
Abstract
Abstract
Objective:
To present a preliminary experience with the modified technique of extravesical intraureteral injection of non–animal-stabilized hyaluronic acid/dextranomer (NASHA/Dx) gel under direct ureteroscopic visualization for the treatment of primary high-grade vesicoureteral reflux (VUR).
Patients and Methods:
The medical records of all pediatric patients (age range, 0–14 years) who underwent intraureteral injection of NASHA/Dx gel under direct ureteroscopic visualization for the treatment of primary high-grade VUR during the period June 2006–June 2010 were reviewed.
Results:
Eighty-nine children (61 boys, 28 girls; M:F ratio, 2.1) underwent intraureteral injection of NASHA/Dx gel under direct ureteroscopic visualization for the treatment of primary high-grade VUR during the study period. VUR completely disappeared after the injection of NASHA/Dx gel into 105 (73%) of 144 ureters, with no further treatment required. Thirty-five (24.3%) required a second injection, and 2 (1.4%) required a third injection for resolution of their VUR. No intraoperative complications were observed. No ureteral obstruction during follow-up was observed using ultrasound or micturition studies.
Conclusions:
Intraureteral injection of NASHA/Dx gel under direct ureteroscopic visualization is safe and effective in the treatment of primary high-grade VUR, including cases with ureteral duplication, if the ureteral meatus is easy to pass through without mechanical dilation. This approach represents an effective and safe alternative to antibiotic prophylaxis alone and open surgery.
Introduction
Non–animal-stabilized hyaluronic acid/dextranomer (NASHA/Dx) gel has been used successfully in Europe for over a decade for the endoscopic treatment of VUR. No long-term complications have been associated with its use.4,5 It is a biocompatible injectable agent that has been shown in animal models not to migrate from the injection site thanks to the size of the dextranomer microspheres.6,7
The procedure itself is well tolerated with a low risk of associated complications.4,8 The low morbidity associated with the endoscopic injection of these types of bulking agents has encouraged many centers to recommend this approach as the initial treatment for primary high-grade VUR instead of antibiotic prophylaxis or re-implantation of the ureter.9–11 While biocompatible NASHA/Dx gel has become a popular subureteral and intraureteral injectable agent for the endoscopic treatment of VUR,5,12–15 its use for high-grade reflux has not been standardized yet.
The purpose of this study is to present our preliminary experience with a modified technique of intraureteral extravesical injection of NASHA/Dx gel under direct ureteroscopic visualization for the treatment of primary high-grade VUR in children.
Patients and Methods
The medical records of all pediatric patients (age range, 0–14 years) who underwent intraureteral injection of NASHA/Dx gel under direct ureteroscopic visualization in order to treat primary high-grade VUR (grade 4–5) during the period June 2006–June 2010 at Gaslini Children's Hospital and Research Institute (Genoa, Italy) were reviewed. Symptomatic VUR was diagnosed by voiding cystourethrogram (VCUG) or ultrasound and classified according to the international classification for VUR. 10
Either a 99m-technetium-dimercaptosuccinic acid or a magnetic uroresonance was performed to evaluate the presence of renal parenchymal scarring 4–6 months after a urinary tract infection. Patients with secondary VUR, including posterior urethral valve and neurogenic bladder, were excluded from the study because they first needed treatment for the primary cause of VUR.
Follow-up consisted of periodic urinalysis, renal bladder ultrasound 1 month after treatment, and VCUG and ultrasound 4–6 months after the procedure and then 1 year after the procedure. Further endoscopic treatment was considered if VUR persisted. Antibiotic prophylaxis was continued until the radiological follow-up and was suspended if VUR was disappeared.
Surgical technique
The patient is placed in the lithotomy position, and cystoureteroscopy is performed with a nonflexible pediatric ureteroscope 8–15 French (according to the patient's age), 15° lens, with the patient under general anesthesia. Hydrodistention of the distal ureter is created through a pressured stream by placing the tip of the ureteroscope at the ureteral orifice. Hydrodistention is graded according to the classification system developed by Kirsch et al. 15 If hydrodistention allows insertion of the ureteroscope without mechanical dilation, the injection of NASHA/Dx gel under direct ureteroscopic visualization of the intraureteral injection site is performed.
A ureteral catheter is introduced before the injections through the meatus into the ureteral lumen in order to identify the level of the detrusor muscle. A flexible needle (Oceana Therapeutics Ltd., Edison, NJ) is used in order to perform the injection. About 0.1–0.2 mL of NASHA/Dx gel is used for each submucosal injection. In total, six submucosal injections are performed at different levels and sites (Fig. 1): two intraureteral, extravesical injections proximal to ureteral insertion into the vesical wall and detrusor muscle; two intraureteral, intravesical injections at the level of the detrusor muscle; and the last two intravesical, subureteral, 2–3 mm below the refluxing orifice as described by Puri et al.4,11
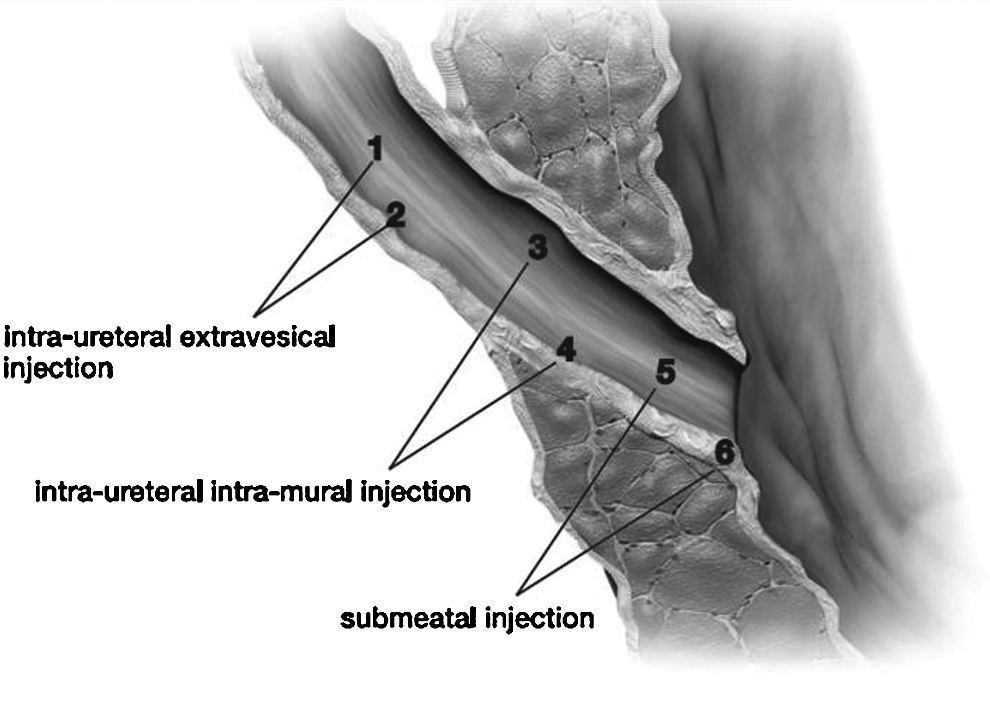
Two submucosal extravesical injections are performed proximal to ureteral insertion into the vesical wall and detrusor muscle. Two more intravesical injections are performed at the level of the detrusor muscle, always submucosally, and another two inside the meatus and subureterally as described by O'Donnell and Puri. 22
Results
Eighty-nine children (61 boys, 28 girls; M:F ratio, 2.1) underwent intraureteral injection of NASHA/Dx gel under direct ureteroscopic visualization for the treatment of primary high-grade VUR during the study period. Patients' ages ranged from 4 months to 15 years (median age, 3 years). The median operative time was 15 minutes (range, 5–25 minutes).
VUR was unilateral and bilateral in 34 (38.2%) and 55 (61.8%) patients, respectively, resulting in 144 high-grade refluxing ureters. Ureteral duplication was present in 23 of 89 patients (25.8%). In 27 of 55 patients with bilateral VUR (49.1%), a lower grade of VUR (grade 1–3) in one of two sides was observed. In 42 of 89 patients (47.2%), a scarred kidney was identified through 99m-technetium-dimercaptosuccinic acid scans.
VUR completely disappeared after the first injection of NASHA/Dx gel in 105 of the 144 ureters (72.9%), thus requiring no further treatment, whereas a second injection was required in 35 (24.3%) and a third injection in 2 (1.4%) (Table 1).
Percentages are based on the number of total ureters treated.
VUR, vesicoureteral reflux.
Two patients underwent re-implantation of the ureter after a single injection because of parental preference. One patient presented with a new contralateral VUR during follow-up after correction of unilateral VUR by a single endoscopic injection of NASHA/Dx. No intraoperative complications were reported. No ureteral obstruction during follow-up was observed using ultrasound or through the evaluation of urinary flow rate. No major hematuria, postoperative infections, or urinary retention were seen. After VUR resolution, urinary tract infections were no longer described in any patient.
Discussion
The current practice of low-dose, continuous antibiotic prophylaxis for the treatment of VUR in children can result in antibiotic resistance of common causative pathogens responsible for urinary tract infections. 16 Poor treatment compliance may also contribute to antibiotic resistance, as exposure to subtherapeutic levels of antibiotics encourages the development of resistant strains. 17 Given the clinical and social ramifications of poor compliance with antibiotic treatments, there is a need for strategies to improve rates of compliance and/or for alternative therapies to deal with this problem.
Open surgery is costly, requires hospitalization, and results in postoperative pain as well as anxiety of both the child and the caregiver. The two therapies for VUR (surgical ureteral re-implantation and endoscopic dextranomer–hyaluronic acid copolymer injection) provide options that do not involve long-term antibiotic prophylaxis. Compared with open surgery, endoscopic injection is minimally invasive, can be performed as an outpatient procedure, is cost-effective, and provides VUR resolution rates are at least equivalent to surgery. 18 These two options result in cure rates of 98% versus a spontaneous resolution rate of up to 50% over a year for patients receiving prophylactic antibiotics. 19
When given information on each of the two treatment options, 80% of parents of patients with moderately severe VUR chose endoscopic injection. 20 According to some studies,10,12,21 the opinion of parents is important in the choice of the approach, and their clear preference for endoscopic treatment indicates a clear understanding of the minimally invasive nature of the procedure.
The rationale of our modified technique of injection can be found in the basic principles of treatment for primary high-grade VUR.12–15,21,22 Submeatal injection provides a solid support under the ureteral orifice, thus increasing the submucosal length of the ureter, with resultant improvement of the anti-reflux valve mechanism.12,22 Intraureteral intravesical injections at the level of the detrusor muscle allow a reduction of the distal ureter lumen with a resultant lower risk of bolus dislodgement.12,23
The aim of our modified technique of submucosal intraureteral extravesical injections proximal to ureteral insertion into the vesical wall and detrusor muscle on different levels, under direct visualization, is to obtain a lumen reduction and remodeling of the ureteral wall as seen in the Kalicinski ureteral folding technique for megaureter. 24 Injection on different axes allows the stacking-up of two boluses, thus reducing the risk of gel displacement or stricture. Direct ureteroscopic visualisation is mandatory to carefully identify intraureteral injection sites and to avoid ureteral obstruction.
Some reported studies do not recommend postoperative VCUG if there are no clinical signs or symptoms.9,10,12 However, we perform routine VCUG or ultrasound 4–6 months after all procedures to confirm the surgical results.
This modified technique showed a high VUR resolution rate (73%) after one injection of NASHA/Dx gel with a smaller complication rate compared with open surgery. The procedure can be easily repeated in case of persistence of reflux. 10 Moreover, open surgery following injection treatment did not represent a more difficult procedure in our experience.
In conclusion, thanks to the optimal results obtained over a 4-year period, we have standardized our modified technique even for high-grade primary VUR, including ureteral duplication. Intraureteral injection of NASHA/Dx gel under direct ureteroscopic visualization is safe and effective if the meatus is easy to pass through without mechanical dilation, thus representing an effective and safe alternative to antibiotic prophylaxis alone and open surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.