
Abstract
Abstract
Introduction:
Minimally invasive surgery in children with long-segment intestinal aganglionosis aims to reduce the number of abdominal wall incisions. Conventional laparoscopic and laparoendoscopic single-site (LESS) surgeries fulfill this goal. In children, natural orifice translumenal endoscopic surgery (NOTES™; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society for American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) has been limited because of fear of access site complications. We present a novel technique of totally transanal LESS pull-through colectomy (TLPC), avoiding abdominal wall incision, which combines LESS technology and the NOTES approach.
Subjects and Methods:
Two boys and one girl (2.5 months, 6 months, and 5 years of age, respectively) with sigmoid and transverse colon aganglionosis underwent surgery. The TLPC procedure consisted of an endorectal technique with submucosal dissection starting 1 cm orally from the dentate line to above the peritoneal reflection, where the rectal muscle was divided circumferentially. After ligation of the rectal mucosa, the proximal bowel was replaced into the abdominal cavity, and a TriPort® (Olympus Surgical Technologies Europe, Hamburg, Germany) was introduced transanally. Mesenterial resection of the aganglionic bowel was accomplished via transanal LESS until the normoganglionic colon segment was reached and pulled down to the site of anastomosis. After removal of the port, a conventional pull-through procedure was performed.
Results:
All children displayed normal bowel movements and were complication-free during the follow-up period of up to 7 months.
Conclusions:
TLPC combines the minimally invasive LESS surgery with the scarless concept of NOTES and allows resection of long-segment aganglionosis without abdominal incision. TLPC is a safe, effective, and feasible surgical procedure in children with long-segment intestinal aganglionosis.
Introduction
Natural orifice translumenal endoscopic surgery (NOTES™; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society for American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) and laparoendoscopic single-site (LESS) surgery are currently revolutionizing minimally invasive surgery. Natural orifice specimen extraction combined with conventional left-sided laparoscopic colectomy is used in the adult population in order to avoid a larger abdominal wall incision for specimen extraction and the creation of an anastomosis. 3 However, the intra-abdominal laparoscopic dissection is performed with instruments introduced through multiple incisions in the abdominal wall. In contrast, our technique prevents any incision of the abdominal wall.
Our idea was to combine the transanal access to the abdominal cavity as described by de la Torre-Mondragon and Ortega-Salgado 2 with the LESS TriPort® (Olympus Surgical Technologies Europe, Hamburg, Germany) as used in laparoscopic single-access transumbilical appendectomy. We present, for the first time in pediatric surgery, the successful management of long-segment colonic aganglionosis using a novel technique of totally transanal LESS pull-through colectomy (TLPC).
Subjects and Methods
Two boys and one girl (2.5 months, 6 months, and 5 years of age, respectively) with intestinal aganglionosis underwent surgery after the diagnoses of HD was confirmed by histological analysis, anorectal manometry, X-ray contrast enema, and failure of conservative treatment with laxatives and enemas. The transition zone was located in the sigmoid colon in 2 cases and in the transverse colon in 1 case. The 5-year-old patient with the transition zone located in the transverse colon had previously undergone a colostomy. Written, informed consent was obtained from the parents of the children, and the study design was approved by the appropriate ethics review boards.
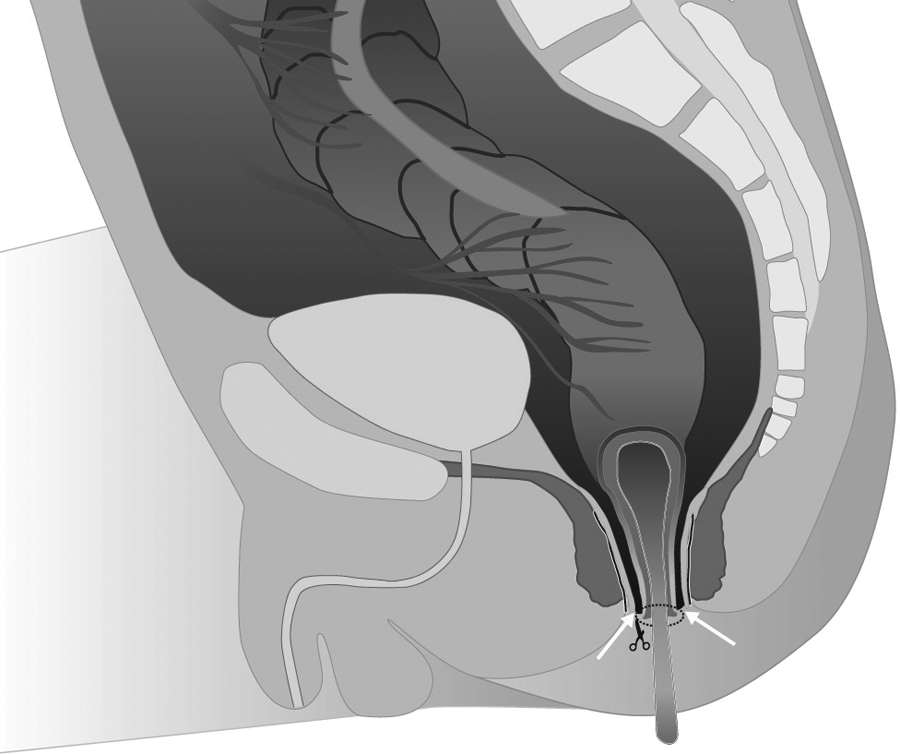
Rectal irrigations were performed prior to surgery. The perisurgical antibiotic regimen consisted of daily intravenous administration of cefuroxime (100 mg/kg of body weight in three doses) and metronidazole (20 mg/kg of body weight in two doses) for 5 days starting at the onset of anesthesia. The endorectal pull-through procedure, initially described by de la Torre-Mondragon and Ortega-Salgado 2 and adopted by several pediatric surgeons, 1 was modified for this surgery. The patient was positioned on the operating table in the dorsal lithotomy “suspension” position, and a Foley catheter was inserted into the bladder. The rectal mucosa was grasped with four traction sutures placed above the dentate line. After the mucosa was everted, traction sutures were attached to a ring. The endorectal circumferential mucosa dissection (Fig. 1) started 1 cm above the dentate line (2–3 cm below the peritoneal reflection). The rectal mucosa was incised, and the submucosal plane was exposed using blunt dissection. The edge of the mucosal cuff was closed distally with multiple sutures, which were used for traction. The endorectal submucosal dissection was then continued proximally, to a point above the peritoneal reflection (Fig. 2) at about 4–7 cm above the dentate line (depending on the child's size). At this point, the rectal muscle was divided circumferentially (Fig. 3). The traction sutures were tied together, and the endorectal tube was allowed to fall back into the abdomen. Subsequently, the rectal muscular cuff was split longitudinally posteriorly (Fig. 4). Depending on the child's size the muscular cuff had a length of approximately 4–7 cm. The TriPort system was inserted transanally (Fig. 5). The blue elastic ring of the TriPort was unfolded intraperitoneally to provide a pneumoperitoneum without CO2 leakage (Fig. 6). Under direct transanal laparoscopic observation, mesenterial resection of the aganglionic rectal, sigmoid, and colonic bowel was accomplished until the estimated normoganglionic colon segment was reached. Figure 7 shows the intraoperative situs. Dissection was continued very close to the bowel wall to avoid damage to the splanchnic innervation by using LigaSure™ (Covidien, Mansfield, MA). During the division of the vessels, bowel perfusion was ascertained under direct laparoscopic observation. When the transition zone was encountered, full-thickness biopsy sections were taken to confirm the presence of ganglion cells. Full-thickness biopsy sections were extracted via the opened TriPort ring. The biopsy sites were left open because they were situated below the resection line, and the mucosa was not opened.

An incision was made (scissors symbol) in the mucosa, situated 0.5–1 cm above the dentate line.

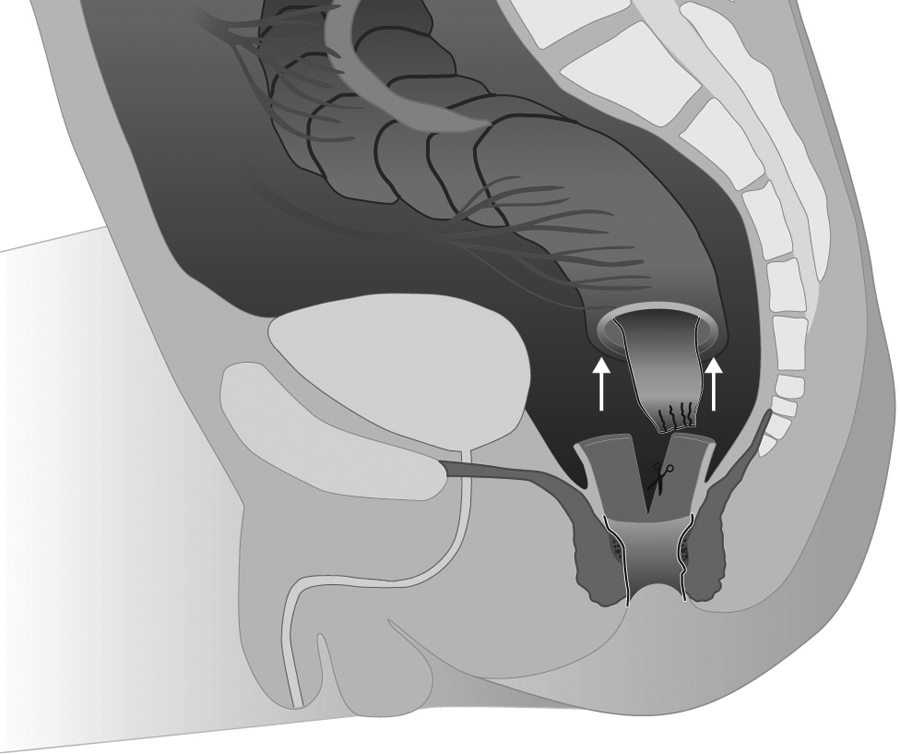
After a circumferential mucosal incision was performed (scissors symbol), the endorectal mucosa tube was detached from the muscular layer by means of submucosal dissection and closed with multiple traction sutures. The endorectal submucosal dissection was carried out proximally, to a point above the peritoneal reflection, about 4–7 cm above the dentate line (depending on the child's size). Traction on the mucosal tube developed the folds of the rectal muscular sleeve (arrows).
Transection in the muscle of the denuded rectum (arrows and scissors symbol) began to form the muscular sleeve.
After the endorectal tube was allowed to fall back into the abdomen, the muscular sleeve was split longitudinally posteriorly.
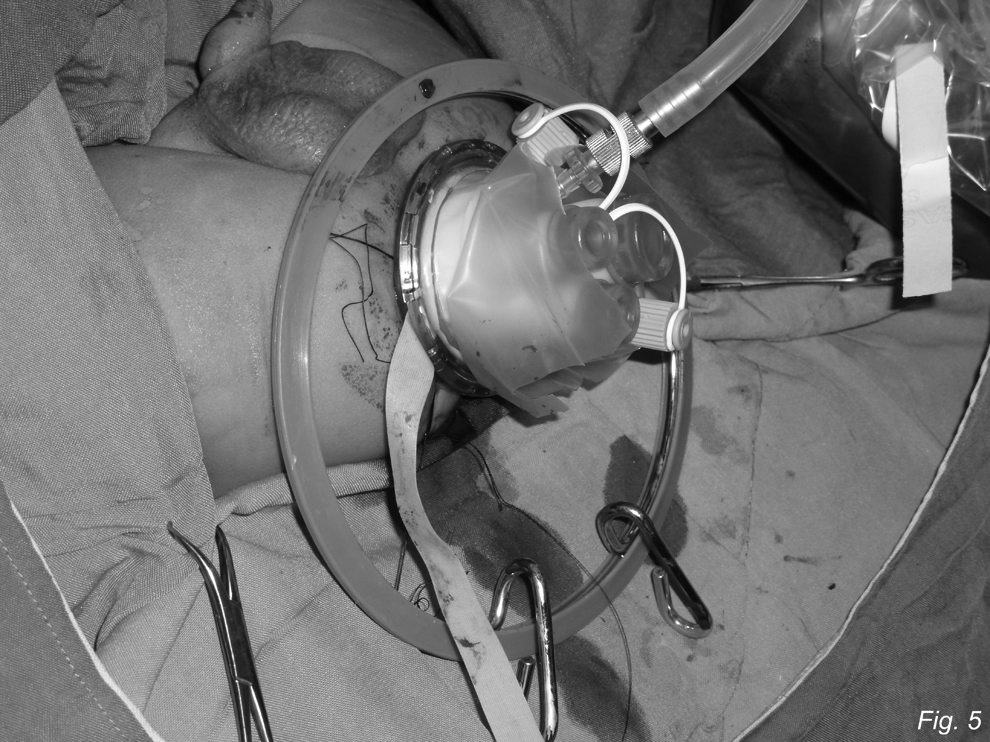
Intraoperative picture of the transanal TriPort for laparoendoscopic single-site surgery.
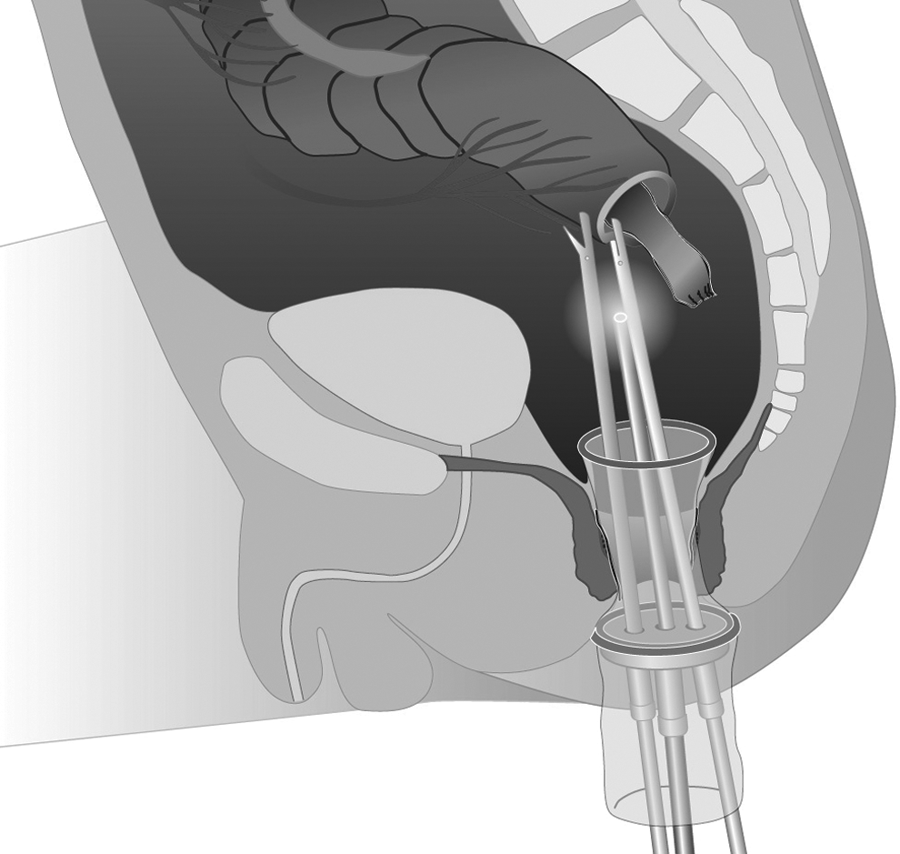
A TriPort was inserted through the muscular sleeve, and a pneumoperitoneum was induced. The dissection was continued above the dilated transition zone, dividing the mesenteric vessels as they enter the colonic wall using LigaSure.
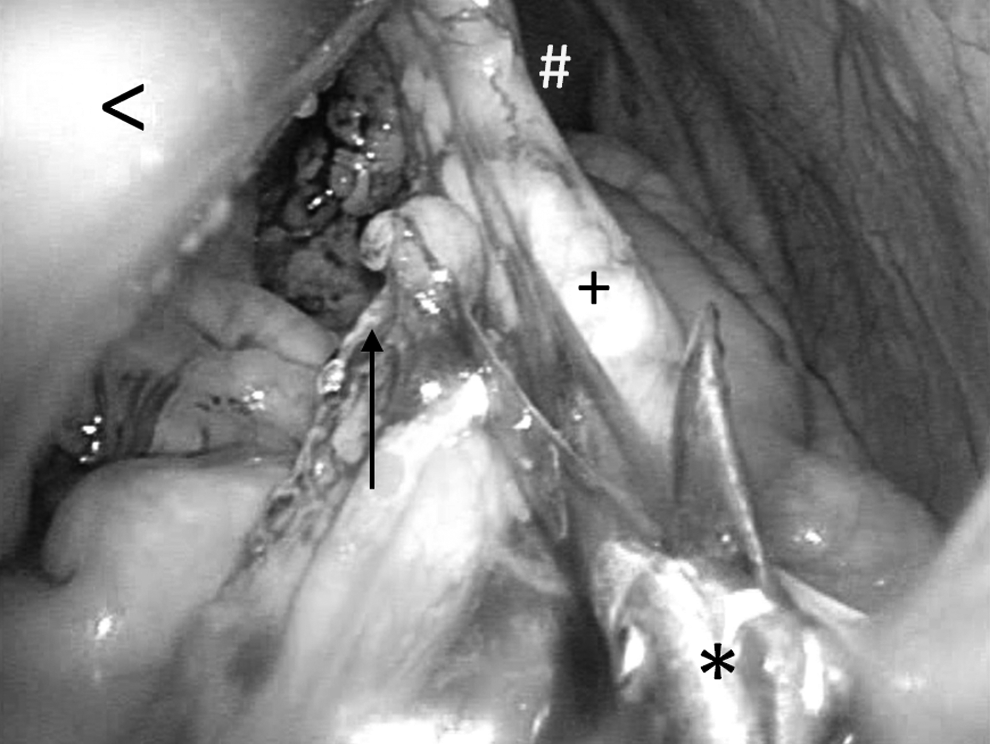
Transanal endoscopic view showing transsection of the vascular pedicle of the colon: grasper (<), electric scissors (*), colonic mesentery (arrow), aganglionic colon (+), and spleen (#).
Vascular perfusion of the normoganglionic bowel was repeatedly monitored during traction and dissection. Finally, simulation of the pull-through was performed several times down to the site of the planned anastomosis to ascertain adequate vascular perfusion, under laparoscopic observation. At this point, the TriPort was removed, taking care to withdraw the traction sutures of the endorectal tube outside the anus. The endorectal tube was carefully retracted outside the anus to prevent torsion, and the colon was divided several centimeters above the most proximal normal biopsy site (Fig. 8). The anastomosis to the rectal mucosa was sutured with absorbable material (Fig. 9), as previously described. 2
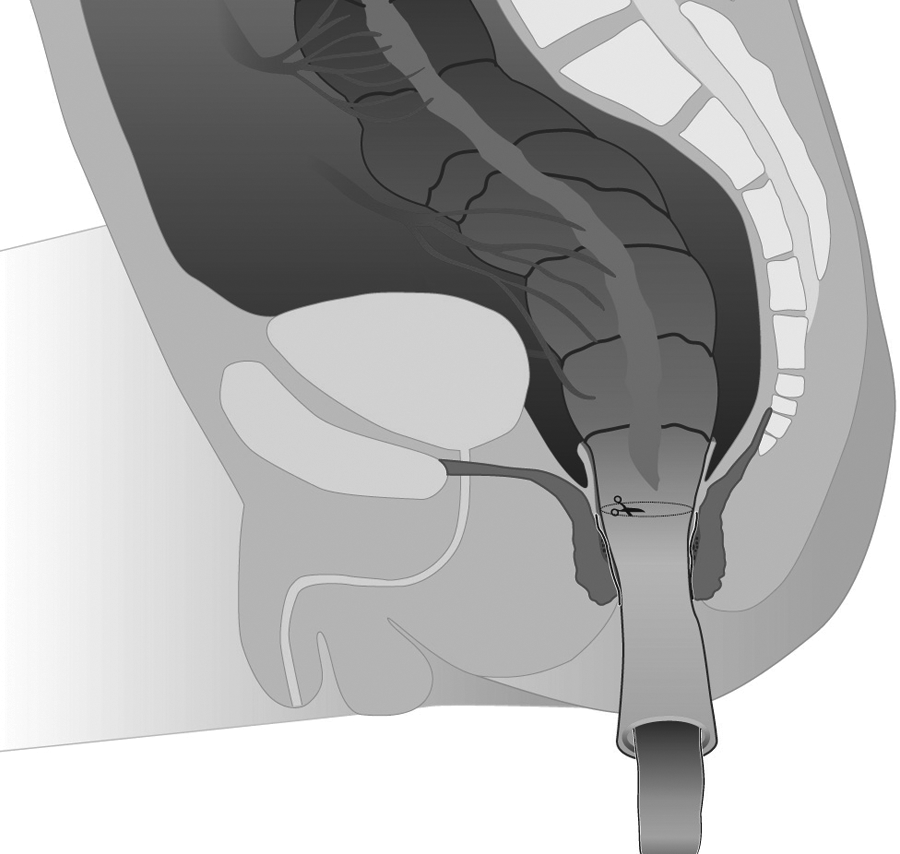
The mobilized aganglionic bowel segment was pulled through the split muscular sleeve (scissors symbol indicates the planned resection site above the transition zone).

After resection of the bowel, the anastomosis was completed outside the anus and allowed to retract into the abdomen.
In the patient having a previous transversostomy and a transitional zone located aborally in the left transverse colon, we had to mobilize the descending colon, the splenic flexure, and the transverse colon. While the colon was mobilized, the simultaneously taken biopsy specimens showed an aganglionary segment located very close to the stoma. We decided to free the transverse colon up to the mesenterium of the oral stoma segment by LESS. This was performed using traction on the bowel with one instrument and using either LigaSure or electric scissors in order to take down the mesenteric attachments (Fig. 7). Subsequently, the stoma opening was excised out of the abdominal wall by open surgery and temporarily closed. The abdominal wall incision was then closed in order to restore the capnoperitoneum. Under laparoscopic visualization the previously mobilized oral transversostoma segment was then pulled down through the anus and anastomosed to the rectum.
The patients were started on oral food after 24 hours and discharged around postoperative Day 5. By this day patients had resumed oral intake and had regular bowel movements. We observed the patients by routine until postoperative Day 5 in order to gain experience with the postoperative treatment and exclude early complications with the new method.
Digital rectal examinations were performed 2 weeks after the operation. Rectal dilatations were continued daily by the parents for 6–8 weeks.
Results
The duration of the surgical procedure was 2 hours 20 minutes and 2 hours 35 minutes for the 2 patients with sigmoid HD. For the patient with HD located in the transverse colon with existing transversostoma, the duration of operation was 3 hours 46 minutes.
Follow-up information was available at 7 months after the operation for the patient with the transition zone located in the transverse colon and at 5 months for the other 2 patients. During the follow-up period of up to 7 months, no complications occurred. All children displayed normal bowel movements.
Discussion
Minimizing incisional trauma during surgery for HD has become a goal in pediatric surgery. A decisive step was the description, 4 in 1995, of the primary laparoscopic-assisted pull-through technique, using transabdominal ports through multiple incisions. Abdominal incisional trauma was abolished, in selected cases, following the description of transanal endorectal pull-through (TEPT) in 1998 by de la Torre-Mondragon and Ortega-Salgado. 2 They performed rectal mucosectomy, aganglionic segment colectomy, and normoganglionic colon pull-through through the anus. However, the original TEPT had limitations precluding the treatment of long-segment bowel aganglionosis.
In a recent review of the method, de la Torre and Langer 5 underlined that, for children with a transition zone that is more proximal than the midsigmoid colon, there is usually not enough length to bring the ganglionic bowel down without mobilization of at least the descending colon and, in some cases, the splenic flexure. For these cases, TEPT had to be combined with a laparoscopic procedure through an umbilical incision.
In our cases the preoperative radiological findings did not permit a clear analysis of the distance of the aganglionic segment. LESS gave us the opportunity to better visualize the position of the transition zone. In addition, TLPC offered us the possibility to continue the transanal pull-through without need for abdominal wall incision even in cases where the aganglionic segment is located more proximal than the midsigmoid.
A step toward reducing the invasiveness of this gold standard was shown in 2008 by Diana et al., 6 who performed a transumbilical single-port colectomy in an experimental model and reported survival. Nevertheless, the original concept of eliminating abdominal incisions remained unfulfilled for long-segment aganglionosis.
Transanal trocar insertion for correction of sigmoid HD was described in a single case. 7 In this procedure, three trocars were inserted transanally, with the patient in the prone position. The authors proved that the method was feasible in a single case with a transitional zone in the lower sigmoid, while encountering the escape of CO2. This is consistent with the term “pure NOTES,” as emphasized in a technical review of the method. 8 However, proximal mobilization is usually not required for children with a transition zone in the rectum or the sigmoid colon. Here, a conventional TEPT usually solves the problem, and laparoscopic visualization is not mandatory. The situation is different when long-segment aganglionosis is encountered. For a transition zone at or just proximal to the splenic flexure, the flexure must be taken down, and the middle colic vessels must be divided, ensuring that the marginal vessels are preserved. In these situations, there is need for safe, intra-abdominal visualization of the entire colon. In our experience, this is best achieved without CO2 escape. The next logical step involved combining TEPT with transanal single-port surgery, thus completely eliminating incisions in the abdominal wall. A single transanal TriPort prevented CO2 escape and allowed excellent visualization of the entire colon, permitting the extension of TEPT to long-segment aganglionic bowel disease.
Resection of the long aganglionic bowel segment in HD represents an ideal indication for TLPC because the port entry site is resected and the anastomosis is completed between the rectum and ganglionic bowel. The surgical procedure is initially technically demanding but can be safely accomplished with an acceptable learning curve. In the beginning, the surgeon is confronted with new challenges and limitations compared with the conventional laparoscopic approach. As previously reviewed, 6 the difficulties consist of the need for all instruments to come through a single entry point with almost parallel orientation, resulting in the clashing and crossing of instruments. Handling of the tissue is initially more difficult, and the cranial and posterior aspects of the bowel are more difficult to visualize because the camera position cannot be changed. However, we could visualize the area around the splenic flexure very well (Fig. 7). Another current limitation is the length of the 3-mm instruments. This is no problem when surgery is focused on the colonic frame in small patients like the ones we operated on and as encountered in the majority of cases with HD. Here, the handling and visualization of the distantly located colonic flexures are excellent. However, in older patients this might be a limiting factor.
In situ, the shape of the TriPort resembles an hourglass. At its narrowest point the diameter of 1.3 cm is calculated by the sum of the diameter of the instruments. These are one 5-mm optics, one 5-mm LigaSure device, and a 3-mm grasper. We believe that this causes less overstretching than the manipulations performed in the conventional open transanal surgery.
With increasing experience in LESS procedures, the surgeon is able to overcome these difficulties and take advantage of TLPC. TLPC includes transanal natural orifice specimen extraction, 9 thus solving the problem of resection and retrieval of long bowel specimens, a feature otherwise considered a limitation of colorectal LESS procedures. Additionally, TLPC might be an alternative to laparoscopic-assisted colorectal surgery in adults.
In conclusion, TLPC is a safe and elegant method to treat long-segment bowel aganglionosis without abdominal incisional trauma. This technique has a possible application for total colonic HD with colectomy and ileoanal pull-through and also for colonic resection for ulcerative colitis.
Footnotes
Acknowledgments
We thank Mrs. Charlotte Schmitz (CATSNFROGS Medical Illustrations) for illustrating the steps of the surgical procedure.
Disclosure Statement
No competing financial interests exist.