
Abstract
Abstract
Background:
Laparoscopic total mesorectal excision (LTME) for rectal cancer remains controversial. The aim of this meta-analysis of randomized controlled trials (RCTs) is to compare LTME and open total mesorectal excision (OTME) as the primary treatment for patients with middle and low rectal cancer with regard to short-term outcomes.
Materials and Methods:
Literature searches of electronic databases (PubMed, Embase, and the Cochrane Library) and manual searches up to October 30, 2011 were performed. Prospective randomized clinical trials were eligible if they included patients with middle and low rectal cancer treated by LTME versus OTME. Fixed and random effects models were used. Review Manager version 5.1 software was used for pooled estimates.
Results:
Four RCTs enrolling 624 participants (LTME group, 308 cases; OTME group, 316 cases) were included in the meta-analysis. LTME for rectal cancer was associated with a significantly longer operative time but significantly less intraoperative blood loss and earlier time to pass first flatus. We found no significant differences in the number of lymph nodes, overall morbidity, and perioperative mortality rates between the two groups. Time to resume liquid diet, time to resume normal diet, and length of hospital stay, although not significantly different between the two groups, did suggest a positive trend toward LTME.
Conclusions:
It may be concluded that LTME is a safe and effective alternative to OTME and is justifiable under the setting of clinical trials. Additional RCTs that compare LTME and OTME and investigate the long-term oncological outcomes of LTME are required to determine the advantages of LTME over OTME.
Introduction
Many clinical studies, including several randomized controlled trials (RCTs),3–6 systematic reviews,11–13 and a meta-analysis, 14 have drawn the conclusion that laparoscopic surgery for colon cancer is safe and feasible and can yield better postoperative recovery and equivalent long-term outcomes.
Compared with laparoscopic colectomy, laparoscopic rectectomy is more complex and technically demanding, and it is characterized by a steep learning curve with protracted operating times. Therefore, rectal cancer was not included in earlier studies on laparoscopic versus open resection for colorectal cancer. Patients with rectal cancer were excluded from the majority of randomized clinical trials or represented only a small proportion of patients recruited; to date, the number of prospective randomized trials specifically focusing on middle and low rectal cancer is limited. Although some studies15–18 have demonstrated that laparoscopic surgery has the same benefits for rectal cancer as laparoscopic surgery has for colon cancer, because of the limited amount of available data in the literature and technical difficulties, 19 most surgeons are skeptical about the oncological value of laparoscopic total mesorectal excision (LTME), the adequacy of cancer margins, and long-term outcomes. However, many colorectal surgeons who practice laparoscopic surgery soon appreciated that the improved optics of laparoscopy can provide a much better view of the pelvis, and the Heald principle of meticulous sharp dissection for total mesorectal excision could be performed without compromise. 20 With the advances in technology and more technique and experience of surgeons, the application of LTME for rectal cancer has recently become more widespread. In recent years, there have been increasing numbers of reports on LTME for rectal cancers. Meta-analysis can be used to evaluate the existing literature in both a qualitative and quantitative way by comparing and integrating the results of different studies and taking into account variations in characteristics that can influence the overall estimate of the outcome of interest. The goal of this meta-analysis is to assess the safety and efficacy of LTME for middle and low rectal cancer compared with open total mesorectal excision (OTME).
Materials and Methods
Study selection
A PubMed, Embase, and Cochrane Library search was performed on all studies between 1993 and 2011 to compare laparoscopic and open surgery for rectal cancer. The following Medical Subject Headings were used: “laparoscopy,” “rectal neoplasms/*pathology/*surgery,” “comparative study,” and “treatment outcome.” The following text words were searched as text: “total mesorectal excision (TME),” “laparoscopy,” “rectal cancer,” and “randomized controlled trial.” The “related articles” function was used to broaden the search, and all abstracts, studies, and citations scanned were reviewed. No language restrictions were made. All of the abstracts, studies, and citations scanned were reviewed. The latest date for this search was October 30, 2011.
Data extraction
Three reviewers independently extracted the following from each study: first author, year of publication, study population characteristics, study design, inclusion and exclusion criteria, number of subjects operated on with each technique, male:female ratio, conversion rate, and time of follow-up.
Inclusion criteria
To enter the analysis, studies had to include the following: (1) be an RCT comparing laparoscopic and open techniques in patients undergoing middle and low rectal cancer resection; (2) report on at least one of these outcomes—operative time, blood loss, length of resection specimen, circumferential resection margin (CRM) positivity, the proximal resection margin, the distal resection margin and the number of lymph nodes harvested in the specimen, complications, perioperative mortality, time to pass first flatus, time to resume liquid diet, time to resume normal diet, time requiring parenteral analgesia, length of hospital stay, rate of tumor recurrence, disease-free survival (DFS) rate, and overall survival (OS); and (3) clearly document rectal cancer surgery as an “TME” and clearly document technique as “laparoscopic” or “open.” When two studies were reported by the same institution, either the one of better quality or the most recent publication was included in the analysis. If necessary, we contacted the authors of the original studies to receive further information.
Exclusion criteria
Studies were excluded from the analysis if (1) the outcomes of interest were not reported for the two techniques or it was impossible to calculate these from the published results, (2) they reported on rectal surgery for benign lesions and inflammatory bowel disease and did not contain a distinct group of patients with rectal cancer, (3) they reported on emergency or urgent surgery (acutely obstructed or perforated colorectal cancer), or (4) the tumor was located in the upper rectum or rectosigmoid junction.
Assessment of methodological quality
Meta-analysis was performed in line with recommendations from the Cochrane Collaboration and the Quality of Reporting of Meta-Analyses guidelines. The quality of the RCTs was assessed using the modified scoring system of Jadad et al. 21 The assessment was based on the randomization methods, the use of intention-to-treat analysis, the report of dropout rates, allocation concealment, and the extent to which valid results were depicted. Disagreement between authors was resolved by discussion and consensus.
Statistical analysis
Statistical analysis for categorical variables was performed by using the odds ratio (OR) as the summary statistic. This ratio represents the odds of an adverse event occurring in the laparoscopic group compared with the open group. The Mantel–Haenszel method was used to combine the ORs for the outcomes of interest by using a random-effects meta-analytical technique. For continuous variables such as the number of lymph nodes harvested, statistical analysis was performed by using the weighted mean difference (WMD) as the summary statistic. If studies reported medians and ranges instead of means and standard deviations (SDs), we assumed the difference of medians to be equal to the difference of means. If no measure of dispersion was given, we tried to obtain these data from the authors or estimated the SD as the mean or median. 13 The heterogeneity for summary effects was calculated through the statistics of chi-squared and I 2 , and a value for I 2 more than 50% was regarded as representing existing heterogeneity. Random-effects models were used to identify heterogeneity between the studies, and the degree of heterogeneity was assessed using the chi-squared test. The confidence interval was established at 95%, and values of P<.05 were considered to indicate statistical significance. All statistical analyses were performed with Review Manager software version 5.1 (provided by the Cochrane Collaboration).
Results
Studies selected
Four studies22–25 published between 1990 and 2011 that matched the selection criteria and compared LTME with OTME for rectal cancer were therefore included in this meta-analysis. These included a combined total of 624 subjects, of which 308 (49.36%) underwent LTME and 316 (50.64%) underwent OTME as the primary operative intervention for rectal cancer. On review of the data extraction, there was 100% agreement among the three reviewers. Two studies was excluded because they did not clearly document rectal cancer surgery as a “TME,”16,17 and two were excluded because the tumor was located in the rectosigmoid junction and upper rectum.18,26 The selection process of the studies included is summarized in Figure 1.
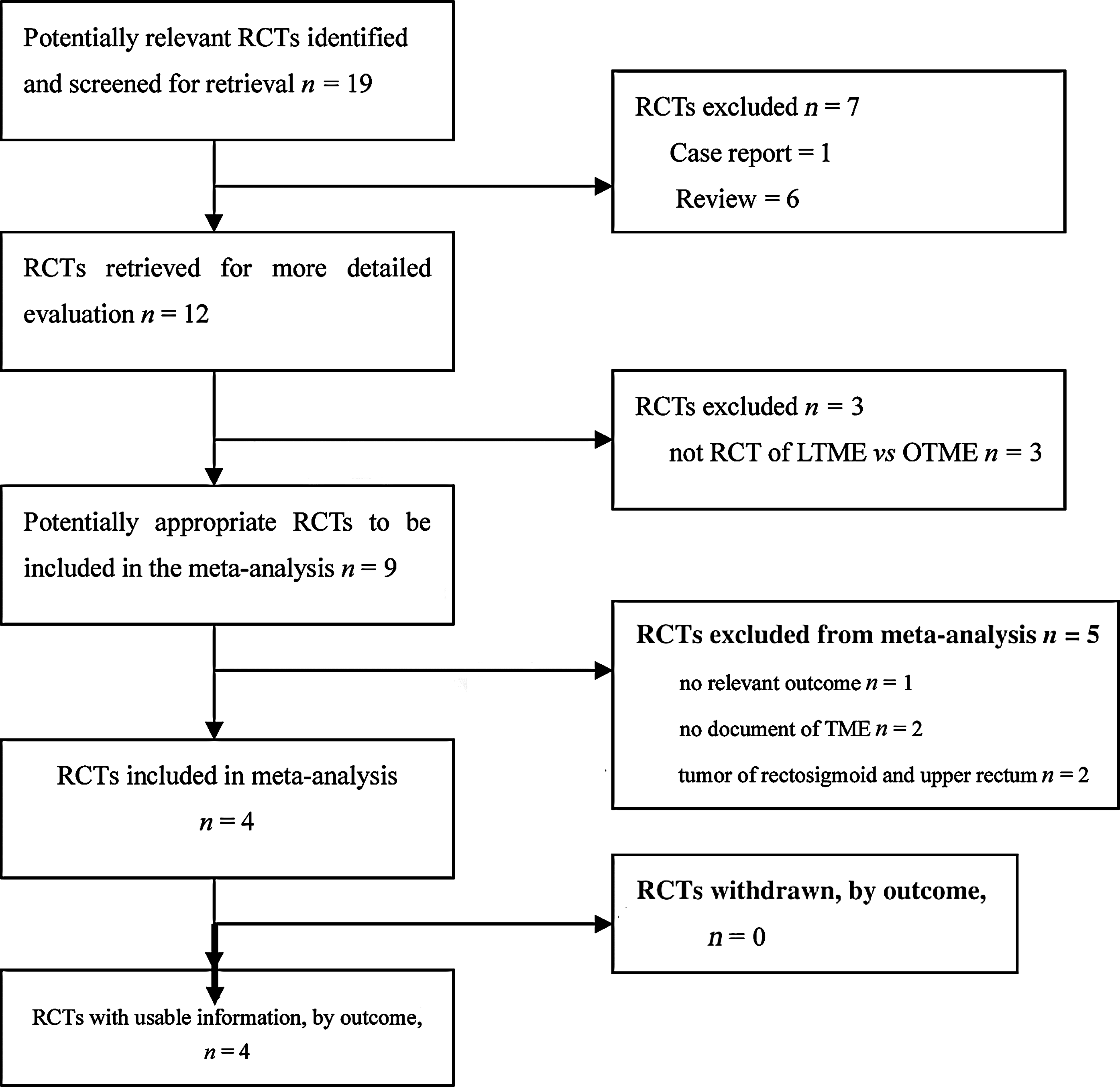
Flow diagram of this meta-analysis in accordance with the QUOROM statement. LTME, laparoscopic total mesorectal excision; OTME, open total mesorectal excision; RCTs, randomized controlled trials; TME, total mesorectal excision.
The characteristics of these four studies are listed in Table 1. The four studies contained groups that were fully matched for age and sex. Quality assessment of studies included in the meta-analysis is listed in Table 2. Two reviewers assessed all the studies that met the inclusion criteria.
LTME, laparoscopic total mesorectal excision; NR, no record; OTME, open total mesorectal excision.
ITT, intention-to-treat; ND, no record.
Operative outcomes
The operation time, intraoperative blood loss, and number of harvested lymph nodes are compared in Figure 2.
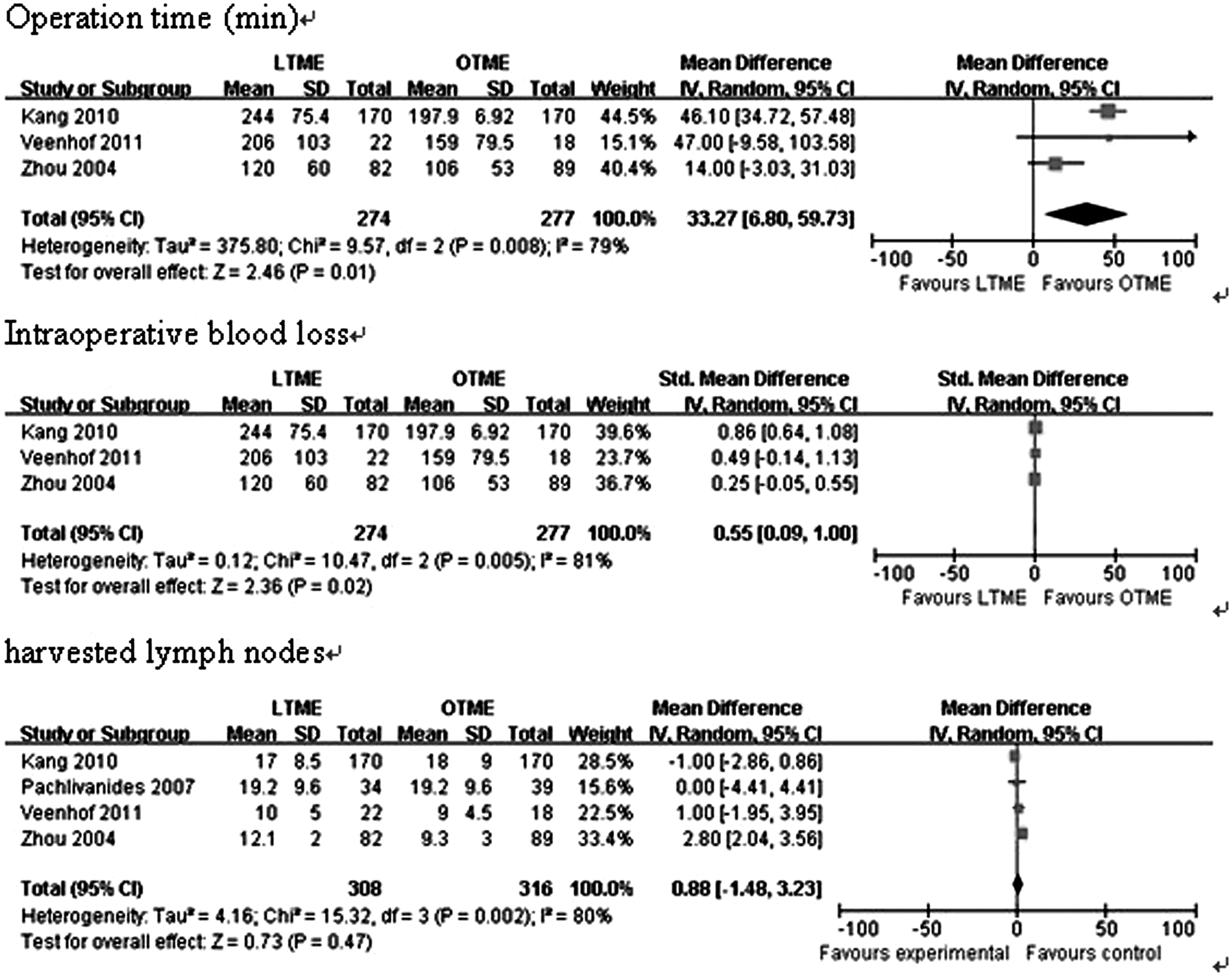
Forest plot displaying the results of the meta-analysis of measures of operative outcomes after laparoscopic total mesorectal excision (LTME) versus open total mesorectal excision (OTME) for rectal cancer: operation time, intraoperative blood loss, and harvested lymph nodes. The four studies compared here were those of Veenhof et al., 22 Kang et al., 23 Pechlivanides et al., 24 and Zhou et al. 25 CI, confidence interval; SD, standard deviation; IV, inverse variance.
Operative time was significantly increased in the laparoscopic compared with the open group (WMD 33.27 [6.80, 59.73], P=.01). There was a significant difference in intraoperative blood loss between the two groups (WMD −79.83 [−135.98, −23.69], P=.02). However, there was no significant difference between the two groups in the number of lymph nodes (WMD 0.88 [−1.48, 3.23], P=.47) (Fig. 2).
Only Veenhof et al. 22 reported length of resection specimen as median and range, and there was no difference between two groups (P=.62). Zhou et al. 25 reported the distance of the tumor from the section edge as interquartile range without mean or median. Kang et al. 23 found that the proximal, distal, and radial resection margins were similar between the two groups, as was CRM positivity. Macroscopic quality of the TME specimen was similar between the two groups. Because the data on CRM positivity and the proximal, distal, and radial resection margins were limited, meta-analysis cannot be carried out.
Perioperative complications
There was no significant difference between the LTME and OTME groups in perioperative mortality rate (OR 0.26 [0.01, 6.76], P=.42), overall morbidity (OR 0.81 [0.52, 1.26], P=.35), anastomotic leak (OR 1.41 [0.41, 4.86], P=.58), wound infections (OR 0.74 [0.16, 3.42], P=.70), pelvic abscess (OR 2.80 [0.28, 27.50], P=.38), and ileus (OR 0.76 [0.40, 1.45], P=.41) (Fig. 3). However, Zhou et al. 25 were surprised to find that morbidity was dramatically lower in the laparoscopic group compared with the control group (6.1% versus 12.4%, P<.05) in their study.
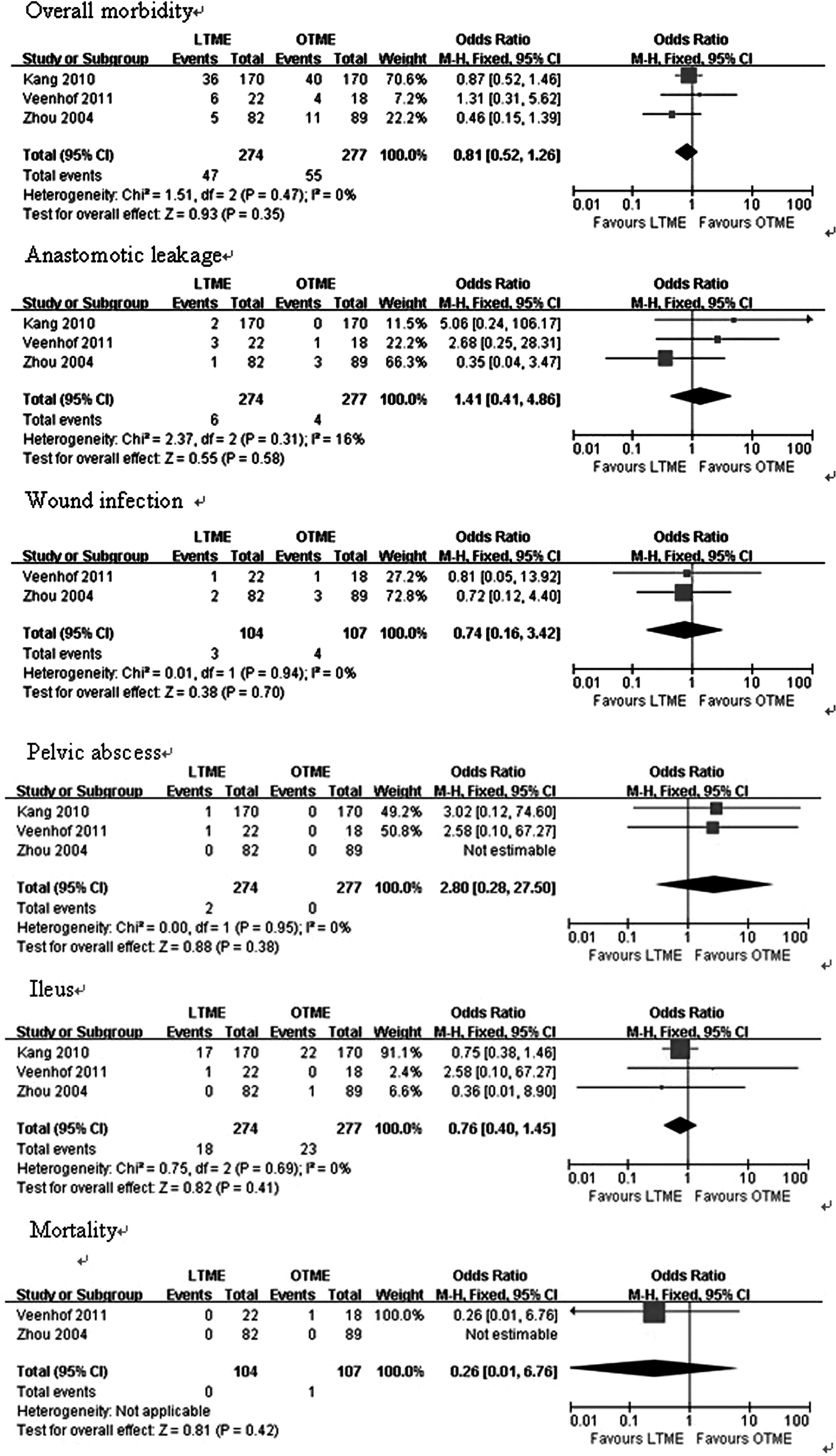
Forest plot displaying the results of the meta-analysis of measures of perioperative complications after laparoscopic total mesorectal excision (LTME) versus open total mesorectal excision (OTME) for rectal cancer: overall morbidity, anastomotic leakage, wound infection, ileus, pelvic abscess, and perioperative mortality. The three studies compared here were those of Veenhof et al., 22 Kang et al., 23 and Zhou et al. 25 CI, confidence interval; M-H, Mantel–Haenszel.
Postoperative recovery
Time to pass first flatus was significantly decreased in the LTME group compared with the OTME group (WMD −23.85 [−30.54, −17.17], P<.00001). Time to resume liquid diet (WMD −12.35 [−27.24, 2.55], P=.10), time to resume normal diet (WMD −5.94 [−12.48, 0.59], P=.07), and length of hospital stay (WMD −1.88 [−5.34, 1.59], P=.29) were shorter in the LTME group than in the OTME group; these differences, however, did not reach statistical significance (Fig. 4). Meta-analysis of pain scores and the total amount of morphine was not possible owing to the lack of uniformity of data presentation.

Forest plot displaying the results of the meta-analysis of measures of postoperative recovery after laparoscopic total mesorectal excision (LTME) versus open total mesorectal excision (OTME) for rectal cancer: time to pass first flatus, time to resume liquid diet, time to resume normal diet, and hospital stay. The three studies compared here were those of Veenhof et al., 22 Kang et al., 23 and Zhou et al. 25 CI, confidence interval; SD, standard deviation; IV, inverse variance.
Long-term outcomes
No trial reported the rate of tumor recurrence, DFS, and OS, so meta-analysis cannot be performed. Only Zhou et al. 25 reported that two port site recurrences were found in patients who underwent LTME with anal sphincter preservation, and three pelvic local recurrences were found in the open group. There was no mortality observed during follow-up, which ranged from 1 to 16 months.
Heterogeneity
The heterogeneity of the included trials was assessed. In the short-term period, significant heterogeneity was detected among studies with respect to the following six factors: number of harvested lymph nodes, operation time, intraoperative blood loss, duration of hospital stay, time to pass first flatus, and time to resume liquid diet.
Publication bias
Funnel plot analysis of the studies was performed in the meta-analysis reporting on overall postoperative complications after LTME compared with OTME. None of the studies lay outside the limits of the 95% confidence intervals, and there was no evidence of publication bias or heterogeneity among the studies (P=.47) (Fig. 5).
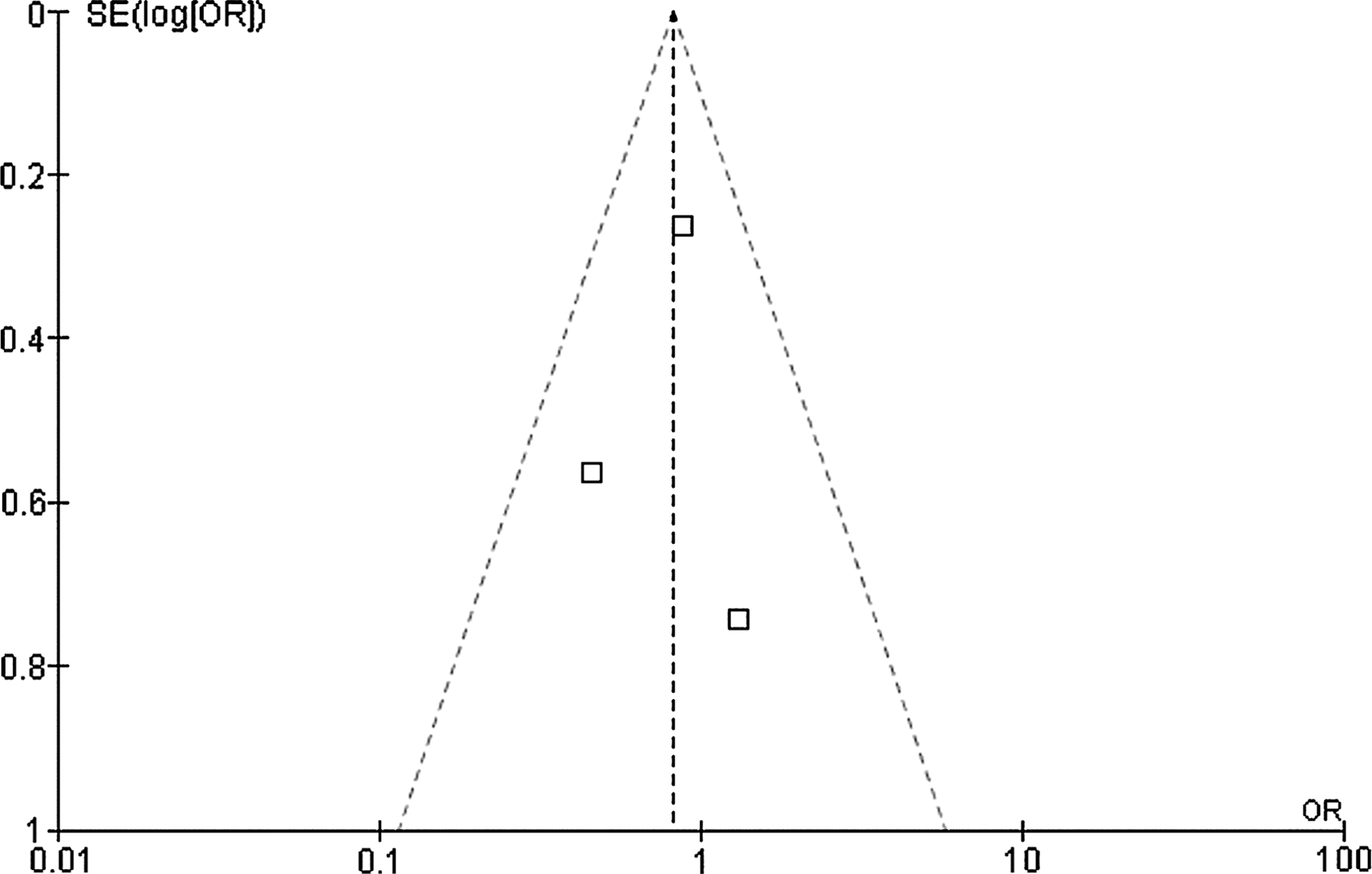
Funnel plot for the results from all studies comparing overall morbidity in patients undergoing laparoscopic total mesorectal excision versus open total mesorectal excision for rectal cancer. The four studies compared here were those of Veenhof et al., 22 Kang et al., 23 Pechlivanides et al., 24 and Zhou et al. 25 OR, odds ratio; SE, standard error.
Discussion
Since the introduction of new concept of TME, first described by Heald et al. 27 in 1982, local control and survival of rectal cancer have been improved. Currently, TME is the gold standard for treatment of middle and lower third rectal cancers.28,29 LTME for rectal cancer was first performed in 1991 and followed up by Leroy et al. 30 Thereafter, LTME was gradually applied in rectal cancer. However, application of the laparoscopic approach for the management of rectal cancer has been more limited and controversial and is still considered investigational in the United States.19,31
The aim of this study was to compare the short-term outcome between LTME and OTME for rectal cancer. Four RCTs22–25 were included; two studies were considered to be at low risk of bias. The sample sizes varied between 18 and 170, with a mean follow-up ranging from 1 to 38 months. No statistically significant differences were found between the two groups regarding the number of lymph nodes harvested, overall morbidity, and mortality.
Short-term outcome
The examination of short-term outcomes showed that LTME for rectal cancer is associated with a significantly longer operative time but significantly less intraoperative blood loss compared with conventional OTME. These results are consistent with those of comparative trials.7,32–42 The findings of this meta-analysis are in accordance with the Cochrane review in 2006 on the short-term outcomes of LTME versus OTME for rectal cancer. 43
The safety of LTME has been extensively reported in these studies,32–43 including several case series, case-matched studies, non-randomized studies, and systematic reviews.43,44 No significant difference was found for overall perioperative complications, anastomotic leakage, wound infection, pelvic abscess, ileus, and perioperative mortality between the two surgery groups. The morbidities for laparoscopic procedures were similar to those for other series.32–42 This finding suggests that the safety and feasibility of LTME are similar to those of conventional OTME.
The pooled data of the RCTs showed that time to resume liquid diet, time to resume normal diet, and hospital stay were shorter following LTME than after conventional OTME but did not reach statistical significance. It may be associated with the small number of studies included and small sample size. Aziz et al. 45 published a meta-analysis comparing operative outcomes and found no significant difference in complication rates but did find laparoscopic surgery to be associated with shorter time to feeding, first bowel movement, and hospital discharge. Ohtani et al. 46 found that there was no significant difference in the period of parenteral analgesic administration between the two groups in their meta-analysis; however, Ng et al.17,18 reported that the number of postoperative analgesic requirements was significantly lower following laparoscopic surgery than after conventional open surgery, for both upper and low rectal cancer.
Neoadjuvant therapy
In our meta-analysis, neoadjuvant therapy was carried out in three of the four trials.22–24 There is no record about neoadjuvant therapy in one trial. 25 Neoadjuvant therapy, especially neoadjuvant chemoradiotherapy, followed by TME of the rectal cancer, has been accepted as the gold standard for patients with locally advanced rectal cancer. 47 Neoadjuvant chemoradiotherapy has been shown to downstage or even downsize the tumor and to reduce local recurrence48–50 and may therefore be used together with a surgical resection as part of a multidisciplinary approach to the treatment of rectal cancer. 51
Oncological outcome
In a more recently published meta-analysis, Ohtani et al. 46 have demonstrated that the quality of laparoscopic surgery for rectal cancer appears to be similar to that of conventional open surgery, as shown by an insignificant difference in the number of dissected lymph nodes 52 and the rate of positive CRM and distal resection margin 20 in our meta-analysis and previous studies.15,17,19
Adequacy of resection margins and TME for middle and low rectal tumors are important requirements of rectal resections for cancer because they have been shown to be crucial in reducing local recurrence and ultimately improving survival during open surgery. 28 TME emphasizes the achievement of negative CRM and distal margins, thus optimizing the oncologic outcome for the patient.53,54 Involvement of the CRM is an important prognostic factor for local recurrence and distant recurrences in rectal cancer. Free CRM is one of the key aims of the TME procedure. 55 A circumferential margin of≤2 mm is associated with a local recurrence risk of 16% within 2 years of operation, whereas patients with margins>2 mm have a risk of 5.8%. 56 Breukink et al. 33 and Leung et al. 26 reported no significant difference between the two groups in terms of positive CRM.
Korolija et al. 57 reported that more lymph nodes were extracted laparoscopically (0.3–2.14 lymph nodes more), and the average distal margin clearance was 4.6 cm with the laparoscopic approach and 5.3 cm with the open approach in their meta-analysis, which shows that the laparoscopic approach is as adequate as the conventional approach. Aziz et al. 45 also found that laparoscopic rectal resections were feasible with the same proportion of positive margins and similar node retrieval found for both treatment groups. This showed that there was no difference between laparoscopic and open surgery for rectal cancer in the extent of oncological clearance. Anderson et al. 58 found that there was no difference in radial margin positivity, with 5% of patients undergoing laparoscopic surgery compared with 8% for open surgery. The incidence of distal margin positivity distal margin distance and its incidence were not significantly different between the two groups.
Five RCTs on rectal cancer16–18,59,60 reported data on the mean number of lymph nodes harvested during the surgical procedure; no significant difference was found (WMD,−0.38; 95% confidence interval, −1.35 to 0.58; P=.43),which was indicated in a recent meta-analysis. 61 However, Anderson et al. 58 found that laparoscopic surgery was associated with lower numbers of lymph nodes harvested (P=.001), but in some of the studies included patients received neoadjuvant therapy. The lymph node yield in rectal cancer specimens after neoadjuvant therapy may be reduced. 62 The nonrandomized designs of the studies included may be the reason for different numbers of lymph nodes harvested between the two groups. However, it showed that there are no oncologic differences between laparoscopic and open resections for treatment of primary rectal cancer.
An intact CRM is considered a more accurate indicator of oncological adequacy 56 than the number of lymph nodes retrieved because the latter depends mostly on the pathologist's diligence 30 and effort and neoadjuvant chemoradiotherapy.47,48 So lymph node harvest cannot be used as a good measure of the adequacy of the technique.
Long-term outcome
Because of limited and incomplete data in the studies included, pooled analysis of the long-term outcome was not applicable. Studies reporting survival outcomes for LTME have increased, but data of RCTs are limited. The Cochrane systematic review of LTME versus OTME for rectal cancer, 43 published in 2006, reported respective local recurrence rates of 7.2% and 7.7%, distant metastasis rates of 13.5% and 9.1%, and cancer-related mortality rates of 9.2% and 10%; none of these between-group differences was statistically significant.
To the best of our knowledge, only a few studies,30,37,63,64 including a case series 30 and three comparative studies,37,63,64 have reported the long-term outcome of LTME. Two comparative studies37,63 showed that there was no significant difference between LTME and OTME in local recurrence and distant recurrence, 3-year OS, 3-year DFS, and 5-year OS rate. Several meta-analyses46,58,61 also suggested that there are no differences between laparoscopic and open surgery in terms of number of lymph nodes harvested, involvement of CRM, local recurrence, 3-year OS, and DFS for rectal cancer. A published review on the long-term result of laparoscopic colorectal cancer resection from the Cochrane Collaboration concluded that long-term results from laparoscopic resection for rectal cancer are still scarce and should be obtained within the framework of RCTs. 65 Ng et al. 17 calculated that nearly 4000 patients are needed to demonstrate that long-term survival was not different between laparosopic and open surgery in a RCT. Currently, there are three ongoing multicenter RCTs—the COLOR II trial, 66 the Japanese JCOG 0404 trial, and the ACOSOG-Z6051 trial 67 ; the final data are yet to be published. The latter two are designed to compare laparoscopic versus open resection for curable rectal cancer, and their results will provide crucial information on the practice of laparoscopic rectal cancer resection. 20
So far, there is no large-sample, multicenter, prospective RCT comparing long-term outcomes of LTME with those of conventional OTME in patients with rectal carcinoma. The long-term survival benefit of LTME is still eagerly awaited by further outcomes of RCTs.
Limitation
This meta-analysis has several limitations that must be taken into account when its results are considered. First, the small number of RCTs included and the small number of cases may limit the statistical power; although there was no optimal cutoff value of number of studies, more studies are still needed. Second, outcome measures were less well defined and standardized, and this therefore limited the proportion of studies for which outcomes were comparable. Because of the lack of randomized data available, meta-analysis of some outcomes, such as CRM, distal margin, local recurrence rates, the 5-year DFS rate, and the 5-year OS rate, cannot be carried out. Third, this study could not account for the learning curve associated with the technique and its effect on postoperative outcome, and this is an important consideration because it has been suggested that laparoscopic resection of the rectum is more technically demanding and is associated with a longer learning curve than other laparoscopic colonic resections. 68 Finally, but not least, the long-term efficacy of the surgical treatment was not thoroughly discussed in the some trials included. This has impacted the comprehensiveness of the evaluation on the measured markers in our meta-analysis and decreases the robustness and comprehensiveness of its results.
All the limitations mentioned above might not allow a reliable conclusion. The design and reporting of future RCTs should consider the following suggestions: participants enrolled should undergo neoadjuvant therapy according to clinical tumor stage. More details of the trial, such as randomization, blinding, involvement of CRM, distal margin, length of specimen, and lymph node retrieval, should be described. The survival data should be presented as a hazard ratio.
In conclusion, LTME was associated with a significantly reduced rate of intraoperative blood loss and significantly reduced time to pass first flatus, at the expense of significantly longer operating time, compared with OTME. There was no significant difference between the LTME and OTME groups in the number of lymph nodes harvested, perioperative mortality rates, and overall morbidity. Furthermore, time to resume liquid diet, time to resume normal diet, and length of hospital stay, although not significantly different between the two groups, did suggest a positive trend toward LTME. Based on this meta-analysis, it showed that LTME is safe and feasible, does not jeopardize the complication rate, and does not seem to entail any oncologic disadvantages. However, significant limitations exist in the interpretation of these data because of the limited number of published RCTs, the small sample sizes, and the limited duration of follow-up. More large-sample, multicenter, prospective, randomized trials are required to determine whether LTME will play a significant role in the treatment of rectal cancer in the future. Additional RCTs that compare LTME and OTME and investigate the long-term oncological outcomes of LTME are required to determine the advantages of LTME over OTME.
Footnotes
Acknowledgments
The authors thank Dr. Huang Shifeng for reviewing this manuscript.
Disclosure Statement
No competing financial interests exist.