
Abstract
Abstract
Background:
NOTES cholecystectomy has become one of the hottest areas of research. But most of the cases need the assistance of the laparoscope. This study is conducted to evaluate the feasibility and safety of a newly proposed operative method–functional cholecystectomy by pure NOTES.
Materials and Methods:
The functional cholecystectomy was performed on eight female miniature pigs. An incision was made on the vaginal wall, and an endoscope was inserted into the peritoneal cavity to create a pneumoperitoneum to expose the intra-abdominal viscera, gallbladder, and cystic duct. The cystic duct was isolated and closed with a clip. Then, an injection needle was inserted into the gallbladder to suck up the bile. After the gallbladder was washed with saline, an incision was made on the wall of the gallbladder, and the tip of the endoscope was inserted into the gallbladder cavity. After the endoscope was withdrawn, the gallbladder incision was closed with clips in four pigs and was suspended in the other four pigs. The vaginal incision was closed with clips. All the animals were closely monitored and euthanized 28 days after the procedure. Necropsy was performed.
Results:
The functional cholecystectomy was successfully completed in all eight pigs. No severe intraoperative complications occurred. The animals recovered well postoperatively. At necropsy, no macroscopic signs of intraperitoneal infection or bile leakage in the peritoneal cavity were observed, and the clips were still present on the cystic duct in a good position in all cases. The gallbladder incision healed, with no sign of bile leakage or injury to the adjacent organs.
Conclusions:
We successfully performed the functional cholecystectomy by transvaginal approach on pigs, which appears to be feasible, safe, and convenient. Functional cholecystectomy provides a new fitting path to pure NOTES.
Introduction
At present, most surgeons prefer cholecystectomy, either open or laparoscopic, which involves ligation of the cystic artery and the bile duct and removal of the gallbladder, while others prefer cholecystolithotomy, which removes gallstones by cholangioscopy and preserves the gallbladder. However, gallstones are likely to recur in cases receiving cholecystolithotomy with gallbladder preservation. 5
With the advancement in medical science and technology, natural orifice translumenal endoscopic surgery (NOTES), a minimally invasive, painless, and scarless surgery, has emerged as a new approach in surgery.6,7 NOTES is a new surgical technique whereby “scarless” operations can be performed with a flexible endoscope passed through a natural orifice (mouth, urethra, anus, etc.) and then through an internal incision in the stomach, vagina, bladder, or colon, thus avoiding any external incisions or scars.6,8 To date, various NOTES procedures have been successfully performed on animals and humans.9–17 Specifically, many investigators have tried NOTES cholecystectomy in different ways, of which transvaginal NOTES cholecystectomy is commonly used.18–24 Because the gallbladder bed is close to the liver and the structures between Calot's triangle, cystic duct, and arteriovenous vessels are complex, it is relatively difficult to uncover and separate the gallbladder from the surrounding tissues during operation. Therefore, laparoscopic assistance is required during NOTES cholecystectomy for most cases because it is difficult to complete the operation by a single flexible endoscope, whether it is through single or double pipelines. Thus, NOTES cholecystectomy assisted with laparoscopy is actually a hybrid operation (i.e., a combined use of an endoscope and a laparoscope) rather than a pure NOTES (i.e., use of a flexible endoscope only), which undermines the advantages of NOTES over laparoscopy.25,26
In order to treat gallstones with pure NOTES, we developed an innovative technique, dubbed as a “functional cholecystectomy.” This operation only needs to use the endoscopic clip to ligate the cystic duct. Then, an injection needle is inserted into the gallbladder to suck up the bile. Finally, an incision is made on the wall of the gallbladder to remove the gallstones. The gallbladder is preserved, but the cholelithiasis can be cured. The gallstone recurrence will never occur because the bile, a major ingredient of the gallstone, no longer exists in the gallbladder. 27 The entire operation can be performed with a flexible single-pipeline endoscope by pure NOTES.
Materials and Methods
Animals, equipment, and medications
Eight female miniature pigs weighing 15–25 kg and 5–6 months old were used in this study. The pigs were housed at the animal research facility at the 2nd Affiliated Hospital of Harbin Medical University (Harbin, China). The research approach was approved by the Animal Care and Use Committee of the 2nd Affiliated Hospital of Harbin Medical University.
An Olympus (Tokyo, Japan) gastroscope (model GIFQ260) and an electrosurgical generator (Endocut ICC200; Erbe, Tübingen, Germany) with a blended current of 50–70 W cutting cautery were used. Other equipment included an isolated tip knife (model KD-610L; Olympus), a hook-type knife (model KD-620LR; Olympus), an injection needle (model 19G; Olympus), a Coagrasper™ (Olympus), hemostatic clips and a release device (Olympus), a polyloop and release device (Olympus), a transparent plastic-fitted cap, and homemade outer thimbles. All endoscopes and accessories were sterilized prior to use.
Medications used in the study included diazepam, ketamine hydrochloride for injection, 2% pentobarbital sodium, atropine, cimetidine, ciprofloxacin hydrochloride, and penicillin sodium (Harbin Pharmaceutical Group Co., Harbin).
Anesthesia and procedures of functional cholecystectomy by NOTES
The pigs were deprived of food and water for 12 hours before the experiment. Premedication consisted of intramuscular injection of ketamine (100 mg) and diazepam (10 mg). General anesthesia was induced with intravenous 2% pentobarbital sodium (2 mL/kg).
The animals under general anesthesia were placed in a supine position on the operation table. The vulva and vagina were disinfected routinely with iodophor. An incision was made on the vaginal wall with a hook-type knife, about 15 cm away from the vulva, and enlarged to about 20 mm with the hook-type knife and an isolated tip knife. The endoscope was then inserted into the peritoneal cavity to create a pneumoperitoneum with room air insufflation to expose the intra-abdominal viscera and find the gallbladder and cystic duct (Fig. 1).
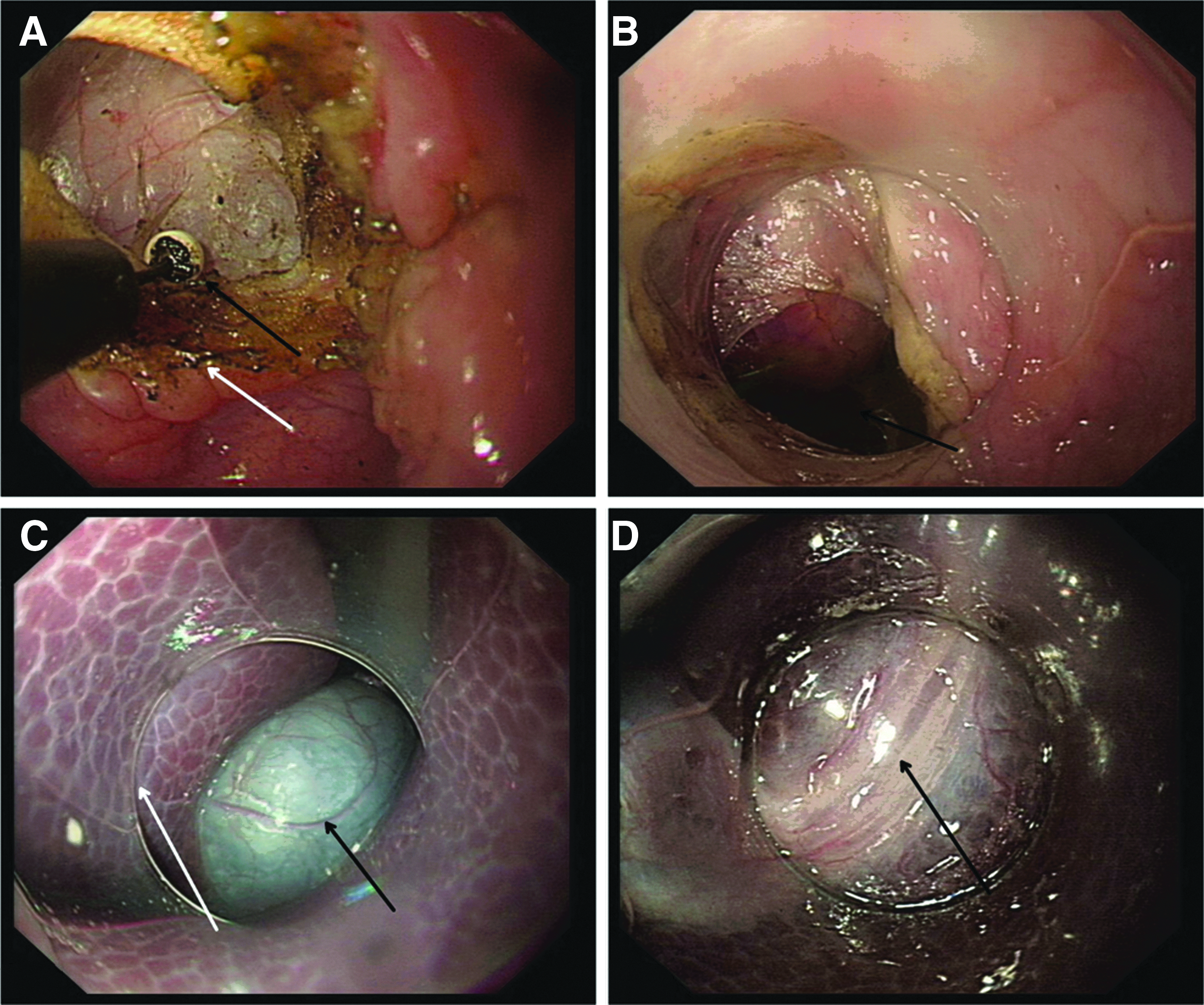
Endoscopic views of the initial procedures in pigs of functional natural orifice translumenal endoscopic surgery (NOTES) cholecystectomy:
The cystic duct was exposed, isolated, incised for about 2 cm near the gallbladder with the hook-type knife and the isolated tip knife, and occluded with clips (Fig. 2A–C). An injection needle was inserted through the endoscope, sent into the bottom of the gallbladder to suck up the bile from it, and then withdrawn after repeated washes of the gallbladder with normal saline. The gallbladder wall was then incised for about 2 cm at the bottom center along the vertical axis with the hook-type knife and the isolated tip knife, through which the endoscope was sent into the gallbladder to inspect the mucosa of the gallbladder and the debouch of the cystic duct (Fig. 2D and E). After the endoscope was withdrawn from the gallbladder, the gallbladder incision was closed by clips in four pigs (Fig. 2F) and suspended in the other four pigs. The vaginal incision was closed by clips.
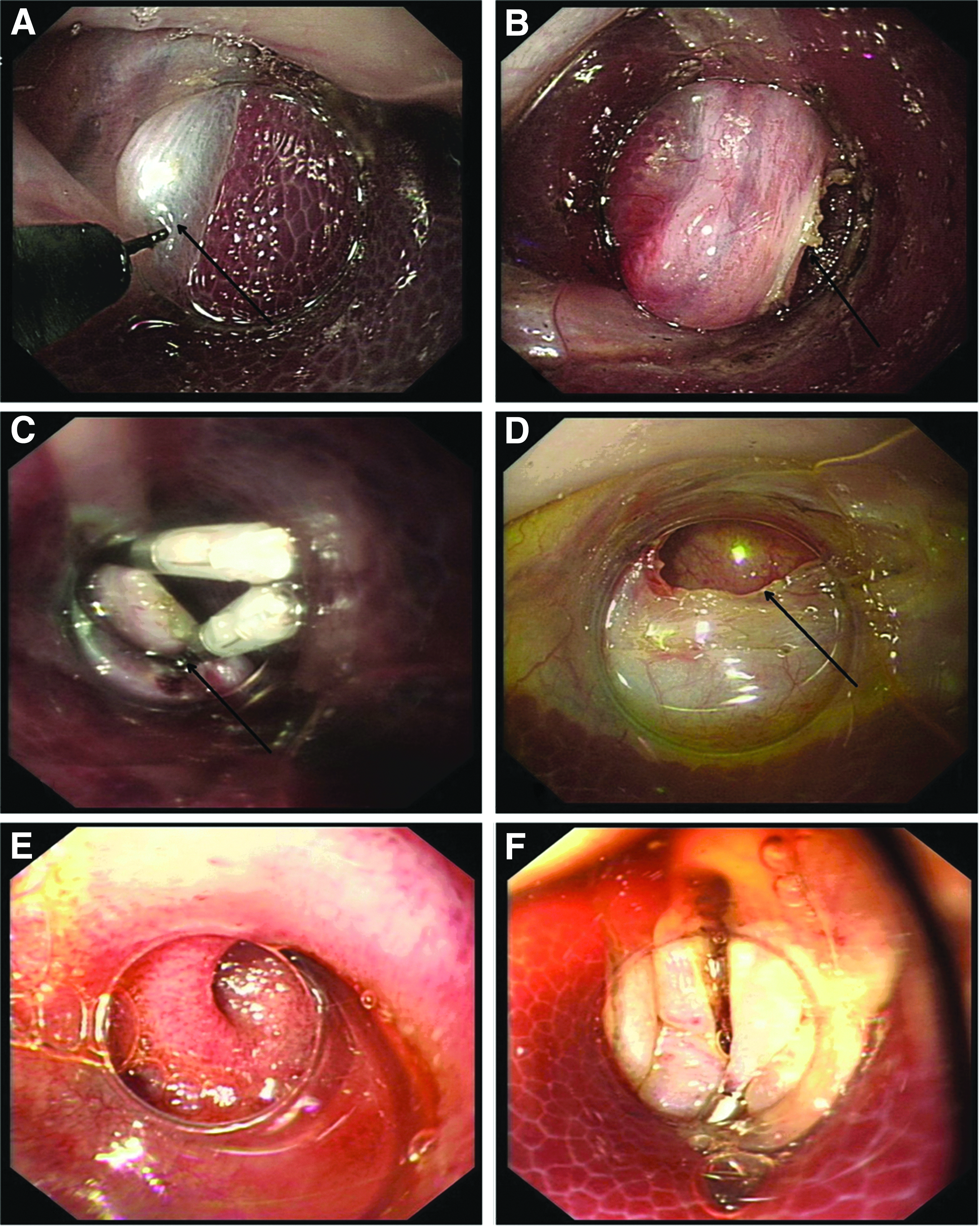
Endoscopic views of the major procedures in pigs of functional natural orifice translumenal endoscopic surgery (NOTES) cholecystectomy:
Postoperative follow-up
All pigs were given a regular diet immediately after recovery from general anesthesia (about 4–6 hours after the procedure). All animals received antibiotic prophylaxis with intramuscular injection of penicillin, 800,000 units twice a day for 3 days. The animals were extensively monitored on a daily basis for signs of peritonitis or other adverse events and postoperative complications by an experienced biotechnician. All pigs were sacrificed with intravenous pentobarbital sodium (100 mg/kg) 28 days after the operation; then a necropsy was performed, and the cystic duct and gallbladder were observed.
Results
Functional cholecystectomy was successfully completed via the vagina in all eight pigs. No intraoperative events and postoperative complications occurred. All animals were fed separately and recovered well postoperatively. All pigs survived in a good general condition and with appropriate weight gain. No jaundice developed in any animal. Thus, there was no difference in all observed parameters between the pigs with the closed gallbladder incision and those with the suspended incision.
All eight pigs were euthanized 28 days after surgery to examine the peritoneal cavity, with particular attention paid to the site of the cystic duct, the clips, the gallbladder, and the presence or absence of adhesion of the gallbladder. At necropsy, no macroscopic signs of intraperitoneal infection or bile leakage in the peritoneal cavity were observed in any animal. The clips were still present on the cystic duct in a good position in all cases. The gallbladder incision healed well in the animals using the clips and started healing in the animals with the suspended gallbladder, with no sign of bile leak or injury to the adjacent organs (Fig. 3).
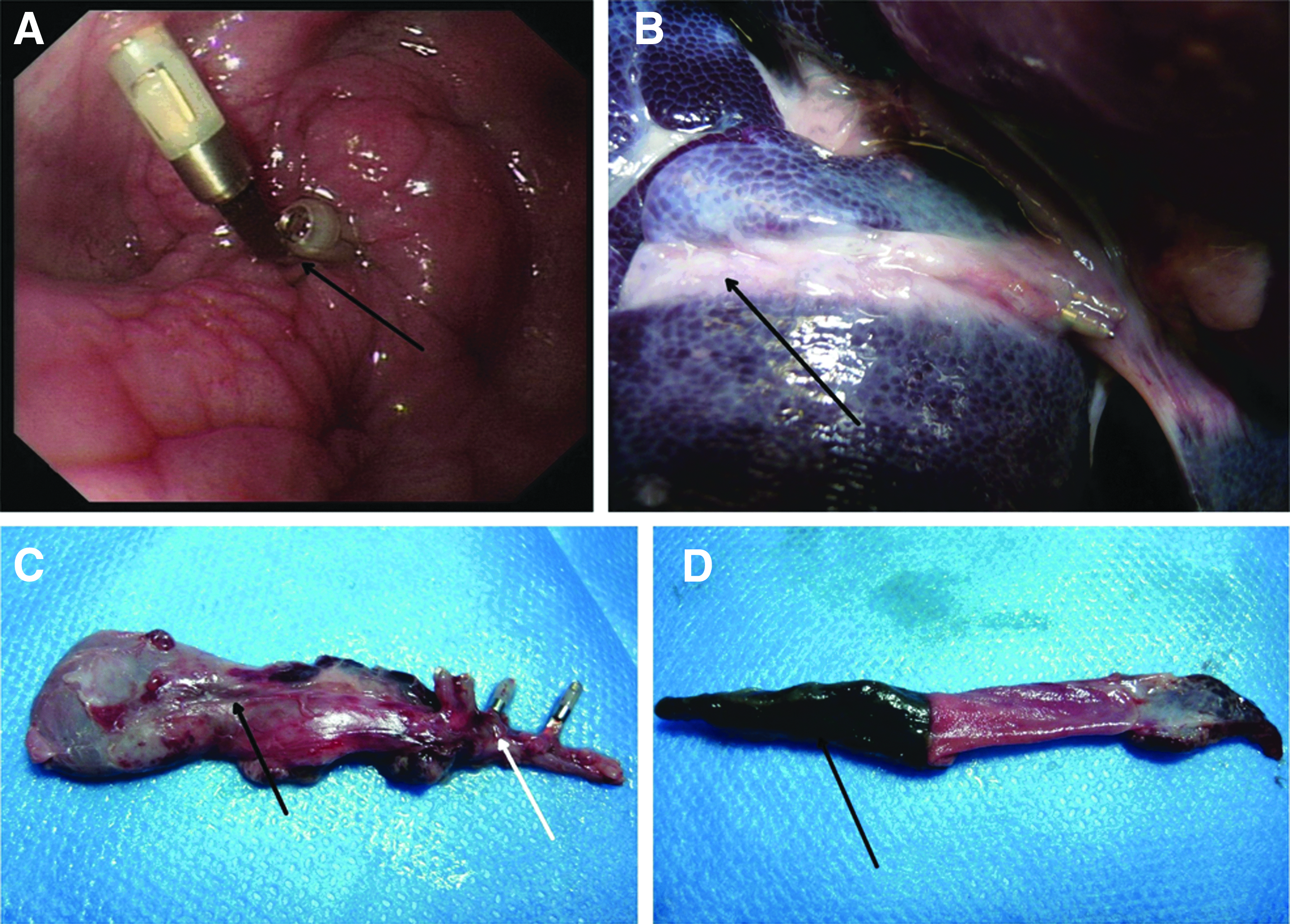
Macroscopic views of the gallbladder and cystic duct in pigs 28 days after functional natural orifice translumenal endoscopic surgery (NOTES) cholecystectomy:
Discussion
Currently, transvaginal and transgastric routes are the major approaches into the abdominal cavity in NOTES cholecystectomy, with transvaginal cholecystectomy being more commonly used because it does not affect food intake after the surgery. However, the gallbladder is difficult to separate from the surrounding tissues during transvaginal cholecystectomy in some cases, and thus laparoscopy is usually used. To simplify the operation, we proposed a novel technique, which we call functional cholecystectomy. In the study, we successfully completed the operation in all eight pigs with only a single-pipeline endoscope. There were no serious adverse events, postoperative complications, or death.
The greatest advantage of “functional cholecystectomy” is that it is not necessary to remove the gallbladder; instead, we preserved the gallbladder but made it lose its bile storage and condensation functions by clipping the cystic duct, which made the procedure simpler.
The detailed compilation of the conventional cholecystectomy, cholecystolithotomy, laparoscopic-assisted NOTES cholecystectomy, and functional cholecystectomy by pure NOTES is listed in Table 1. We believe that the surgical procedures for “functional cholecystectomy” are useful, necessary, and feasible in the treatment of cholelithiasis. First, removal of the pathogenic organ is usually considered as only a means rather than an objective of treatment. In patients with cholelithiasis, the ultimate objective that needs to be achieved is removal of the bile in the gallbladder, not the gallbladder per se. Second, conventional cholecystectomy cannot be successful in some patients with complex or irregular anatomical structures, and subtotal cholecystectomy or partial cholecystectomy has to be performed, In these cases, while the bile in the residual gallbladder remains a risk factor for the recurrence of the gallstone, the residual gallbladder does not seem to have caused big problems. 28 Thus, it is conceivable that the suspended gallbladder is unlikely to do any harm, although long-term animal and clinical studies are required to confirm this notion.
NOTES, natural orifice translumenal endoscopic surgery.
Theoretically, the functional cholecystectomy by NOTES is not only simpler and quicker, but also safer than laparoscopy-assisted NOTES cholecystectomy simply because it does not require laparoscopy and the removal of the gallbladder. It should be mentioned that since there was no need to separate the gallbladder artery and remove the gallbladder, the risks of serious complications such as massive hemorrhage are expected to be significantly reduced. Indeed, in the present study, we completed the functional transvaginal cholecystectomy in all eight pigs without any intraoperative events, postoperative complications, and death during the close follow-up interval of 28 days. We attempted to determine if there was any difference between the pigs with the gallbladder incision closed and those with the incision suspended, but failed to observe any. However, further investigation with a large sample size and especially those in humans are required for confirm the preliminary observation.
There are some concerns or limitations for the functional cholecystectomy by NOTES. The first concern is the potential for carcinogenesis of the residual gallbladder. However, carcinoma of the gallbladder is a relatively rare malignancy. 29 The incidence of gallbladder cancer varies with races and environments; the highest incidence rate worldwide is among Indian women (21.5 per 100,000), whereas the rate is very low in whites in Western Europe and the United States (1 per 100,000).30–32 According to previous findings, the pathogeneses or contributing factors mainly include gallstones and abnormal connections between pancreatobiliary ducts. 33 We therefore believe that the functional cholecystectomy would not increase the risk of carcinogenesis; rather, it may decrease the risk because it removes one of the risk factors of gallbladder cancer—the gallstone. The second concern is related to the secretion of the gallbladder mucosa that may cause hydrocholecystis. The gallbladder mucosa secretes about 20 mL of mucus daily to protect it from erosion of the bile. However, the absorption capacity of the gallbladder is by far greater than its secretion capacity. Our experiment demonstrated that there was no fluid in the gallbladder 28 days after surgery, except for a small amount of mucin-like substances. In addition, pathological examination did not show any inflammatory or precancerous change in the mucosa. We thus deduce that functional cholecystectomy would not cause hydrocholecystis or hydrops of the gallbladder in the long run, although further investigation is needed to confirm our observation in animals. If long-term experiments demonstrate the existence of hydrocholecystis, we could further treat the gallbladder mucosa using alcohol or phenol to ablate the mucosa, as previously described.34–36 Currently, we are planning to carry out a further study in this aspect.
In conclusion, we successfully performed a newly proposed functional cholecystectomy by pure NOTES in pigs, which appears to be feasible and safe. Further investigation of this technique with long-term follow-up in animals and humans should be conducted to confirm the preliminary observation and determine the therapeutic and prophylactic efficacy.
Footnotes
Acknowledgments
This work was supported by grant ZD2008-09 from The Science Foundation of The Second Affiliated Hospital of Harbin Medical University.
Disclosure Statement
No competing financial interests exist.