
Abstract
Abstract
Purpose:
Laparoscopic management of inflammatory bowel disease (IBD) has been well established in adults. Its efficacy and safety are less defined in pediatrics. We reviewed our single surgeon laparoscopic experience with pediatric IBD patients.
Patients and Methods:
All consecutive patients 17 years old or younger with IBD who underwent initial laparoscopic surgery for management of disease from May 2002 to May 2011 were identified. Patients were analyzed retrospectively with respect to age, gender, weight, American Society of Anesthesiologists classification, history of prior abdominal surgery, operative time, need for conversion to open procedure, estimated blood loss, need for blood transfusion, length of hospitalization, need for intensive care unit monitoring, and patient outcomes within 30 days.
Results:
In total, 44 pediatric patients underwent 52 laparoscopic surgeries. Forty-two patient cases (80.8%) had had no prior abdominal surgery. Mean operative time was 132 minutes. Two patients (3.8%) underwent conversion from a laparoscopic to open approach. Mean estimated blood loss was 64 mL. The average hospitalization was 5.5 days. Postoperative complications occurred in 10 patients (19.2%): 2 were treated for wound infection or abscess, 7 required re-admission, and 1 required return to the operating room for exploratory laparotomy.
Conclusions:
Laparoscopic management of IBD has not routinely been implemented in the pediatric population. We demonstrate acceptable perioperative morbidity and rate of conversion to open with an overall successful laparoscopic approach in pediatric patients. This may have particular long-term benefits in a population faced with longer life expectancy. An initial laparoscopic approach is a feasible and safe option for pediatric IBD patients.
Introduction
In the pediatric population, the experience with laparoscopic surgery has been limited. Although laparoscopic surgery has been evaluated and long been in use for general pediatric surgery diseases, 4 the use, efficacy, and safety of a laparoscopic approach have been less clearly defined in the pediatric IBD population. To our knowledge, few studies have evaluated the indications for a laparoscopic approach and surgical complications in the management of pediatric inflammatory disease. We therefore reviewed the laparoscopic surgical indications, procedures, and complications in the treatment of pediatric IBD at our single institution by a single surgeon.
Patients and Methods
Patient selection
This retrospective descriptive study was approved by our institution review board with waiver of informed consent and is HIPAA compliant. Between May 2002 and May 2011, patients were prospectively entered into a database. In total, 44 consecutive pediatric patients with 52 surgeries underwent a laparoscopic approach for IBD by a single fellowship-trained colorectal surgeon with 16 years of experience after fellowship training. The surgeon has handled over 2000 laparoscopic colorectal cases. The pediatric population was defined as being younger than 18 years old at a single institution. Ulcerative colitis, Crohn's disease, and indeterminate colitis were considered.
Data review
From the electronic medical record and charts, patients were analyzed retrospectively with respect to age, gender, weight, American Society of Anesthesiologists classification, and prior abdominal surgery. Procedures performed included small bowel procedures, ileocolic resection, colorectal resection, and ileal pouch-anal anastomosis.
Perioperative factors included were operative time, rate of conversion, estimated blood loss and need for blood transfusion, length of stay, need for intensive unit care monitoring and duration, complication rate, and final pathology findings. Complication rates within the first 30 days postoperatively included wound or intra-abdominal infection requiring antibiotics or drainage, re-admission, or return to the operating room.
Results
Over the 9-year study period, in total, 44 pediatric patients underwent 52 laparoscopic surgeries. The mean age at time of surgery was 14.1 years (range, 3.5–17 years). Eighteen patients were male, and 26 were female. The average weight at time of surgery was 84.3 pounds (range, 22–156 pounds). The average American Society of Anesthesiologists classification was 2.25. Forty-two patients (80.8%) had no prior abdominal surgery. Ten patients (19.2%) had had previous bowel surgery, including proctosigmoidectomy with ileal pouch-anal anastomosis and loop ileostomy (n=6), ileocolic resection (n=1), diagnostic laparoscopy, lysis of adhesions, and takedown of ileostomy (n=1), left hemicolectomy (n=1), and total abdominal colectomy (n=1). Demographic data are given in Table 1.
Data are mean (range) values unless indicated otherwise.
ASA, American Society of Anesthesiologists; F, female; ICU, intensive care unit; LOS, length of stay; M, male.
Of the 44 patients, 37 patients underwent a single surgery, 6 patients underwent two operations, and 1 patient had three surgeries. Sixteen patients (36.4%) underwent 21 surgeries (40.4%) for ulcerative colitis. Crohn's disease was the operative indication for 25 patients (56.8%) undergoing 28 surgeries (53.8%). Lastly, 3 patients (6.8%) each underwent surgery (5.8%) for indeterminate colitis. Of the 52 operations, 3 were small bowel procedures, 17 were ileocolic resections, and 32 were colorectal resections, of which 14 included ileal pouch-anal anastomosis. The distribution of cases categorized by diagnosis is shown in Figure 1.
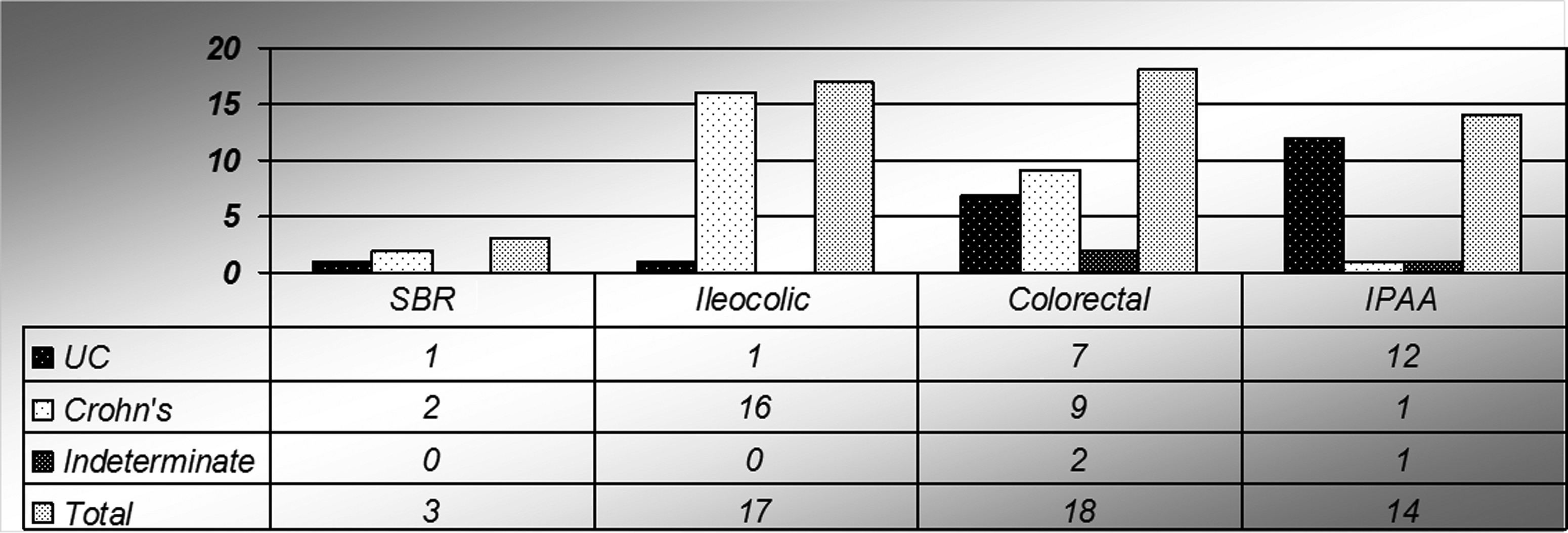
Types of surgery performed. IPAA, ileal pouch-anal anastomosis; SBR, small bowel resection; UC, ulcerative colitis.
Mean operative time was 132 minutes (range, 23–317 minutes). Estimated blood loss was 64 mL (range, 5–350 mL). Six patients received blood transfusions ranging from 150 mL to 2 units (average, approximately 600 mL) of packed red blood cells. Average hospital length of stay was 5.5 days, of which no patients required monitoring in a higher level of care setting (Table 1).
Complications within the first 30 days postoperatively included wound or intra-abdominal infection requiring antibiotics or drainage, re-admission, or return to the operating room. Postoperative complications were noted in 10 of 52 patients (19.2%), among whom 2 (3.8%) were treated for wound infection or abscess, 1 (1.9%) required return to the operating room on postoperative Day 3 for small bowel obstruction and peritonitis with a negative exploration, and 7 (13.5%) required re-admission for ileus or dehydration (Table 2). Four patients (7.6%) had superficial wound complication (n=3) or an intra-abdominal collection requiring drainage (n=1).
Forty-two cases underwent successful laparoscopic definitive treatment of IBD. Two surgeries (3.8%) were converted from a laparoscopic to an open approach. One patient with ulcerative colitis required conversion to an open procedure because of the severity of colonic inflammation present. Another patient with Crohn's disease required conversion because of severity of mesenteric inflammation present near the terminal ileum (Table 3).
Final pathologic examination revealed findings consistent with the original diagnosis in all 47 patient cases, 4 with nonspecific findings of inflammation versus reactive changes, and 1 patient diagnosed with Crohn's disease had pathology consistent with ulcerative colitis.
Discussion
The laparoscopic management of IBD is a safe and technically feasible option in the adult population. In the pediatric population, some small studies have evaluated the safety of laparoscopic surgery. Initial reports described the use of laparoscopic surgery to aid in the diagnosis of Crohn's disease. 5 Several studies have since been conducted to evaluate the safety and utility of a laparoscopic approach for pediatric patients.
Many of these studies are limited by sample size. In a study of 11 patients undergoing subtotal colectomy for IBD, the laparoscopic approach was not inferior to the open approach. 6 A subsequent case series of 15 patients undergoing laparoscopic ileocecectomy for Crohn's disease also showed the safety of this approach. 7 Additional reports have demonstrated the safety of laparoscopic surgery for pediatric patients, including those with IBD. 8
Laparoscopic surgery may offer additional advantages. In a study of 12 patients undergoing laparoscopic surgery for segmental bowel resection compared with 16 patients undergoing open surgery, the laparoscopic approach was associated with improved pain control and early return of bowel function. 9 Additionally, laparoscopic surgery may offer improved cosmesis, decreased ileus, and subsequent shorter hospitalization. 10
Overall rates of postoperative morbidities were similar to those with open surgery.11–13 In a study of pediatric patients including 29 with IBD, 5% of patients had a postoperative complication. One patient presented with an infected hematoma and 1 with an abscess. Additionally, 1 patient was found to have an injury of the ureter, another an injury of the urethra, and the last patient exhibited small bowel obstruction with abscess and pouch ischemia. Overall, 5% of patients required conversion to open surgery. 14
Most patients had never had prior abdominal surgery, yet those with prior surgery were still able to have successful repeat laparoscopic surgery. Overall, our rate of complications was higher than that reported in the literature. This may be due to a larger number of patients undergoing urgent surgery for refractory colitis as well as an increased rate of more distal anastomoses. Our conversion rate to open surgery was slightly lower at 3.8%, despite including patients with prior abdominal surgery.
The outcomes of laparoscopy in the pediatric population are comparable to those in the adult population. In a meta-analysis published by Wu et al., 15 overall complication rates in ulcerative colitis patients were seen in 39.3% of patients. This is higher than our rate in pediatric patients of 23.8%. Conversion to the open procedure was found to be 4.2%, 15 which is slightly lower than the 4.8% in this study. Similarly, in a prospective study at the University of Chicago, 55 patients underwent laparoscopic colectomy for Crohn's colitis; the complication rate was 14.5%, 16 which is consistent with our 14.3% complication rate. Duepree et al. 17 studied laparoscopic Crohn's disease patients and reported a complication rate of 14% and a conversion rate of 4.8%, which is higher than in our pediatric population. These studies demonstrate that performing laparoscopy in the pediatric population is not faced with overall greater morbidity or conversion in IBD patients as if performed in adults.
Several factors limit our study. Inclusion of more patients would allow for improved analysis. Additionally, there were no patients who underwent primary open surgery to allow for a direct comparison of laparoscopic versus open surgery outcomes. However, this is one of the largest consecutively obtained studies of laparoscopic surgery (of all types) in pediatric IBD patients.
Overall, this study demonstrated a successful laparoscopic approach in the pediatric population. A laparoscopic approach may have particular long-term benefits as pediatric patients are faced with a longer life expectancy and thus a higher likelihood of repeat surgery in the future. The pediatric population with inflammatory bowel disorders requiring surgery can be routinely and safely offered an initial laparoscopic approach in the hands of a laparoscopic-experienced surgeon.
Footnotes
Disclosure Statement
No competing financial interests exist.