
Abstract
Abstract
Background:
Intraluminal erosion of a laparoscopic gastric band into the stomach has been reported as a complication of laparoscopic adjustable gastric banding. To our knowledge, however, intraluminal erosion of the band tubing into the duodenum has not been described.
Patient and Methods:
We report a 46-year-old man in whom a laparoscopic adjustable gastric band tubing eroded into the duodenal lumen, causing recurrent port-site infections. This complication was diagnosed on upper endoscopy and also, in retrospect, on an upper gastrointestinal barium study and computed tomography.
Results:
The patient underwent surgical removal of the band and tubing, with a primary duodenal repair, and made a complete recovery without complications.
Conclusion:
Erosion of laparoscopic band tubing into the duodenum should be included in the differential diagnosis for recurrent port-site infections after laparoscopic adjustable gastric banding. Radiographic or endoscopic visualization of the intraluminal portion of the tubing may be required for confirmation. Definitive treatment of this complication entails surgical removal of the tubing from the duodenum.
Introduction
Complications unique to LAGB are related primarily to the device components and include band slippage, port-site infections, and leakage of the band, port, or tubing. Intraluminal erosion of the band into the stomach is a much rarer complication, 3 and, to our knowledge, intraluminal erosion of the band tubing into the duodenum has not been reported. We present an unusual case of a capped, patent LAGB connecting tube that migrated into the duodenal lumen, causing repeated port-site infections. In the past, endoscopy has been advocated for patients with recurrent port-site infections to rule out erosion of the band into the stomach as the underlying cause. Based on our experience, we recommend endoscopy as well as radiographic imaging tests such as an upper gastrointestinal barium study or abdominal computed tomography (CT) to rule out erosion of the band tubing into the duodenum as a cause of recurrent port-site infections.
Patient and Methods
A 46 year-old man with morbid obesity (weighing 374 lbs and height of 5 feet 8.5 inches, yielding a body mass index of 56 kg/m2) underwent LAGB (standard-size LAP-BAND®; Allergan, Irvine, CA) in April 2009 at an outside medical facility. One week after discharge, the patient developed a wound infection at the site of his subcutaneous port. He subsequently developed repeated port-site infections, necessitating revision of the port in June 2009 and removal of the port (but not the tubing) in October 2009 at an outside facility. During the second procedure, the residual tubing was returned to the peritoneal cavity through a narrow tunnel.
In April 2010, the patient (who had lost 61 lbs [weight of 313 lbs and body mass index of 46.2 kg/m2]) presented to our outpatient clinic with a persistent wound infection and purulent drainage around his previous port site. A small amount of pus was aspirated from the wound and sent for cultures, which grew rare Staphylococcus aureus. An upper gastrointestinal barium study and an abdominal CT scan showed that the proximal end of the residual tubing was connected to the band and that the distal free end entered the anterior abdominal wall with gas and soft tissue stranding in an adjacent inflammatory collection (Fig. 1a). The tubing did not appear to have eroded into the gastric lumen, and no leaks were found. In retrospect, however, the band tubing was seen to enter the lumen of the duodenum on CT (Fig. 1b).
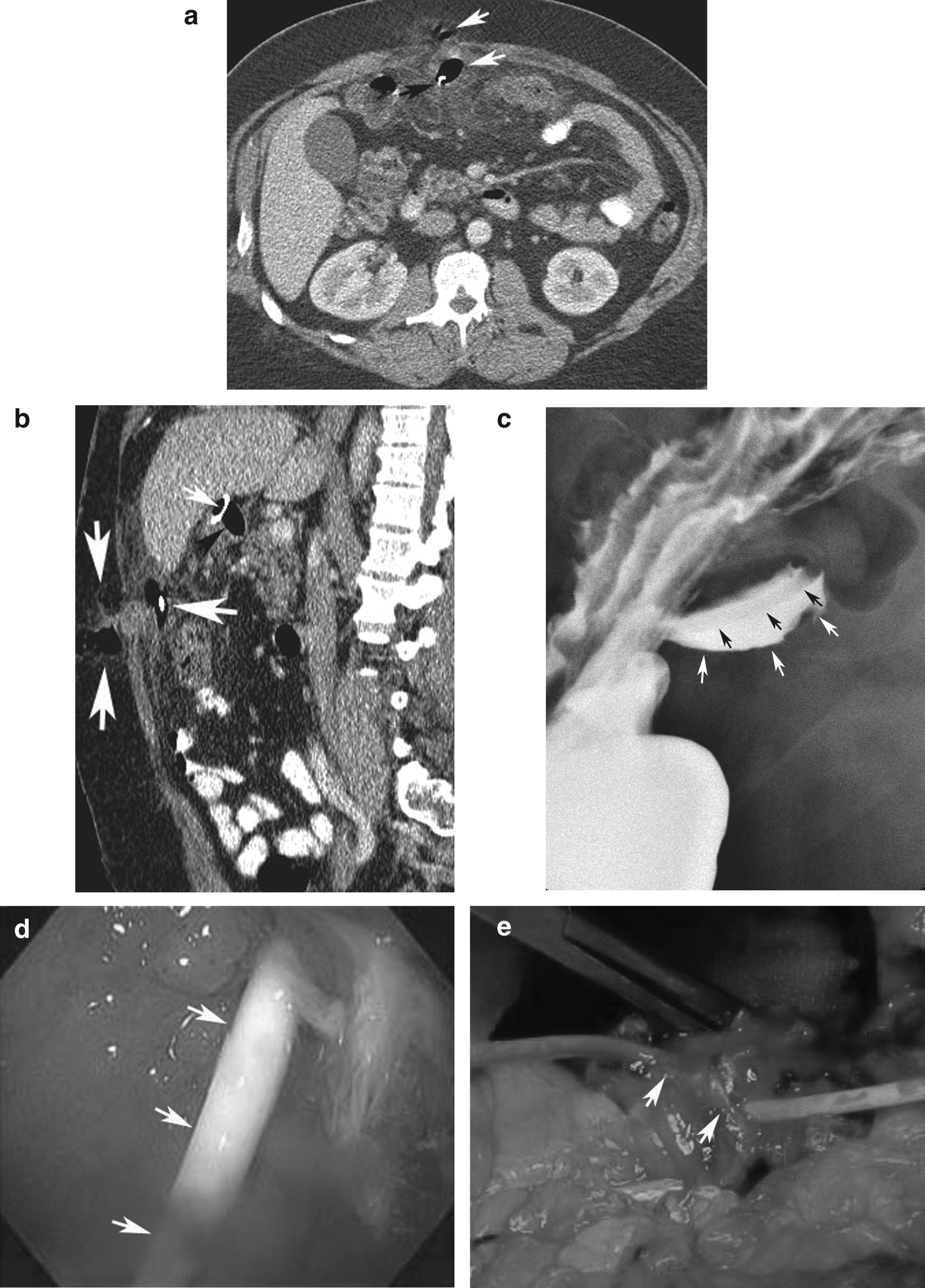
Intraluminal erosion of laparoscopic band tubing into the duodenum in a 46-year-old man with recurrent port-site infections.
The findings on the imaging studies raised concern that the infection at the previous port site was caused by a persistent sinus tract from the free end of the connective tubing in the anterior abdominal wall. In May 2010, outpatient diagnostic laparoscopy showed that the free end of the tubing was encased in an inflammatory rind and firmly attached to the anterior abdominal wall. The tubing was mobilized and released from the abdominal wall, capped with a specifically designed cap from the LAP-BAND kit, and placed in the abdominal cavity with excision of surrounding inflammatory tissue in the anterior abdominal wall wound, drainage of an adjacent abscess collection, and packing of the wound.
The patient returned to our outpatient clinic 7 months later with continued purulent drainage from the previous port site. Because of the chronic nature of the infection, a wound exploration was performed in December 2010, at which time the wound was excised and the Prolene® (Ethicon Endosurgery, Somerville, NJ) suture securing the connective tubing was removed. The tubing was then repositioned in the abdominal cavity, and the wound was closed.
The patient's postoperative course was uneventful until January 2011, at which time there was additional purulent drainage from the wound, raising concern that these recurrent wound infections were caused by erosion of the band or tubing into stomach or bowel. A repeat barium study showed the band in place without evidence of obstruction or distal band slippage.
The band tubing was seen coursing toward the anterior abdominal wall. In a retrospective review, however, the band tubing was surrounded by barium in the proximal duodenum, indicating an intraluminal location (Fig. 1c). Upper endoscopy confirmed that the band tubing had eroded into the lumen of the proximal descending duodenum just distal to the duodenal bulb (Fig. 1d). Because of this finding, the patient was taken to the operating room for surgical removal of the laparoscopic band and tubing.
Results
In February 2011, a midline laparotomy was performed. The tubing was traced through dense inflammatory tissue extending from the anterior abdominal wall to the duodenum, where it entered the lumen of the postbulbar descending duodenum, with visualization of clear entry and exit sites of the tubing in this portion of the duodenum (Fig. 1e). The band and connective tubing were removed, and a primary duodenal repair was performed.
When the connective tubing was removed, a thin mucosal layer was seen to bridge the entry and exit sites of the tubing in the duodenum, which was resected to release the tubing. The resulting 1.5-×1.5-cm defect was closed in two layers, using 3-0 Maxon™ (Covidien, Mansfield, MA) and 2-0 silk sutures. The repair was reinforced with an omental patch, and two Jackson-Pratt drains were placed in this region. Portions of the omentum and the infected tract were sent for pathology, which showed dense fibrous tissue with extensive acute and chronic inflammatory and granulation tissue.
The patient had a nasogastric tube in place until postoperative Day 3 and remained nil per os (nothing by mouth) until postoperative Day 7, when he underwent a follow-up water-soluble contrast study that showed no evidence of a leak. The patient's diet was advanced, and he was discharged from the hospital in satisfactory condition on postoperative Day 8.
Discussion
Erosion of a laparoscopic band into the lumen of the stomach is a well-recognized complication of LAGB, occurring in 2%–28% of patients.3,4 Affected individuals may present with abdominal pain, weight gain, and port-site infections. 4 Erosion of the connecting tubing into the stomach is much rarer, and, to our knowledge, no cases of tube erosion into the duodenum have been reported, although anecdotal cases of tube erosion into the jejunum,5,6 colon,7–10 and renal hilum 11 have been described. In all but one of the reported cases, the distal end of the tubing was no longer connected to the subcutaneous port. Similarly, free-floating peritoneal dialysis catheters have been known to cause bowel perforation.12–14 These cases suggest it may not be prudent to place the free end of the tubing in the peritoneal cavity when the tubing is disconnected from the subcutaneous port because of recurrent port-site infections, as the presence of free tubing in the peritoneal cavity may increase the risk of bowel erosion by the tubing.
On the other hand, one of the reported patients had erosion of the connecting tubing into the jejunum despite attachment of one end of the tubing to the port and the other to the band, 5 so the band tubing can erode into the bowel even in the absence of a free end in the peritoneal cavity. Although the tubing in our patient had been disconnected from the port, the imaging and intraoperative findings revealed that the free end of the tubing was adherent to the anterior abdominal wall, so our case also shows how the tubing can erode into the bowel lumen even when the tube connections are effectively intact.
As more LAGBs are performed and the devices remain in patients for longer periods of time, there may be a greater number of complications related to the tubing, so a high index of suspicion will be needed to properly diagnose and treat intraluminal erosion of band tubing into the bowel. As in our patient, previously reported cases of tubing eroding into the bowel have been associated with recurrent port-site infections,5,8,10 underscoring the importance of having a high index of suspicion for this complication when a patient presents with recurrent infections of the subcutaneous port. In our patient, surgical removal of the band and connective tubing with primary repair of the duodenum was performed for definitive treatment of this complication.
Of the six reported cases in which the LAGB connecting tubing eroded into the bowel (either jejunum or colon), three were diagnosed by laparoscopy,5,6,8 two by abdominal CT,7,10 and one by endoscopy. 10 Another was diagnosed at the time of laparoscopy with the help of intraoperative fluoroscopy. 9 As any one diagnostic test may fail to detect intraluminal erosion of the tubing, we believe the work-up for recurrent port-site infections should include multiple imaging tests, including an upper gastrointestinal barium study and abdominal CT, which in our case, in retrospect, showed intraluminal erosion of the band tubing into the duodenum (Fig. 1b and c). If this complication is not seen on barium study or CT, endoscopy should be performed to document band erosion into the stomach or tubing erosion into the duodenum that has been missed on imaging studies (Fig. 1d). Because the connecting tubing can also erode into the colon, colonoscopy should be considered if CT and upper endoscopy both fail to show this complication. Diagnostic laparoscopy might also be considered in patients with persistent port-site infections who have no identified source on other imaging tests.
Conclusions
Erosion of LAGB tubing into the duodenum should be included in the differential diagnosis for recurrent port-site infections after LAGB. Radiographic or endoscopic visualization of the intraluminal portion of the tubing may be required for confirmation. Definitive treatment of this complication entails surgical removal of the tubing.
Footnotes
Disclosure Statement
No competing financial interests exist.