameter of choledochal cysts on ultrasound was 47.8 mm (range, 10–170 mm). One hundred sixty-three patients had preoperative associated intrahepatic dilatation of biliary ducts, and 237 had no associated intrahepatic dilatation. Cystic diameter was not different between patients in the HD and HJ groups (47.5±15.4 mm versus 48.3±16 mm, respectively).
Cystectomy plus HD was performed in 238 patients and cystectomy plus HJ in 162 patients.
Three different techniques of cystectomy were carried out:
• Dissection and division of the cyst in the middle before removing the distal and proximal parts in 249 patients (62.2%) • Opening the front wall of the cyst and separating the cyst from the portal vein while viewing inside and outside the cyst in 105 patients (26.3%) • Dissection and division of the cyst from the distal end before dissecting the middle and upper parts in 46 patients (11.5%)
Perforation of the right hepatic duct occurred in 1 patient and was laparoscopically closed with 6/0 Vicryl® suture (Ethicon). Transection of two hepatic ducts was done in 3 patients, and ductoplasty was carried out before performing HD in 2 patients. Laparoscopic HJ at two different sites was performed in the third patient, in whom the distance between the two hepatic ducts was too great to bring them together. A twist of the Roux limb was detected and repaired laparoscopically during operation in 2 patients.
Conversion to open surgery was required in 2 patients because of a common hepatic duct tear while performing HD in one patient and because of long operative time in the other patient with a large and highly adhesive cyst.
Mean operative time was 164.8±51 minutes in the HD group and 212±61 minutes in the HJ group. The difference is significant (P<.01).
Intraoperative transfusion was required in 4 patients.
Postoperative biliary leakage occurred in 8 patients (2.0%): 4 patients in the HD group (1.7%) and 4 patients in the HJ group (2.5%). The difference is not significant (P=.31). One patient in the HD group required a second operation. The leakage resolved with medical treatment in the remaining 7 patients. Subhepatic fluid collection was seen in 2 patients (0.5%), which resolved after fluid aspiration under ultrasound guidance.
All biliary leakage and fluid collection occurred before 2009. Pancreatic fistula occurred in 4 patients (1.0%) but resolved with medical treatment. There were no operative or postoperative deaths.
Postoperative stay was 6.4±0.3 days in the HD group and 6.7±0.5 days in the HJ group. The difference is not significant (P=.11).
Follow-up of 5–57 months (mean, 24.2±2.7 months) was obtained for 342 children (85.5%), including 207 patients in the HD group and 135 patients in the HJ group. Cholangitis occurred in 5 patients in the HD group. Of these 5 patients, 3 patients required a second operation (2 patients due to anastomotic stricture and 1 patient due to stenosis of the hepatic bifurcation and intrahepatic stones). One patient with anastomotic stenosis was successfully treated by transcutaneous balloon dilatation. All anastomotic stenoses happened in patients who underwent their first operation before January 2008.
One patient in the HJ group had cholangitis. The rate of cholangitis is not significantly different between the two groups (P=.24). Duodenal bleeding due to ulcer occurred in 1 patient in the HJ group but resolved with medical treatment. Gastritis owing to bilious reflux occurred in 8 patients in the HD group (3.8%).
Discussion
Results from these 400 laparoscopic operations reveal that laparoscopic surgery is feasible for choledochal cyst. Only 2 cases (0.05%) required conversion to open surgery. The laparoscopic operation is indicated for most choledochal cysts of Todani Type I and Type IVa except patients with previous biliary surgery or perforated cyst. Our results also demonstrate that laparoscopic surgery is a safe approach for choledocal cysts. The intraoperative complication rate is favorable in comparison with open surgery. 18 All intraoperative complications could be managed laparoscopically.
Twisting of the Roux limb happened in the HJ group. This complication has also been reported in other series. 19 Careful inspection of the Roux limb before performing the anastomosis could prevent it. A shorter intestinal loop is also recommended to avoid this complication. 19
Transection of two hepatic ducts occurred in 3 patients in our series and has also been reported in other series.6,7 Ductoplasty in a double-barrel fashion could be carried out if the distance between the two ducts is not too great. HJ in two different sites is an alternative when two hepatic ducts cannot be brought together. Internal inspection of the upper remnant of the cyst to identify the orifice of the common hepatic duct and right and left hepatic ducts is necessary to avoid this complication.
The rate of biliary leakage in our series was 2.0% and decreased with operator experience. This complication has not been seen in our center since 2009.
Postoperative bleeding requiring reoperation did not occur in any patient, possibly because of improved hemostasis under laparoscopic magnification.
The rate of postoperative complications in our series is lower in comparison with open surgery.18,20
Follow-up varied from 5 to 57 months, demonstrating that intermediate outcomes of laparoscopic operations for choledochal cyst are satisfactory. The rate of anastomotic stenosis in our series was 0.87%. This rate has varied from 9% to 24% in different reports of results with open surgery.21–23 All patients with anastomotic stenosis underwent operation between January 2007 and July 2008. This fact suggests that the rate of anastomotic stenosis may depend on the surgeon's skill.
Ascending cholangitis is a great concern in HD. However, this rate was low in our series and not significant different in comparison with that in HJ. Gastritis due to bilious reflux was only seen in the HD group.
We presently perform HD at 3 cm instead of 2 cm from the pylorus. Whether the rate of reflux would be lower because of this modification is a question for further research.
Upper gastrointestinal bleeding due to duodenal ulcer occurred in 1 patient in the HJ group. This complication was also reported by Martino et al. 24
From our results we can conclude that laparoscopic surgery is a safe approach for choledochal cyst. The postoperative rates of cholangitis and anastomotic stenosis are low.
Footnotes
Acknowledgments
The authors thank Dr. John Taylor, Clinical Associate Professor, Department of Pediatrics, School of Medicine, University of Washington, for his careful reading and valuable comments on the manuscript.
Disclosure Statement
No competing financial interests exist.