
Abstract
Abstract
Objective:
This randomized clinical study compared the feasibility and safety of the shortest suture for bidirectional knotless barbed versus standard sutures, with either extracorporeal or intracorporeal knots, for vaginal cuff closure following total laparoscopic hysterectomy (TLH) and lymph node dissection for early endometrial cancer.
Subjects and Methods:
The study design was Canadian Task Force Classification I. In tertiary-care university-based teaching hospitals, 61 women underwent TLH and lymph node dissection. In accord with randomization, the vaginal cuff in TLH was closed with either extracorporeal or intracorporeal knots (1-Monocryl®; Ethicon Inc., Somerville, NJ) and a bidirectional knotless barbed suture (0-Quill™; Angiotech Pharmaceuticals, Inc., Vancouver, BC, Canada). All patients were evaluated at 3-month, 6-month, and 1-year follow-up.
Results:
Time required to suture was significantly lower in the group treated with bidirectional suture than in groups with traditional sutures (P<.001). No significant difference was observed in the operative time between the study groups. The degree of surgical difficulty was significantly lower in the bidirectional barbed suture group than in the other groups. At 1-year follow-up all patients presented no wound dehiscence, no bleeding, dyspareunia, and other potential major complications such as ureteric, bladder, or bowel injury.
Conclusions:
Use of a barbed suture reduces the time required to repair the vaginal cuff during TLH. At follow-up of patients, carried out 3 months, 6 months, and 1 year after the surgery, no wound dehiscence, no bleeding, or no other potential major surgical complications had occurred.
Introduction
Barbed sutures have recently been proposed to facilitate laparoscopic suturing and have been used in various surgical fields.3–5 The barbed suture is a relatively new concept in gynecologic surgery. The Quill™ SRS bidirectional barbed suture (Angiotech Pharmaceuticals, Inc., Vancouver, BC, Canada) was Food and Drug Administration–approved for soft tissue approximation in 2004 and has been commercially available in the United States since 2007. Recently the unidirectional V-Loc™ absorbable wound closure device product line (Covidien, Mansfield, MA) has been introduced.
Bidirectional barbed sutures are created by cutting barbs into the suture, with the barbs facing in the opposite direction to the needle. Up to now, barbed sutures have received a favorable impression in gynecologic surgery.6–11
The present study is a clinical, prospective, controlled, randomized trial designed to compare the feasibility, safety of the shortest suture, and the percentage of postoperative surgical dehiscence with bidirectional knotless barbed versus standard suture, with either extracorporeal or intracorporeal knots, for vaginal cuff closure following hysterectomy. Additionally, we evaluated patients at 3-month, 6-month, and 1-year follow-up.
Subjects and Methods
The present clinical, prospective, controlled, randomized trial compared the effectiveness of the bidirectional knotless barbed suture versus standard suture, with either extracorporeal or intracorporeal knots, in the repair of the vaginal cuff and peritoneum during TLH and pelvic and para-aortic lymph node dissection, for early stage endometrial cancer. This study was conducted at the Department of Obstetric, Gynaecology and Reproductive Medicine of the Second University of Naples, Naples, Italy, and at the Operative Unit of Obstetrics and Gynaecology, A.O.R.N. S.G. Moscati, Avellino, Italy.
In total, 61 patients with clinical stage I endometrial cancer (disease limited to the uterine corpus), who underwent TLH in the period of July 2010–October 2011, were enrolled in this study. All patients enrolled in the study had their initial pathologic diagnosis confirmed at our institutions. The staging of the patients was done according to the FIGO 2010 staging system. 12 All the women enrolled in the study gave their written informed consent at study inclusion. The study protocol received institutional review board approval before the beginning of the study, in accordance with The Code of Ethics of the Declaration of Helsinki. Exclusion criteria for the study were previous uterine surgery, additional diseases requiring surgical treatment (such as endometriosis, tubal surgery, or appendicitis), body mass index of ≥29 kg/m2, contraindications for general anesthesia, and psychiatric disorders precluding informed consent. No patient included in the study underwent medical treatment for ovarian suppression before surgery.
Demographic data of the patients included in the study were collected on the day before surgery. For the purpose of the study, the hemoglobin (Hb) concentration was determined on the day before surgery and at 24 hours after surgery; the difference in Hb concentration (ΔHb) was calculated to estimate the intraoperative blood loss.
Two surgeons (L.C. and M.A.) performed the surgical procedures. The following parameters were analyzed: the time needed to perform the intervention and the suture, respectively, and the blood and Hb loss. Additionally, at the end of each surgical procedure, the surgeons evaluated the degree of surgical difficulty of suturing the vaginal cuff by use of a visual analog scale scale ranging from 1 (low difficulty) to 10 (high difficulty) as previously described by Vassiliou et al. 13
All surgical procedures were recorded. The operative time was determined by reviewing the surgical procedures by use of Final Cut Pro (Apple, Inc., Cupertino, CA); it was calculated between the beginning of the operation (after the insertion of the trocars) and the removal of the trocars. The same technique was used to determine the time required to vaginal cuff closure.
Patients were randomized into three groups for suture of the vaginal cuff through use of a computer-generated list drawn up by a statistician: Group A (n=16), extracorporeal knots; Group B (n=14), intracorporeal knots; and Group C (n=12), bidirectional knotless barbed suture 14-×14-cm 0 caliber (Quill sutures). In Groups A and C poliglecaprone 25 (1-Monocryl; Ethicon Inc., Somerville, NJ) was used.
Surgical procedure
TLH was performed with standard technique as previously described by Malzoni et al. 14
Suture of the vaginal cuff was performed in accordance with the randomization. In particular, for Group C, one of the two needles of the bidirectional suture was inserted in the right corner of the vagina, and the suture of the cuff was performed from right to left with five or six stitches in a running fashion, excluding the parietal peritoneum. Then, by using the second needle and with the same direction, a second layer was generated, incorporating the peritoneum posteriorly (Fig. 1).
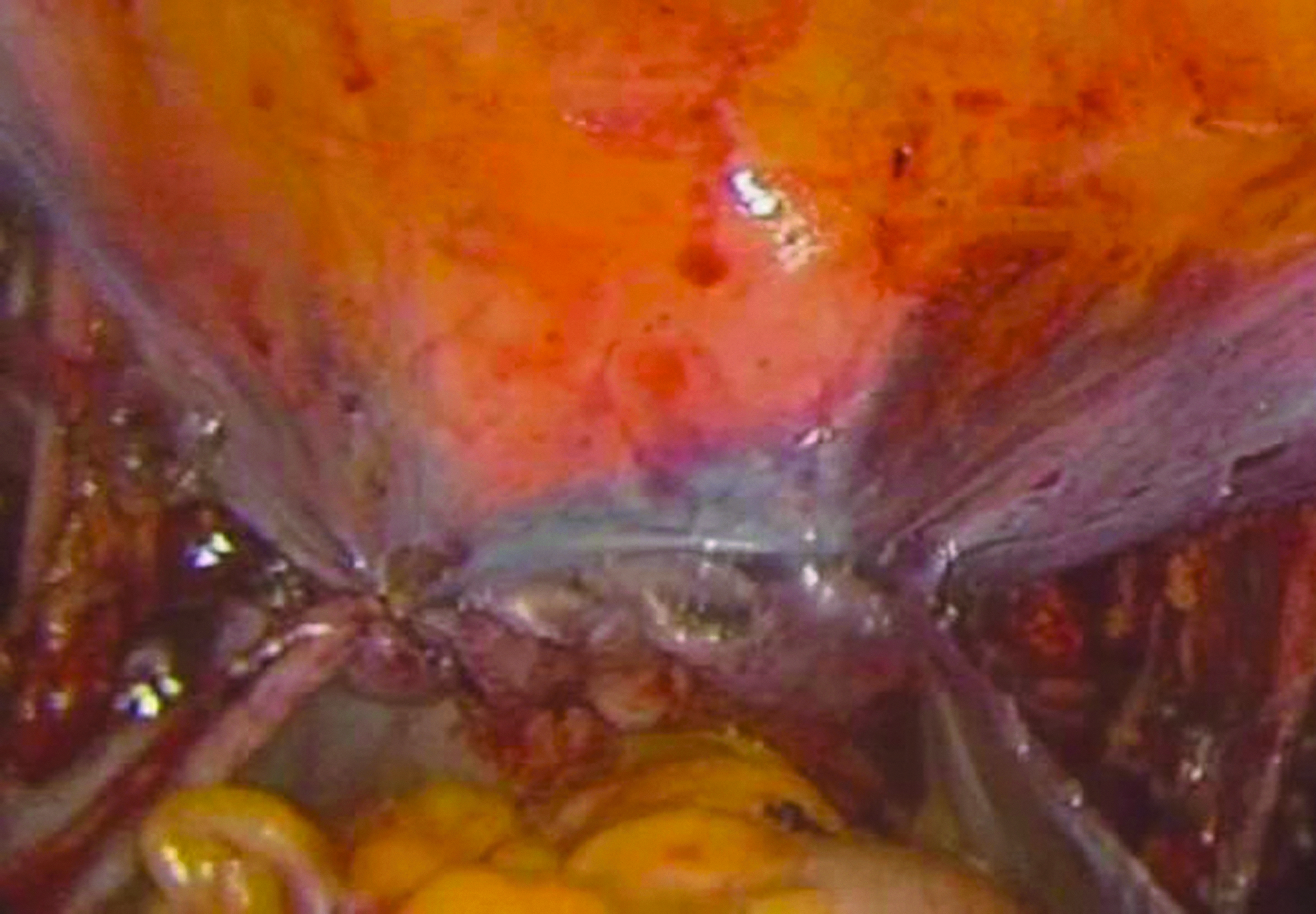
Vaginal cuff coated with peritoneum sutured with Quill after total laparoscopic hysterectomy.
Statistical analysis
For this study, in which the primary aim was to estimate whether a bidirectional knotless barbed suture is significantly faster than a standard suture performed with either extra- or intracorporeal knots in suturing the vaginal cuff after TLH, a pre-test power analysis based on our retrospective data (last 100 TLHs performed by L.C. and M.A.) showed a mean (±standard deviation) time required to perform the suture of the vaginal cuff of 7.3±3.6 minutes.
Considering as clinically significant a difference of 60% in operative time between experimental and control surgical procedures, a two-sided test power calculation was performed. The standard deviation of the time required for suturing during the last 100 TLHs performed by the two surgeons (3.6 minutes) was used as the sigma value. Thus, we needed a sample size of 12 in each group to yield a statistically significant result with a power ≥80% to detect a difference in means of 60% at a 5% level of significance.
Data were analyzed by use of Student's t test and the chi-squared test for parametric variables, whereas the Mann–Whitney U test was used for nonparametric variables. Differences in operative time, suture time, and degree of surgical difficulty in suture performing were assessed by one-way analysis of variance, followed by Bonferroni's post hoc comparisons to investigate pairwise differences between individual groups. Statistical calculations were performed using Statistical Package for the Social Sciences (SPSS) software (version 17.0; SPSS Inc., Chicago, IL). A value of P<.05 was considered statistically significant.
Results
Demographic characteristics of the patients are given in Table 1. The study groups appeared to be globally homogeneous. Moreover, no significant difference was observed among groups in tumor stage. All procedures were completed by laparoscopy, and no conversion to laparotomy was required.
Data are mean±standard deviation values or percentage (n) as indicated.
P<.05 was considered statistically significant.
BMI, body mass index.
No significant difference was observed in the operative time (median±standard deviation [95% confidence interval]) between patients in Group A (133.4±12.9 minutes [122.0–153.1]), Group B (141.5±15.7 minutes [127.5–157.0]), and Group C (131.5±14.8 minutes [121.8–154.9]) (Table 2). However, the time required to suture the vaginal cuff was significantly lower in Group C (3.9±2.0 minutes [3.2–6.7]) than in Groups A (6.2±2.9 minutes [3.7–9.9]) and B (7.1±4.5 minutes [4.3–11.4]) (P<.01). The intraoperative blood loss (ΔHb) was similar in the three groups (Group A, 0.6 g/dL; Group B, 0.3 g/dL; Group C, 0.2 g/dL). Blood transfusion was not required in any case. The degree of surgical difficulty, evaluated by a visual analog scale, was significantly lower in Group C (4±2 [2–7]) than in Groups A and B (6±2 [4–9] and 7±1 [5–9], respectively]) (P<.01) (Table 2).
Data are median±standard deviation values [95% confidence interval].
P<.05 was considered statistically significant.
NS, not significant; VAS, visual analog scale.
At 3-month, 6-month, and 1-year follow-up of patients, no wound dehiscence, no bleeding, no visits to the hospital due to bleeding, no dyspareunia, and no other potential major complications such as ureteric, bladder, or bowel injury occurred.
Discussion
During the last 20 years, laparoscopic techniques have changed the gynecologic surgeon's approach to the suture. Indeed, the need of obtaining a suture that was easier, sure, and functional during laparoscopic surgery contributed to give a substantial impulse to this field.9,15–17 Therefore, despite the multitude of different procedures performed, no study or surgeon has yet identified the perfect suture for all situations.
In recent years, a new class of sutures—barbed suture—has been introduced by the industry. Barbed sutures eschew the traditional, smooth, knot-requiring characteristic of sutures in favor of barbs that anchor the suture to the tissues without a knot. To perform a laparoscopic suture with knot tying is probably the most challenging surgical procedure for a gynecologic laparoscopist in the course of TLH.
In 2008 Greenberg and Einarsson 7 reported the first use of barbed sutures in gynecologic surgery. Since this preliminary report, many publications followed with an increasing number of patients enrolled.6–11 Moreover, recently bidirectional barbed sutures have been introduced into clinical practice and tested for performing abdominoplasty in humans, 3 for closing gastrointestinal enterotomies in pigs, 4 and for closing the collecting system and renal parenchyma during laparoscopic partial nephrectomy in pigs. 5
In 2010 Einarsson et al. 6 performed a retrospective analysis, calling patients 6 months after surgery to inquire about number of days of postoperative vaginal bleeding, visits to the hospital due to bleeding, dyspareunia, and other potential complications. Thus the use of bidirectional barbed sutures appeared to be safe for closing the vaginal cuff in a TLH. 6
Therefore, although previous authors described the use of a bidirectional barbed suture in the closure of the vaginal cuff after TLH,6,7 up to now no study has prospectively compared barbed sutures and standard sutures with either intracorporeal or extracorporeal knots in gynecologic surgery and evaluated 3-month, 6-month, and 1-year follow-ups. This prospective, controlled, randomized study demonstrates, for the first time, that the use of a barbed suture reduces the time required to repair the vaginal cuff during TLH. 3
Moreover, our results showed that the bidirectional suture is rapid and simple to use. Obviously, the decrease in suturing time is due to the fact that there is no need of tying knots. Additionally, we showed that bidirectional barbed sutures did not cause dehiscence of the vaginal cuff, bleeding, dyspareunia, and other major complications at 3-month, 6-month, and 1-year follow-up. This result is very important because the bidirectional barbed suture, due to its configuration, could exert a major impact ton the tissue.15–18 Instead, our data show that this suture is free of possible collateral effects, and we suggest that the absence of dehiscence is probably due to the more rapid reabsorption of the wire because of its configuration.
Conclusions
This study demonstrates that bidirectional barbed suture can be safely and effectively used for laparoscopic suturing, and in particular in the closure of the vaginal cuff after TLH, which is the last step of a surgically challenging procedure. Based on our experience, we believe that the further development and incorporation of this suture material into clinical practice should be actively explored.
Footnotes
Disclosure Statement
No competing financial interests exist.