
Abstract
Abstract
Background:
Many have questioned whether the laparoscopic, percutaneous hernia repair technique is as durable as an open repair in which the sac is divided and ligated. We set out to assess if the suture alone causes enough injury and scar over time to obliterate the internal ring.
Materials and Methods:
In total, 28 male rabbits with congenital patent processus vaginalis underwent laparoscopic repair with the subcutaneous endoscopically assisted ligation technique. For Group 1 the repairs were evaluated laparoscopically at predetermined time points before and after removal of the ligating suture. Group 2 assessed the effect of sharp peritoneal trauma at the time of repair and was evaluated at 2 and 4 weeks.
Results:
When durability of repair with suture alone was evaluated, all repairs failed after insufflation to 35 mm Hg after suture removal out to a time point of 12 weeks. In the peritoneal trauma group, at the 2- and 4-week survival time point, 87.5% and 100%, respectively, of repairs remained intact after removal of suture. In contrast, only 25% and 12.5%, respectively, of defects remained closed in the animals repaired with suture ligation alone.
Conclusions:
The laparoscopic, percutaneous hernia repair may rely heavily on the suture itself to prevent recurrence. In the event of suture failure, this could lead to an increasingly high recurrence rate. The addition of minor peritoneum trauma may induce sufficient scarring to provide a more durable repair.
Introduction
Others have proposed that the suture itself causes ischemia of the peritoneum and thus eventual scar formation. If in fact injury of the sac and scar formation lead to durability of repair, it may be more effective to cause sac injury as part of the laparoscopic approach. Here we describe a double-armed study in rabbits comparing laparoscopic high ligation with suture alone with laparoscopic high ligation with suture and the addition of injury to the anterior portion of the internal ring. Our hypothesis is that repair with suture alone will not form an obliterative scar, thus relying on the suture for life, whereas the addition of injury to a portion of the sac will cause an obliterative scar of the hernia defect.
Materials and Methods
Male New Zealand White rabbits weighing from 2200 to 2400 g were selected for the procedure as they have a natural patent processus vaginalis. Prior to the start of this study the protocol was reviewed and approved by the Institutional Animal Care and Use Committee of Case Western Reserve University. Prior to surgical repair, rabbits were acclimated to their housing for 7 days. Induction of general anesthesia was obtained with a subcutaneous injection of anesthetic cocktail (ketamine [4.3 mg/kg], xylazine [0.86 mg/kg], and acepromazine [0.07 mg/kg]). Anesthesia was maintained throughout the procedure with inhaled isoflurane at 1.5%–5% delivered via a secured nose and mouth cone. After appropriate anesthesia was obtained the abdomen was clipped free from hair and then prepped in a sterile fashion with 70% chlorhexadine scrub.
For laparoscopic access, a single 5-mm laparoscopic port was placed via a Hassan technique in the area of the umbilicus. The abdomen was insufflated with CO2 to a pressure of 4 mm Hg, and a 5-mm 30° laparoscope was then introduced through the umbilical port. Two additional 5-mm working ports were then placed approximately 3–4 cm lateral and inferior to the umbilical port, which were used to facilitate adequate visualization of the hernia defect. Prior to suture repair of the defect, the testicle was internalized; this step is completed because in a rabbit (as opposed to a human) the spermatic cord is intraperitoneal and passes directly through the defect. To perform this step, the testicle is internalized using a grasper, and the gubernaculum is then transected using an electrocautery device (LigaSure™; Covidien, Mansfield, MA).
Animal randomization
In total, 28 rabbits were involved in the study and divided into two groups. Twelve rabbits were included in the first group of the study, which was an initial observational study to evaluate if a specific period of time was necessary for the hernia repair to heal. The second group of the study was used to determine if peritoneal trauma would influence the hernia repair and included 16 rabbits. Animals were randomized within Group 1 or 2 prior to induction of general anesthesia.
Group 1: time to heal
After the testicle was internalized, the defect was repaired using the subcutaneous endoscopically assisted ligation (SEAL) technique previously described.3,4 In brief, a single monofilament 3-0 polypropylene suture is passed transcutaneously under endoscopic guidance. It is directed around the hernia defect, taking care to stay extraperitoneal. A small segment in the inferior aspect of the defect is skipped over to simulate the technique used by some pediatric surgeons to avoid potential injury to the spermatic cord in humans. The suture is then continued out through the skin and passed tail first subcutaneously to exit at the same point as the original suture placement. This is tied down under direct visualization closing the hernia defect. This technique was then repeated on the opposite side. Animals were evaluated at 1, 2, 4, 6, 8, and 12 weeks.
Group 2: evaluation of scar
Group 2 studied the effect of sharply traumatizing the peritoneum on the ability of the ligation to form a permanent scar. Animals were randomized to traditional repair on one side and repair plus sharp trauma on the opposite side. Trauma was caused by using laparoscopic shears to sharply incise the peritoneum around 75% of the circumference in the area of the internal ring. The inferior portion of the hernia defect was left intact to simulate where the spermatic cord would travel in humans. Both defects were closed in a similar fashion as described above with a 3-0 monofilament permanent suture at the level of the internal ring, just proximal to the area of trauma. Animals were evaluated at 2 and 4 weeks.
Evaluation of repair
At the predetermined time point the animal was anesthetized with a subcutaneous injection of anesthetic cocktail; following this, the animal was euthanized with an intravenous injection of pentobarbital sodium (Fatal-Plus®; Vortech Pharmaceuticals, Dearborn, MI). Laparoscopic access to the abdomen was obtained by placing a 5-mm umbilical port in a standard Hassan fashion. The abdomen was insuflated to 4 mm Hg, and the area of repair was evaluated to determine the presence of any breakdown. The insufflation pressure was gradually increased in 5 mm Hg increments to a goal of 35 mm Hg. Any breakdown of the repair was recorded and, if it happened, at what pressure point it occurred. If the repair remained intact the pressure was reduced, and the camera was removed. At this point the Prolene™ (Ethicon Endo-Surgery, Blue Ash, OH) suture was removed by cutting the subcutaneous knot. The camera was reintroduced, and the pressure was again increased in 5 mm Hg increments to a goal of 35 mm Hg. If the repair failed, the pressure at which this occurred was recorded. In all animals, the suture was removed at the outset of the second laparoscopic assessment.
Results
There were no immediate postoperative complications, and all animals survived to their assigned time points.
Group 1: time to heal
At all time points (1, 2, 4, 6, 8, and 12 weeks) all repairs were intact upon initial evaluation and with increase of pressure to 35 mm Hg with the suture in place. However, after removal of the suture all repairs showed signs of failure at 5 mm Hg as defined as a visible opening of the defect. As the pressure was increased, the defects progressively enlarged.
Group 2: evaluation of scar
Eight animals were evaluated at the 2-week time point, and 8 animals were evaluated at the 4-week time point. Upon initial evaluation all repairs were intact with the suture in place. At the 2-week time point, after removal of the suture, 25% (2/8) of defects repaired with suture only remained closed after the pressure was increased to 35 mm Hg. In contrast, 87.5% (7/8) of defects repaired with peritoneal trauma and suture remained closed after suture removal and increasing to maximum pressure (Fig. 1).
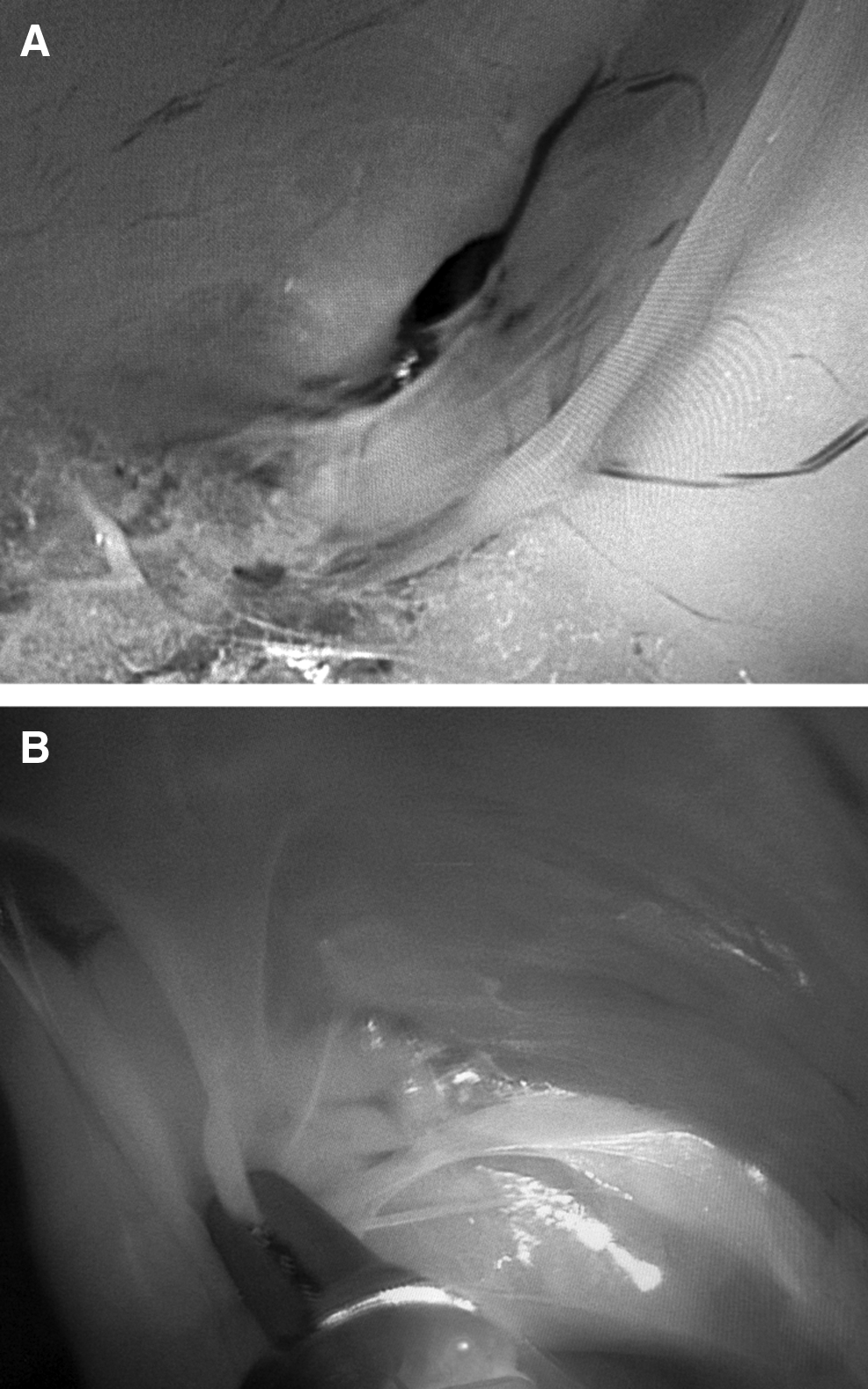
Example of laparoscopic evaluation of hernia defect in a rabbit model after suture removal at 2 week post-repair.
At the 4-week survival time point, only 12.5% (1/8) of defects repaired with suture only remained closed after suture removal and increasing the pressure to 35 mm Hg. All defects (100% [8/8]) repaired with peritoneal trauma and suture remained closed after suture removal with pressure increase to 35 mm Hg.
Discussion
This study served as a pilot to investigate the ability of a subcutaneous SEAL method of pediatric inguinal hernia repair to cause sufficient scarring to cause permanent obliteration of the hernia defect. Although this approach serves as a novel minimally invasive method of repair, studies have shown a variable rate of hernia recurrence from less than 1% to 5% following repair with this method.5–7 Using a rabbit model of patent processus vaginalis, we initially evaluated the time frame necessary for the suture alone to cause significant scarring and found that even out to 12 weeks post-ligation the defect reopened following suture removal. Thus, the suture did not cause sufficient scarring to obliterate the internal ring, and the closure was reliant on the suture alone even after 12 weeks. The second arm of the study served to evaluate the effect of injuring the peritoneum prior to suture placement and found that the addition of peritoneum trauma significantly increased the ability of suture to cause permanent scarring.
Historically, repair of pediatric inguinal hernias has been performed by an open approach and included ligating and dividing the hernia sac. It was thought that the combination of division and ligation of the sac resulted in sufficient long-term scarring of the defect, with small recurrence rates. Initial studies evaluating the percutaneous, laparoscopic hernia repair technique have resulted in varied rates of hernia recurrence. This knowledge led us to investigate the ability of this technique to cause adequate permanent scarring.
Our initial impression was that simply ligating the hernia sac would be sufficient to cause permanent scarring and closure of the defect. This mechanism of action was felt to be similar to the mechanism of a seton fistulotomy. However, in our timing arm of the study we found 100% failure out to 12 weeks postoperatively after suture removal. Understandably, in humans the suture is left in place; however, all sutures experience some form of degradation and are at risk for failure. 8 The high failure rate following suture removal leads us to recommend the use of a permanent suture if using any laparoscopic, percutaneous hernia repair technique. We elected to utilize monofilament suture, to facilitate suture removal at the time of evaluation; however, the use of a braided suture may induce greater inflammation, potentially improving the overall strength of repair, and could be evaluated in future studies.
The fact that we saw little scarring of the defect led us to evaluate the role of peritoneal trauma in initiating scarring of the peritoneum. The trauma was performed by sharply cutting the peritoneum in the area of the defect and then performing the laparoscopic, percutaneous hernia repair technique in the same manner as if we had not caused any trauma. Our results surprisingly demonstrated that the addition of minor peritoneum trauma significantly improved our repair success rate after removal of suture. The addition of peritoneal trauma to a laparoscopic, percutaneous hernia repair technique makes it most similar to an open repair in which the hernia sac is ligated, essentially inducing the same form of peritoneal trauma. Additionally, previous studies have demonstrated that peritoneal trauma leads to increased adhesions during abdominal surgery. 9
These findings also coincide with the findings reported by Marte et al. 10 They recently reported a retrospective review comparing two laparoscopic hernia repair techniques. The first group was repaired with suture ligation of the inguinal ring, whereas the second group utilized a lateral incision of the hernia sac of 1–2 cm in combination with suture ligation. They found a statistically significant reduction in hernia recurrence rate (3.76% versus 0%; P<.05) at a mean follow-up of 24 months.
Additionally, Esposito et al.11,12 have recently published their experience with laparoscopic pediatric inguinal hernia repair, and they used a method of repair similar to the one that we used in this study, in which prior to closing the defect, they circumferentially cut the peritoneum at the level of the internal ring. Using this method of peritoneal trauma, they have reduced their hernia recurrence rates from 3.4% to 0.6%. In our study, we found that in as little as 2 weeks, the addition of peritoneal trauma significantly reduced our defect failure rate compared with suture ligation alone.
In conclusion, although human trials have shown good short-term results with laparoscopic, percutaneous hernia repair techniques, our pilot study in a rabbit model demonstrates that this repair may rely heavily on the suture itself to prevent recurrence. In the event of suture failure, this could lead to an increasingly high recurrence rate. The addition of minor peritoneum trauma on the anterior aspect of the internal ring (away from the spermatic cord) may induce sufficient scarring to provide a more durable repair.
Footnotes
Disclosure Statement
J.A.B., K.C.H., D.M.K., K.B.K., and S.J.S. have no competing financial interests. T.A.P. serves as a consultant for Teleflex.