
Abstract
Abstract
Thoracoscopic repair of esophageal atresia has becoming the gold standard in many centers because it allows a better cosmetic result and avoids the musculoskeletal sequelae of a thoracotomy. Natural orifice translumenal endocopic surgery (NOTES) is a new surgical paradigm, and its human application has already been started in some procedures. In the present study, we explore the feasibility of performing an esophagoesophageal anastomosis using a single transthoracic single port combined with a peroral access in a rabbit model to simulate repair of esophageal atresia by hybrid NOTES in a human newborn. Adult male rabbits (Oryctolagus cuniculus, n=28) were used to perform the surgical protocol. We used a transthoracic telescope with a 3-mm working channel and a flexible endoscope with a 2.2-mm working channel by peroral access. We performed total esophagotomy with peroral scissors followed by an esophagoesophageal anastomosis achieved with a rigid transthoracic scope helped by the peroral operator. Extracorporeal transthoracic knots were performed to complete the anastomosis. The anastomoses were examined in loco and ex loco, after animal sacrifice. We successfully accomplished a complete esophageal anastomosis in all rabbits using a combination of transthoracic and peroral 3-mm instruments. This study provides important insights for a possible translation of hybrid NOTES to human newborns with esophageal atresia. Forward studies to accomplish their feasibility in human newborns will still be necessary.
Introduction
The transition of NOTES to humans has been limited by the inability to safely close the viscera wall. 8 Increasing numbers of reports are describing the use of hybrid NOTES or laparoscopy assisted by NOTES in humans. 9 Regarding pediatric surgery, the peroral route to thoracic procedures seems to be a very attractive approach. Our group previously showed in an adult porcine model that an esophagoesophageal anastomosis could be performed by hybrid NOTES using a peroral and thoracoscopic approach. 10 However, this study was designed to simulate a surgery in human adults and not to explore the feasibility of performing an esophagoesophageal anastomosis in a newborn with EA. In the present work, we tested the possibility of performing hybrid thoracoscopic and peroral NOTES in a rabbit model to simulate the human newborn.
Materials and Methods
Study design
This project was approved by the ethical review boards of Minho University (Braga, Portugal). We used 28 adult male rabbits (Oryctolagus cuniculus) as an experimental model for the human newborn. Twenty animals were used for the learning curve, and in eight animals the experimental protocol was achieved completely. The surgical procedure involved esophageal dissection, esophageal section, and esophagoesophageal anastomosis using a single transthoracic trocar assisted by a peroral access. The surgical instruments used in this protocol included a 10-mm trocar (Thoracoport®; Covidien), a 22 French (7.3-mm) rigid telescope with a 3-mm working channel (model 27092 AMA; Karl Storz), a 16 French (5.3-mm) flexible telescope with a 6.5-French (2.2-mm) working channel (model 11272 VP; Karl Storz), a 5-mm modified endotracheal tube with a valve system (model 112482; Rusch; Teleflex), 3-mm instruments (Karl Storz) consisting of a knot-pusher, scissors, needle holders, dissector, and grasping forceps, a 6 French (2-mm) nasogastric tube (model 12027183; Unomedical), and 5-0 polydioxanone wire (Ethicon).
Presurgical procedures
Adult male rabbits, weighting between 2 and 3 kg, were given a liquid diet 12 hours before the procedure. All procedures were performed using general anesthesia. Pre-anesthesia medication consisted of buprenorphine (0.03 mg/kg, s.c.) (Budale; Dechra) followed 1 hour later by ketamine (25 mg/kg, s.c.) (Imalgene 1000; Merial Portuguesa—Saúde Animal), and medetomidine hydrochloride (0.5 mg/kg, s.c.) (DorbeneVet, EsteveDomitor; Pfizer Saúde Animal). A venous access was obtained through an intravenous line placed in the marginal ear vein, and anesthesia was maintained with ketamine (10 mg/kg/hour, i.v.). All animals were sacrificed with a barbiturate overdose (sodium pentobarbital, 100 mg/kg, i.v.) (Eutasil; CevaSaúdeAnimal).
Ergonomics
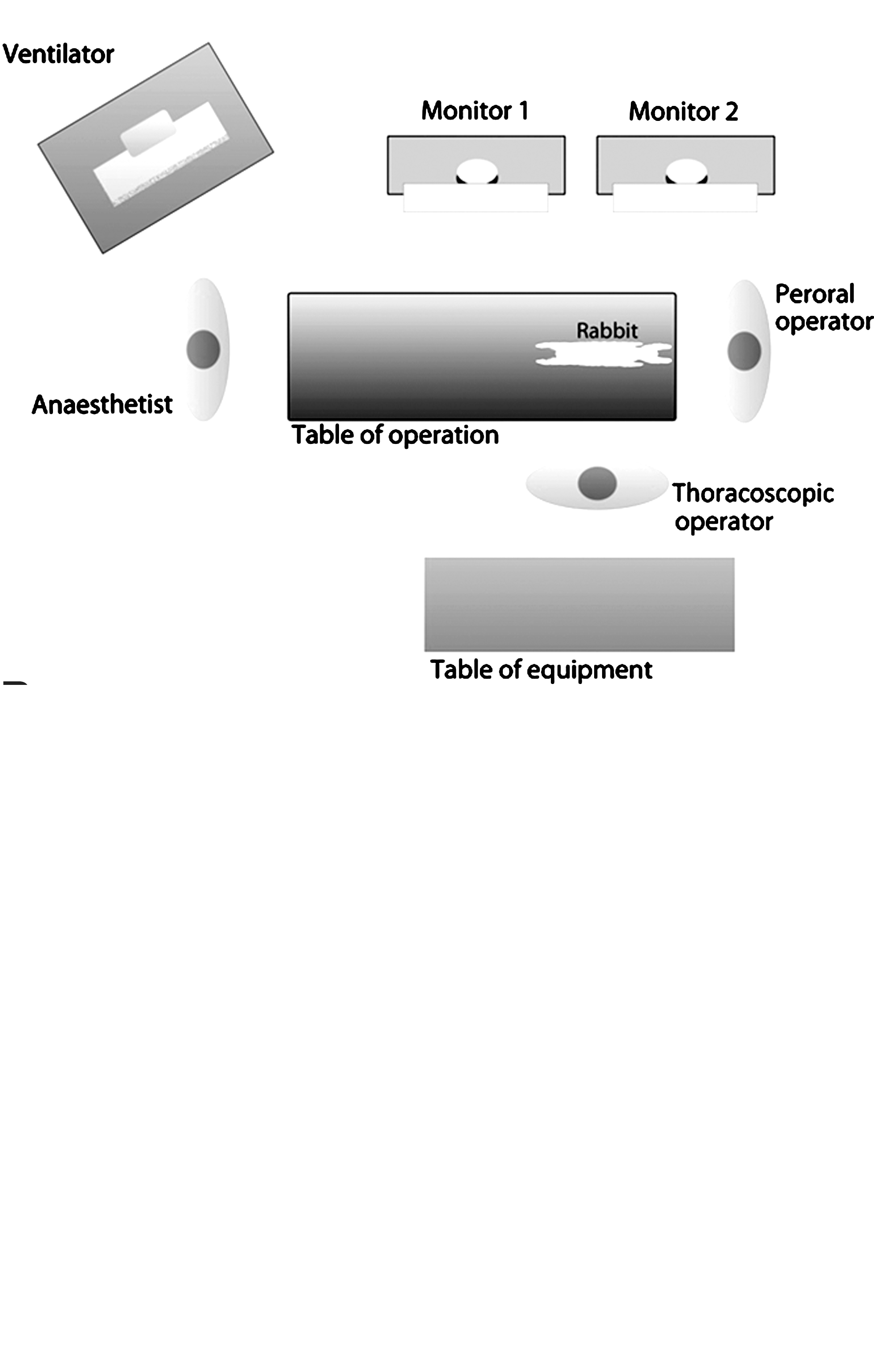
The layout of the room is represented in Figure 1. The animal was positioned at one end of the surgical table in the prone position. The thoracoscopic operator stood at one side of the operating table. The anesthetist and the peroral operator were positioned each one at one end side of the table. Monitors were positioned in front of each operator.
Surgical procedure
After the animal was put under general anesthesia, a tracheostomy was performed, and mechanical ventilation was started. The rabbits were placed in the prone position. A 10-mm transthoracic trocar was positioned immediately below to the lower end of the right scapula. The rigid telescope (thoracoscope) with 3-mm working channel and a CO2 insufflator (maximum pressure of 6 mm Hg) were used. The flexible telescope (endoscope) with a 6.5 French (2.2-mm) working channel was introduced through the mouth and moved to the esophagus. Esophageal dissection was carried out via the transthoracic approach using a 3-mm dissector forceps helped by the lateral and up-and-down movements performed by the peroral endoscope. A wire guide was introduced through the working channel of the peroral endoscope to the stomach, and the endoscope was removed. A modified 5-mm endotracheal tube with a valve system at the distal end was introduced until the proximal third of the esophagus and worked as an overtube or a flexible trocar. The esophagus was grasped near the distal end of the endotracheal tube using a 3-mm transthoracic dissector, and the esophagus was sectioned using the 3-mm peroral scissors. The distal portion of the sectioned esophagus was held by a 3-mm peroral dissector. The esophagoesophageal anastomosis was performed with 5-0 polydioxanone suture using a 3-mm transthoracic needle holder. The first esophagoesophageal stitch was passed in the posterior wall using a transthoracic needle holder helped by a peroral dissector in order to include all layers of the esophageal wall. All the knots were performed extracorporeally using a transthoracic knot-pusher. After two or three stitches on the posterior wall, a nasogastric tube was inserted through the mouth. In total, 7–10 single sutures were made. The rabbits were sacrificed after surgery. A segmental esophagectomy was performed to collect an esophageal section with the anastomosis, and its integrity was checked in its external and internal surface.
Results
Learning curve
During the learning curve we experienced several technical difficulties. We tested different trocars, instruments, and techniques of dissection, section, and anastomosis until we achieved the final surgical protocol presented above. One of the difficulties was related to the decrease of intrathoracic CO2 pressure after esophageal section and introduction of the modified endotracheal tube because a communication was opened between the mediastinum and the exterior through the esophagus. The problem was solved with the insertion of a valve system in the proximal end of the endotracheal tube. A technique to complete intracorporeal knots was developed, but it was abandoned because of its complexity and difficulty. We adopted the use of extracorporeal knots, which were simpler, faster, and more effective to accomplish esophageal anastomosis. Another difficulty was the intercostal hemorrhage caused during the manipulation of the suture needle that in most of the cases prevented the progression of the surgical procedure. This problem was solved after the team gained experience with the technique.
Surgical procedure
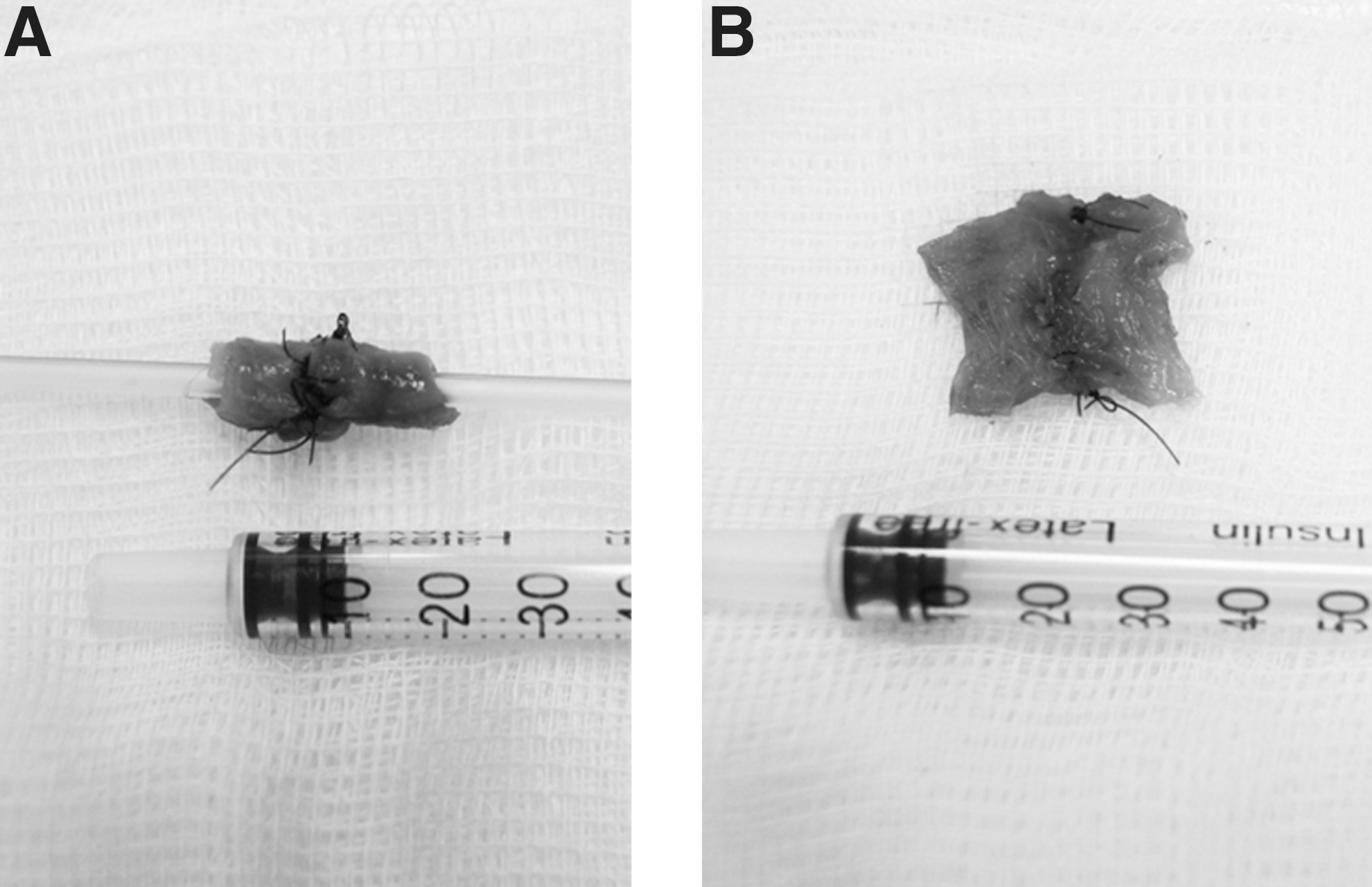
The surgical procedure is summarized step-by-step in Figure 2 and Supplementary Video (Supplementary Data are available online at www.liebertpub.com/lap). The lower end of the right scapula revealed an ideal access point to introduce the trocar. The location of the transthoracic port associated with the animal in the prone position and CO2 insufflation permitted us to obtain a good visualization of the esophagus without the need of other instruments or techniques. For the first three stitches, the peroral dissector was helpful in two aspects: (1) to put the distal esophageal end close to the proximal esophageal end and (2) to include all the layers of the esophageal wall in the sutures. The first stitch, in particular, was the most difficult to perform because of the lack of stability of the esophagus (Fig. 2F). A nasogastric tube was inserted after the first two to three stitches, turning the anastomosis easier and faster to perform (Fig. 2I and J). However, the insertion of the nasogastric tube was again a challenging step, requiring an optimal coordination between the thoracoscopic and peroral operators. The anastomosis procedure was completed dominantly by the transthoracic needle holder helped by peroral rotation of the esophagus. Extracorporeal knots were performed with a 3-mm knot-pusher inserted through the thoracoscope (Fig. 2G). This technique permitted us to obtain an optimal view of the knotting process, easily controlling the pressure applied to each knot, and to decrease operative time. The remaining wire was cut transthoracically without any difficulty. Pearls and pitfalls of the protocol identified by the group are summarized in Table 1. The mean time to perform the surgical procedure in the eight rabbits—including dissection, esophagotomy, and anastomosis—was 85 minutes (range, 62–137 minutes). At the end of the procedure, the final aspect of the anastomosis was properly checked (Fig. 2L). Additional stitches were performed as much as necessary. The manipulation of the instruments needs to be cautious because of the proximity with the intercostal vascular structures. After sacrificing the animals, we performed a segmental esophagectomy to study the anastomosis closely. We verified a complete anastomosis in all cases, with the incorporation of the mucosa in all stitches (Fig. 3).
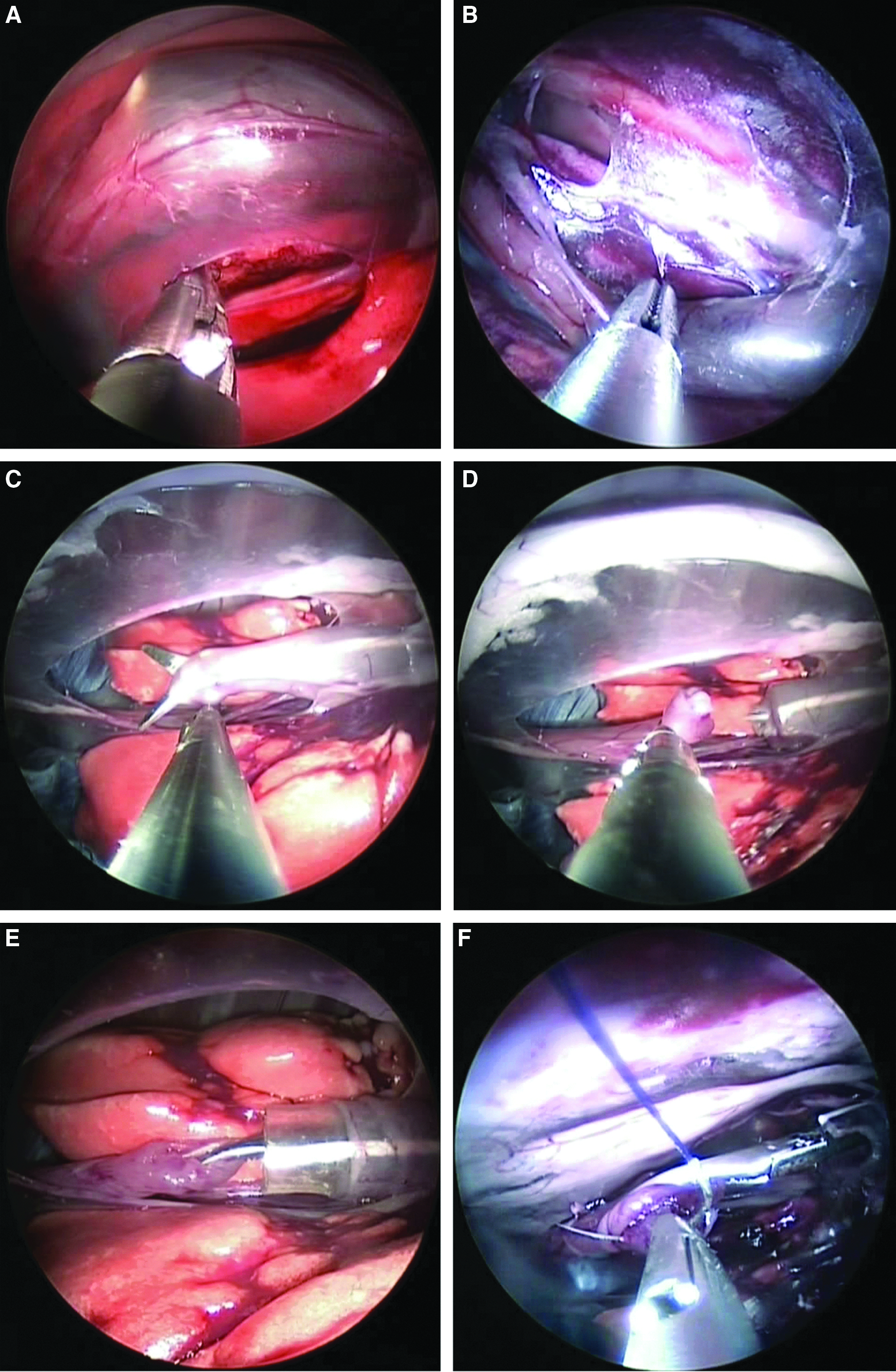
Major steps executed during the protocol. Dissection was performed by the transthoracic operator, whereas the peroral operator accessed the esophageal lumen with a flexible endoscope, permitting him to take lateral movements and
Discussion
Thoracoscopic repair of EA includes obvious advantages like better visualization of the surgical field, less postoperative pain, better cosmesis, and fewer musculoskeletal sequelae. 4 Some studies, including one multicenter analysis, suggested that thoracoscopic correction of EA with TEF can be safely performed by experienced surgeons and had comparable outcomes with thoracotomy. 4 Currently, this surgical technique is becoming the gold standard for EA correction in several centers.4,5 However, a new era is emerging, and three or four transthoracic ports might be too much for a 21st century minimally invasive procedure. Although the first NOTES approach was a transvaginal procedure described by Decker and Cherry 11 in 1944, the enthusiasm about this technique only started six decades later. Starting in 2004 with a human transgastric appendectomy performed by Reddy and Rao, 12 NOTES brought a new set of opportunities. All possible approaches were explored: transgastric, 13 transvesical, 14 transcolonic, 15 and transesophageal 16 accesses. The potential advantages of NOTES over laparoscopy and thoracoscopy might include (1) reduction of general anesthesia use, (2) decrease in hospitalization time and postoperative pain, (3) prevention of skin incision complications (wound infection and hernias), (4) increment of outpatient regimen, (5) faster return of bowel function, (6) better cosmetic outcomes, and (7) increase in overall patient satisfaction. 9 Besides all these advantages, pure NOTES still has some limitations in the present.
A pure peroral approach might have some disadvantages like the extreme difficulty of creating triangulation, the precarious view of the work field, and, concomitantly, the increased risk of leakage resulting from an incomplete esophageal closure. Hybrid NOTES represents the best of the two fields—thoracoscopy and NOTES—because it allows a reduction of the number of transthoracic ports and overrides some of the limitations of pure NOTES. Using a transthoracic access combined with a peroral route, triangulation and countertraction can be achieved. Moreover, the excellent thoracoscopic visualization of the work field is profitable, and the thoracic incision can be used to place a drainage tube postoperatively.
EA can be an excellent congenital malformation candidate for peroral hybrid NOTES. At present, the upper esophageal pouch is only used for the introduction of the nasogastric tube, but in our opinion the upper esophageal pouch could potentially be a route for the thoracic cavity. Rolanda et al. 10 described a peroral esophageal segmentectomy and an anastomosis with a single 12-mm transthoracic trocar in an adult porcine model. The authors demonstrated the reliability of performing this technique in a large animal model. In the present study, we demonstrated the feasibility of combining the peroral and transthoracic routes to perform an esophagoesophageal anastomosis in rabbits. This animal model perfectly simulates the human newborn and is a well-established model to train pediatric surgeons in neonatal minimally invasive procedures. 17 The anatomic constitution of the rabbit simulates the newborn size, allowing the use of 3-mm instruments in a very limited space, as happens in human newborns. In this work, we explored the prone position of the animal to amplify our field of work. The prone position is being explored in patients in order to easily manipulate the esophagus. 18 This approach was previously explored in our department by Rolanda et al., 10 stating the advantage to easily access the mediastinum with the help of the gravity, to use lower CO2 pressures, and to decrease the time of the procedure. In thoracoscopic repair of EA, different centers are using the partially prone position of the patient at 30–45°,4,19 and a fourth port is sometimes applied to retract the lungs.4,19 A completely prone position may be more helpful than a partial one.
The great innovation of this study is the possibility of performing an EA correction with just one transthoracic port, in contrast to the classic thoracoscopy, which uses three or four trocars.4,19 The use of a 10-mm trocar might be considered more invasive than three 5-mm trocars but still is a single incision. This trocar size was used to introduce the camera with the working channel. We might anticipate that the miniaturization of this kind of telescope will allow the use of smaller trocars in the future. The peroral flexible endoscope allowed us to achieve the esophageal lumen without difficulties and to easily mobilize it. The three-dimensional movements of the flexible endoscope allowed us to surpass the inconvenience of using just one transthoracic trocar to perform esophageal dissection. In a human newborn with EA, we might anticipate that this peroral approach could facilitate transthoracic dissection of the upper esophageal pouch. Additionally, cutting the proximal pouch with peroral scissors could be of great help in human newborns. Again, the possibility of grasping the lower pouch using this access can be useful for the first esophageal stitch. In this study, the mean operative time was 85 minutes. The average surgical time for thoracoscopic repair of EA with TEF is 130 minutes, as was reported by a multi-institutional study. 4 In the present study we did not perform dissection and ligation of the distal TEF, but we could anticipate that using a peroral gasper combined by a transthoracic dissector, it would be possible to perform this step. We demonstrated the feasibility of an esophageal anastomosis using a single transthoracic trocar with a similar time interval as using three or four transthoracic trocars. This surgical technique, combining peroral and transthoracic approaches, demands a well-synchronized performance between the surgeon and the first assistant to guarantee optimal results. Whereas in thoracoscopy or laparoscopy the same surgeon performs all the movements with both hands, in hybrid NOTES it is necessary to have an operator in each port. A good coordination between them is essential, permitting them to obtain synchronized movements as if the hands of each operator belonged to the same surgeon. Our team has already proved in other procedures, namely, cholecystectomy 6 and nephrectomy, 7 that the coordination between two operators is demanding but can be achieved with training.
We identified some limitations in the present study: (1) tracheostomy to ventilate rabbits and (2) lack of a true EA with TEF, the most common type of EA. During our learning curve, we abandoned the endotracheal intubation and started to perform tracheostomy to ventilate the animal. An endotracheal tube would make hard to introduce other instrumentation through the peroral route. To overcome this problem in humans, we suggest a nasotracheal tube, instead of using an orotracheal tube. The present work was a non-survival study using normal rabbits without EA. This fact did not allow us to explore the feasibility and safety of performing some technical procedures like TEF ligation. It might be important to simulate a TEF in an animal model or, ideally, translate this study to a deceased newborn with EA and distal TEF. Nevertheless, we believe in the viability of this approach in a human newborn because ligation of TEF is performed by many groups with a simple clip, 4 a maneuver that could be easily performed using transthoracic and peroral routes. This approach would imply a change in the surgical human routine—the first step would be the dissection and opening of the upper esophageal pouch to establish the peroral trocar before performing distal esophageal dissection and TEF ligation.
In conclusion, this is a proof-of-principle study that demonstrates the feasibility of performing an esophageal anastomosis combining a single transthoracic port with a peroral port in a rabbit model that simulates the human newborn. This study provides several important insights into the translation of hybrid NOTES repair for human newborns with EA. We anticipate that in the near future, the peroral route will replace at least one, if not two, transthoracic trocars.
Footnotes
Acknowledgments
This project was funded by a 2010 IPEG research grant.
Disclosure Statement
J.C.-P. is a consultant/adviser for Karl Storz (Tuttlingen, Germany). T.H.-C., T.R.S., A.M., and J.M.-P. declare no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.