
Abstract
Abstract
Background:
Laparoscopy requires a set of skills such as intracorporeal stitching and knotting. The aim of this study is to present an effective specialized training course for the laparoscopic suturing technique.
Materials and Methods:
We designed a specialized 5-day training course for laparoscopic suturing skills with theoretical and practical sessions on inanimate pelvic training. The “gladiator rule” was the method used to teach intracorporeal suturing using the right and left hand from a lateral and suprapubic access. Data on sense of depth, coordination, dexterity, traction power, and posture at the beginning and at the end of the course were compiled. Three practical evaluations were performed by each course participant. Follow-up on subsequent live laparoscopic application of intracorporeal suturing was obtained.
Results:
We enrolled 44 consecutive trainees: 33 men and 11 women. We found a significant statistical improvement during the course in coordination (P=.001), dexterity (P=.000), traction power (P=.002), and posture (P=.003). Men were better than women in coordination (P=.002), dexterity (P=.000), and traction power (P=.014). No significant statistical difference in suturing skill was found in relation to age, gender, previous courses, surgical training (surgeon or resident), and dominant hand. Twenty-nine of 40 (72.5%) trainees after the course began to apply intracorporeal sutures in vivo.
Conclusions:
The present study demonstrates the utility of a 5-day suturing course in teaching laparoscopic suturing technique. The “gladiator rule” is a useful and reproducible theory to teach intracorporeal knotting. The three-step model allows the majority of the trainees to apply laparoscopic suturing in vivo.
Introduction
The traditional Halstedian apprenticeship model—that means “See one, do one, teach one” 4 —has been challenged, as the opportunity for learning in the operating room has diminished, mainly because of pressures of time, cost, and medicolegal concerns.5,6 The best way to overcome this learning curve seems to be attending a formal training in a skilled laboratory. 7 Laparoscopic suturing is an advanced skill that enables the surgeon to broaden the application of laparoscopy 8 ; however, the skill is difficult to acquire and requires specialized training. 9 Many different training systems have been designed and manufactured in order to enable trainees or surgeons to acquire some skill in handling the dedicated equipment and performing laparoscopic surgical procedures. Different training systems can be separated into physical simulation (box trainer or animal model) and systems that use virtual software.
Any kind of motor skill learning can be divided into three phases10,11: the cognitive phase, where the trainee tries to understand the different steps of the task; the associative phase, where he or she practices the skill, integrating the knowledge of the task into the appropriate motor behavior; and, finally, the autonomous phase, where the skill is performed without cognitive awareness.
The objective of this article is to present the data of a 5-day laparoscopic suture course by using the learning model based on three stages and the “gladiator rule” for the packaging of the intracorporeal surgeon's knot.
Materials and Methods
The study population consisted of specialists and residents in gynecology, general surgery, and urology. Forty-four doctors (33 men [75%] and 11 women [25%]) were enrolled. Mean age was 36.95 years (range, 25–55 years). Among trainees, 17 (38.6%) were residents, and 27 (61.4%) were specialists. Sixteen (36.4%) had previously attended at least one laparoscopic course on suturing technique. Eight (18.2%) were left-handed. Four (9.1%) had already practiced intracorporeal suturing in vivo.
A questionnaire concerning demographic information (age, gender, surgical training [surgeon or resident], previous course attendance, and dominant hand) was administered. The entire research was conducted at the High School of Laparoscopy and Minimally Invasive Surgery in the Centro Oncologico Fiorentino, Sesto Fiorentino, Italy, during four training courses for laparoscopic suturing skills held between September 2009 and December 2010.
All subjects attended a 5-day course, consisting of a 4-hour theoretical session on intracorporeal suturing and knot-tying and 35 hours of practical sessions on inanimate pelvic training. The introductory theoretical session was organized in order to allow trainees to capture the cognitive part of the procedure of stitching and knotting. The “gladiator rule” of Romeo and Minelli 12 was used to teach intracorporeal suturing. Following this initial theoretical session, all subjects trained under supervision using a simulator in order to complete the associative phase. Finally, after the acquisition of surgical skill, all subjects were left alone in order to practice the stitching and knotting technique to complete the autonomous phase and improve ergonomics.
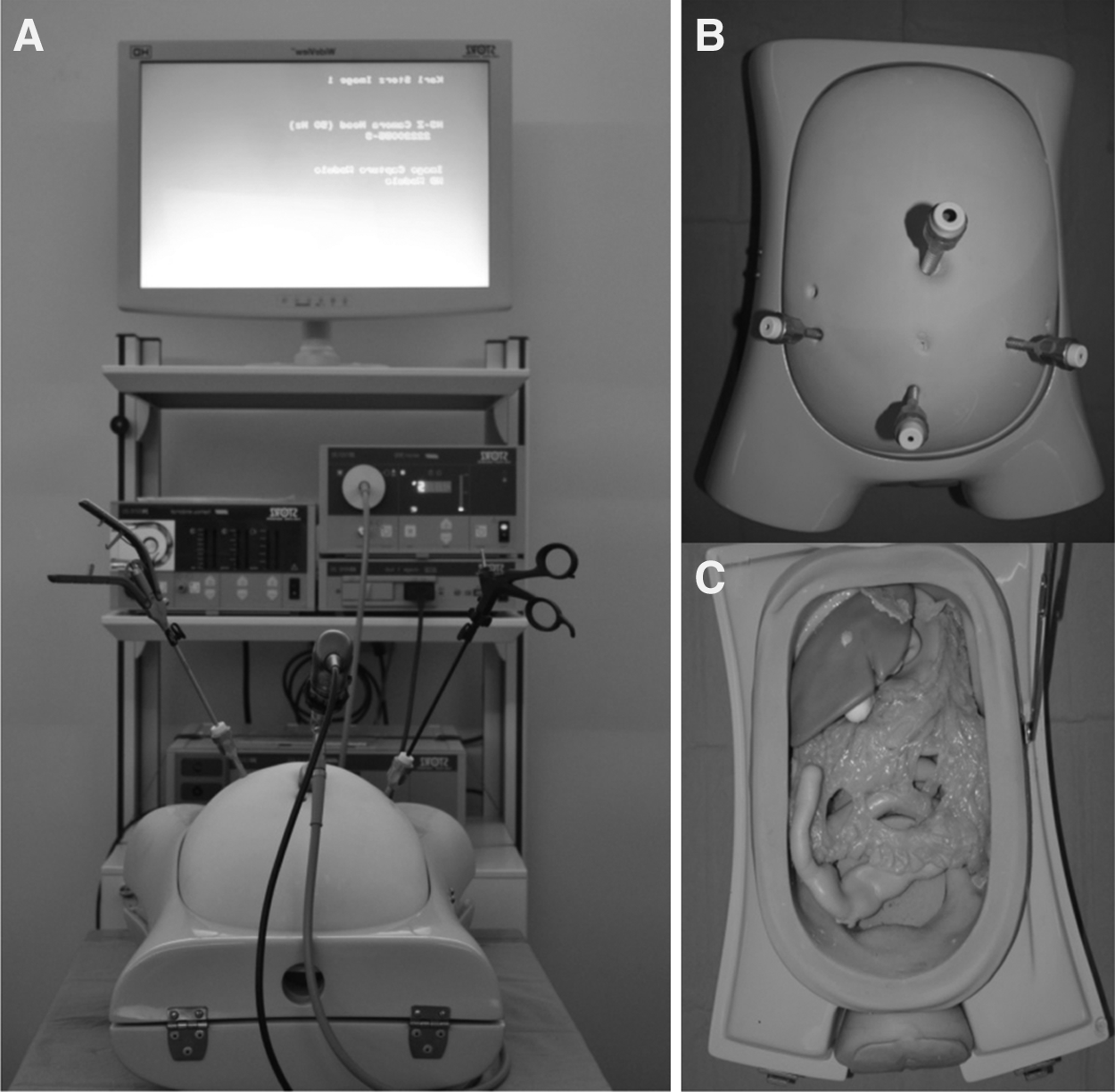
Each location consisted of a Wide View™ HD monitor (Karl Storz, Tuttlingen, Germany) and a pelvic trainer (EVA II generation ETX A1 LAP; Pro Delphus, Pernambuco, Brazil). The model consisted of the multiple-suturing model ETXII (Pro Delphus) according to the exercise performed.
One transumbilical 12 mm-trocar and three 5-mm trocars (two lateral and one suprapubic) were introduced through the ETX 10 abdominal wall (Pro Delphus). A 20-cm 2/0 polyglactin 910 suture (Vicryl®; Ethicon Inc., Johnson and Johnson, Somerville, NJ) on a half-circle cylindrical-section 27-mm needle was used. Laparoscopic instruments included one KOH Macro Needle Holder (introduced through the right-side trocar and moved by the right hand of the trainee), one Kelly forceps, and one scissors (Karl Storz) (introduced through the left side trocar and moved by the left hand of the trainee). Trainees' location and instrumentation are shown in Figure 1.
Training apparatus:
The “gladiator rule” of Romeo and Minelli 12 was used to teach the trainees to tie tight intracorporeal knots.
To tie an intracorporeal knot, it is important to perform the following steps in order:
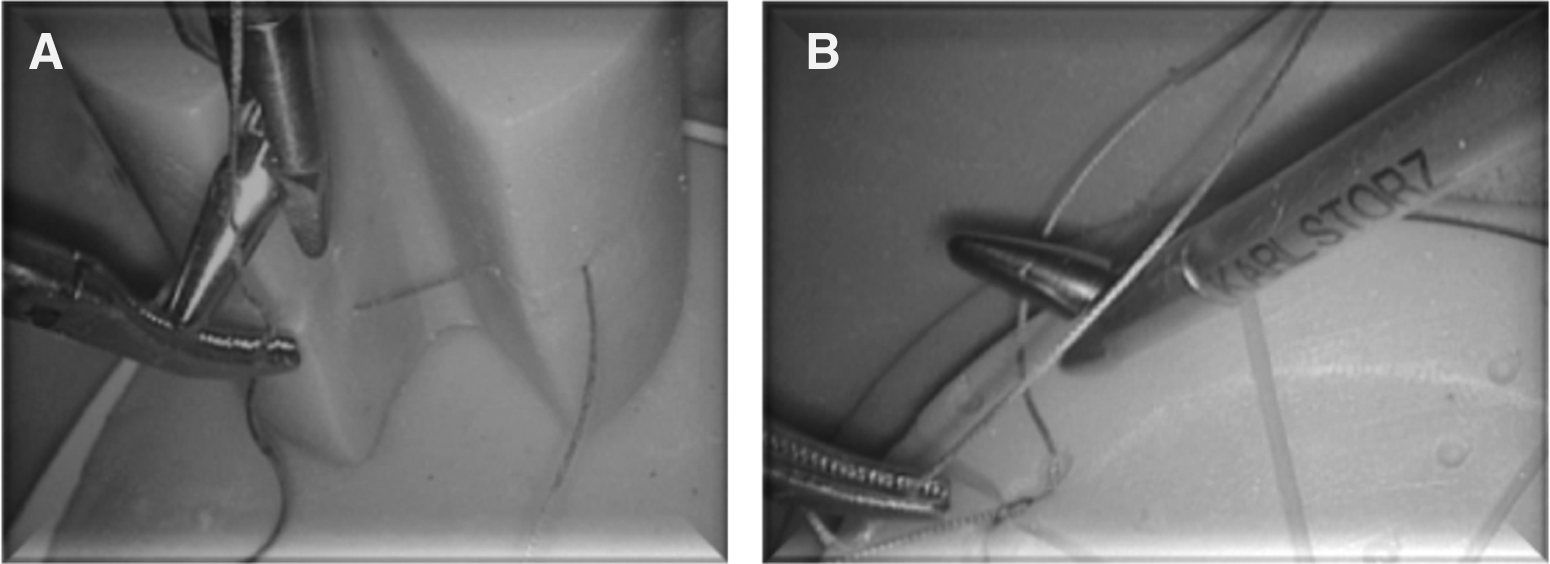
1. The assistant needle holder picks up the suture 2 cm from the needle. 2. The horizon, defined as the first part of the thread from the assistant needle holder grasp, is created (Fig. 2). 3. The needle holder with its open branches acts like the hand of a Roman Imperator, who saved or sentenced to death the gladiator by rotating his thumb (opening the moving branch of the needle holder) up or down, with a 180° rotation around the axis of the needle holder. 4. The needle holder passes behind the wire, called the horizon, with the movable branch open downward. The needle holder then rotates 180°, to return to its initial position. The movement is repeated so as to create two turns of wire around the needle holder. This is the basis for a double flat knot. The needle holder grasps the tail of the wire. The two ends are then pulled in opposite directions to create a double flat knot. 5. The “gladiator rule” is repeated a second time to fix the node. In this case, the open branch of the needle holder begins the winding with the movable branch open upwards, so as to create a reverse knot. The needle holder grasps the tail of the wire. The two ends are then pulled in opposite directions to fix the first knot. 6. The “gladiator rule” is repeated a third time to block the node. In this case, the open branch of the needle holder begins the winding with the movable branch open downwards, so as to create a knot similar to the first one. The needle holder grasps the tail of the wire. The two ends are then pulled in opposite directions to block the first and second knots.
Horizon:
This sequence of nodes is called a “blocking sequence” because if it is done correctly, it allows you to create a knot that will not untie.
Performance measure
Data about sense of depth, coordination, dexterity, traction power, and posture at the beginning and at the end of the course were evaluated by the tutor with a score from 1 (worst result) to 5 (best result). Each trainee performed three different practical exercises in order to test her or his skill in intracorporeal suturing at the end of the course.
The first exercise, called “carrots,” consists of performing the greatest number of singleton stitches with a surgical knot in a 15-minute period.
In the second exercise, called “tracks,” each trainee had to place a continuous suture using as many stitches as possible in a 15-minute period.
In the third exercise, called “cylinder,” each trainee had to perform a continuous suture along a vertical plane, using as many stitches as possible in a 15-minute period.
The tutor systematically controlled the quality and precision of the single stitches and the surgical knot.
Follow-up on subsequent live laparoscopic application of intracorporeal suturing was obtained.
Statistical analysis was performed using SPSS version 17.0 software (SPSS Inc., Chicago, IL). The efficacy of the course was evaluated with a descriptive analysis about absolute values, frequency, range, and mean, followed with a Student's t test. The variables analyzed were age, grouping age, sex, dominant hand, surgeon's training (surgeon or resident), depth, coordination ability, dexterity, power traction, ergonomy, and knot practical exercises (“carrots,” “tracks,” and “cylinder”). We assumed as statistically significant a value of P≤.05.
Results
Pretraining and post-training evaluation data about depth, coordination, dexterity, power traction, and posture were available for all trainees. Once the course was completed, we found a significant statistical improvement in depth (P=.017), coordination (P=.0001), dexterity (P<.001), traction power (P=.002), and posture (P=.003) among trainees, as shown in Table 1. The trainees' mean score improvement and standard deviation reduction demonstrated more homogeneous performances at the end of the course.
P<.05 was considered significant.
SD, standard deviation.
Table 2 describes univariate analysis of improvement before and after the course in the five parameters in relation to sex, age, dominant hand, surgical training (surgeon or resident), and previous course. Men upgraded in coordination (P=.002), dexterity (P<.001), and traction power (P=.014), whereas women increased only in traction power (P=.026). Trainees ≤45 years old had a statistically significant better performance in all the parameters evaluated: depth (P=.002), coordination (P=.001), dexterity (P<.001), traction power (P=.002), and posture (P=.004). Trainees >45 years old had no statistically significant difference in any of the parameters. Right hand dominant progressed in coordination (P=.001), dexterity (P=.001), traction power (P=.003), and posture (P=.023). Surgeons' performance improved in dexterity (P=.016), traction power (P=.008), and posture (P=.005), whereas residents' performance improved in coordination (P=.017) and dexterity (P=.002). Among trainees who had already attended laparoscopic courses we found a statistically significant improvement in traction power (P=.002) and posture (P=.001), whereas in the group that had not attended previous practical courses we detected improvement in coordination (P=.027), dexterity (P=.001), traction power (P=.038), and posture (P=.038) but not in sense of depth.
P<.05 was considered significant.
There was no statistically significant difference in the five parameters between men and women, ≤45 or >45 years old, right or left hand dominant, surgeon or resident, and previous course attendance or not except for surgical training, in that residents were better in coordination than surgeons (1.12 vs. 1.48, P=.001).
Results of the three practical exercises performed are shown in Table 3. All participants were able to perform exercises without a statistically significant difference in terms of sex, age, surgical training (surgeon or resident), and previous courses except for dominant hand, for which we detected better results among right-handed trainees in cylinder exercise quality (P=.007).
P<.05 was considered significant.
SD, standard deviation.
Twenty-nine of 40 (72.5%) trainees after the course began to apply intracorporeal sutures in in vivo laparoscopic surgeries. Four trainees had already used laparoscopic sutures before the course.
Discussion
To master endoscopic surgical skills, surgeons must acquire skill-based behavior, rule-based behavior, and knowledge-based behavior through practice and experience. 13 All the following are required to perform laparoscopic surgery independently: spatial cognition and recognition of bimanual motion under a laparoscope, selecting the most precise approach or rule based on previous successes or failures, and the making of final decisions after planning how to manage an operation based on his or her experience and knowledge. Nevertheless, it is quite difficult to describe and explain to the trainee these techniques, which are closely related to each other. Traditionally, the trainee observes how the instructor operates and borrows the techniques he or she has observed. However, this method of instruction is not precise, and learning by the trainee is not sufficient with it. 14 The traditional training paradigm is being challenged by introduction of many new, complex procedures into surgical practice, which limits residents' training time, the cost of residency teaching in the operating room, and rising ethical concerns about learning on patients. 9 Nevertheless, dry-box training alone is not sufficient for clinical practice, which includes anatomical patterns, open surgical experience, methods of dissection, and decision-making in complex cases. These must be experienced step-by-step and acquired from wet laboratory or clinical practice with an experienced mentor. 14 As a result, the use of simulation for skills training outside the operating room has been embraced by national surgical organizations and is quickly becoming an integral part of surgical training. Simulation allows trainees to acquire new skills and learn new procedures on inanimate models in a safe and nonthreatening environment before performing these tasks on patients. 9
Many educational theories have been postulated. The laparoscopic suturing training courses of the High School of Laparoscopy and Minimally Invasive Surgery are structured following the idea of Rogers et al., 10 that any kind of motor skill learning should be divided into three phases: (1) the cognitive phase (lessons during which the standardized method for stitching and knotting is taught and the trainee learns the different steps of the technique); (2) the associative phase (a practical session on the pelvic trainer in which specific exercises are performed by the trainees under tutorial control in order to integrate theory and motor behavior); and (3) the autonomous phase (a practical examination session during which trainees have to do intracorporeal suturing simulating real situations without tutorial control; the skill is performed without cognitive awareness).
The main factors affecting intracorporeal suturing skill are precision of the stitch and ability to perform surgical knots. In the present work we demonstrate that our method led all doctors, at the end of the course, to be able to achieve proficiency.
The ability of stitching depends on the capability of needle positioning and correctness of the movement evaluated through depth sensation, coordination, dexterity, traction power, and posture. During the 5-day course we evaluated a statistically significant improvement of these parameters among all the trainees but with better results in the group of residents; reasonable skill retention was seen for these novice trainees, even without any clinical or laboratory-based training. These results agreed with data previous reported by Van Bruwaene et al. 6 Teaching this skill in the early stages of the curriculum is feasible and it is will hoped will lead to increase training opportunities in the operating room.
Surgical knot execution depends on the technique and the correct sequence. For this reason the knowledge and the application of the “gladiator rule” are fundamental to obtain the correct execution of intracorporeal stitching and knotting. With the three practical exercises (“carrots,” “tracks,” and “cylinder”) performed at the end of the course, we could check the autonomy, the quality, and the rapidity of performing intracorporeal sutures. Performing a task rapidly does not necessarily imply that the procedure was performed more skillfully and thus with a greater likelihood of a positive clinical outcome. When a scenario is imagined that requires delicate and precise movement in a remote and critical area of the body, the simple measurement of total time elapsed may be an inadequate parameter of performance. 15 To address this issue we introduced a numerical score by the tutor to check the quality of the single stitch at the end of each exercise. All participants were able to perform exercises without a statistically significant difference among the different subgroups.
Like others authors,6,13 we believe that it is fundamental to learn intracorporeal suturing at the beginning of the endoscopic learning curve and not only in the case of a skilled endoscopist. In fact, it has to be considered that also during basic operative procedures the surgeon might unexpectedly need the skill of intracorporeal suturing. The technique taught during this kind of course, as demonstrated in the present work, is fundamental to improve dexterity and coordination, especially among nonexpert laparoscopists.
In accordance with Rosser et al., 16 we have demonstrated that at the end of the course both specialists and residents without laparoscopic experience achieved proficiency without a statistically significant difference in number and resilience of stitches, creating less dispersion and more homogeneous scores.
The cylinder exercise shows that right-handed trainees improved more than left-handed because of their position at the left of the patient. It could be possible to obtain an opposite result if the left-hand dominant surgeon is positioned at the patient's right.
Some authors6,14 believe that the presence of a tutor during the practical session inhibits intrinsic learning strategies and problem-solving activities, resulting in a lower performance. We do not agree with this idea, and we consider the presence of a tutor able to correct mistakes during the session and to explain tricks to overcome the difficulties to be fundamental. O'Connor et al. 3 have already underlined that the presence of a tutor motivates trainees, accelerates the learning curve, and creates an anxiety situation similar to live surgery.
In examining the training curves of all individuals, it can be seen that all reached a plateau within 5 days of the course. In total, 35 hours of practical training on the pelvic trainer was provided to each individual. This information could prove to be extremely valuable when building an efficient surgical skills acquisition curriculum.
We strongly believe that a laparoscopic suturing technique can be learned on the inanimate pelvic trainer following a structured practical training. Twenty-nine of 40 (72.5%) doctors have been able to apply in vivo intracorporeal sutures after this course, demonstrating the efficacy of the method. It is extremely important that during the course the trainees will learn:
1. The reproducible and clear theoretical rule 2. A suturing technique applicable in practical exercises 3. Autonomous control of the technique
In conclusion, the present study demonstrates the utility of a 5-day suturing course in teaching the laparoscopic suturing technique. The “gladiator rule” is a useful and reproducible strategy to teach intracorporeal knots. The three-step model allows to the majority of the trainees to apply laparoscopic suturing in vivo.
Footnotes
Disclosure Statement
Laparoscopic instruments have been provided by Karl Storz, Germany. A.R. is an employee of Karl Storz America do Sul. L.M., G.C., E.D.A.F., V.C., A.P., and L.M. declare no competing financial interests.