
Abstract
Abstract
Background:
Acute small bowel obstruction (SBO) is a common cause of emergency hospital admission, often requiring surgical intervention. Herein, we describe the single-incision laparoscopic surgery (SILS) procedure for the management of SBO in the acute care setting.
Patients and Methods:
Patients with intestinal obstruction who underwent SILS in Chang Gung Memorial Hospital, Linkou, Taiwan, from January 2010 to January 2012 were retrospectively analyzed. Informed consent was obtained from all patients. Demographic information, intraoperative findings, surgery duration, and conversion to multi-incision laparoscopic surgery (MILS) were recorded. Postoperative records included the recovery period after surgery, complications, length of hospital stay, and final prognosis.
Results:
Ten SILS procedures for the repair of SBO were performed (six women, four men; median age, 52 years [range, 28–89 years]). Only 1 patient (10%) required conversion to MILS. The median operative time was 140 minutes (range, 90–210 minutes), median time to resume oral intake was 3 days (range, 1–7 days), median time to ambulation was 3 days (range, 1–6 days), and median postoperative hospital stay was 7.5 days (range, 3–14 days). There was no mortality in this series. All patients were discharged uneventfully. The umbilical incision was nearly invisible at the 1-month follow-up. The median follow-up time was 13.5 months (range, 4–26 months). No incisional hernias or adhesions were observed.
Conclusions:
SILS for SBO is a feasible, safe procedure that can be performed as initial treatment in select patients with bowel obstruction through resection and decompression of the small bowel using intra- or extracorporeal techniques, resulting in a nearly invisible scar.
Introduction
Single-incision laparoscopic surgery (SILS) has become popular in recent years as a minimally invasive approach in several procedures, including cholecystectomy, colectomy, hysterectomy, and bariatric surgery.8–11 Moreover, SILS is commonly performed in emergency operations such as acute appendicitis and cholecystitis.12,13 SILS is associated with reduced postoperative pain, faster recovery, and an improved cosmetic effect compared with multi-incision laparoscopic surgery (MILS).8–10,13 In the present study, we have reviewed a series of single-incision laparoscopic-assisted surgery for release of SBO (SILS-SBO) and discussed the efficacy of this minimally invasive surgery.
Patients and Materials
Ten consecutive patients who underwent SILS-SBO at Linkou Chang Gung Memorial Hospital, Taoyuang, Taiwan, between January 2010 and January 2012 were retrospectively analyzed. Informed consent was obtained from all patients before surgery. Demographic information was collected and recorded together with the results of biochemical and radiographic analyses. In addition, intraoperative findings, operative time, and conversion to MILS were recorded. Postoperative data obtained from clinical records included the time required to resume oral intake, time to ambulation, length of hospital stay, and final prognosis.
Surgical technique
Patients were placed in a lithotomy position under general anesthesia. A subumbilical 2-cm vertical incision was made, and the peritoneum was entered under direct vision, by inserting one finger into the peritoneal cavity to prevent retraction of the viscera or omentum. An Alexis wound retractor (S size; Applied Medical) was inserted to make the incision as wide as possible, and then a homemade glove-port was placed. Two 5-mm trocars and one 12-mm trocar for 10-mm rigid scopes were placed, and, if necessary, an additional 12-mm trocar was introduced to replace one of the 5-mm trocars for instrument insertion (Fig. 1). Under a pneumoperitoneum of 12 mm Hg, the operator performed an intracorporeal procedure using an endoscopic dissector, a nontraumatic grasp, scissors, and electrocauterizer. Adhesiolysis was performed by means of a sharp and a blunt dissection (Fig. 2). The anterior abdominal wall was completely cleared to enable the identification of the cecum and terminal ileum. The small bowel was “run” with atraumatic tissue graspers in a retrograde manner, lysing any adhesions encountered during this process until the point of obstruction was identified and marked. The bowel was then followed to the ligament of Treitz to ensure that no other obstruction was present. Any lesions encountered such as adhesion bands or internal hernias were lysed and reduced intracorporeally. In patients with necrotic bowel, diverticulitis, or neoplasms, resection and anastomosis of the intestine were first attempted intracorporeally. However, if there was massive bowel distension or if the tissue was too fragile, resection and anastomosis were not feasible intracorporeally, and the umbilical incision was extended to 3 cm. The operative port was then dilated to a diameter of 5 cm using the wound retractor. Bowel resection or the release of the obstruction was performed using an abdominal lifting system (Fig. 3) with laparoscopic and conventional open instruments (Fig. 4). Retrograde decompression of the bowel was routinely performed either intra- or extracorporeally. After completion of these procedures, the pneumoperitoneum was reestablished to examine the peritoneal cavity for possible bowel ischemia, serosal injury, or undecompressed dilation.

Homemade glove-port for single-incision laparoscopic-assisted surgery for the release of small bowel obstruction.

Identification and lysis of adhesion band are performed by means of a sharp and a blunt dissection.
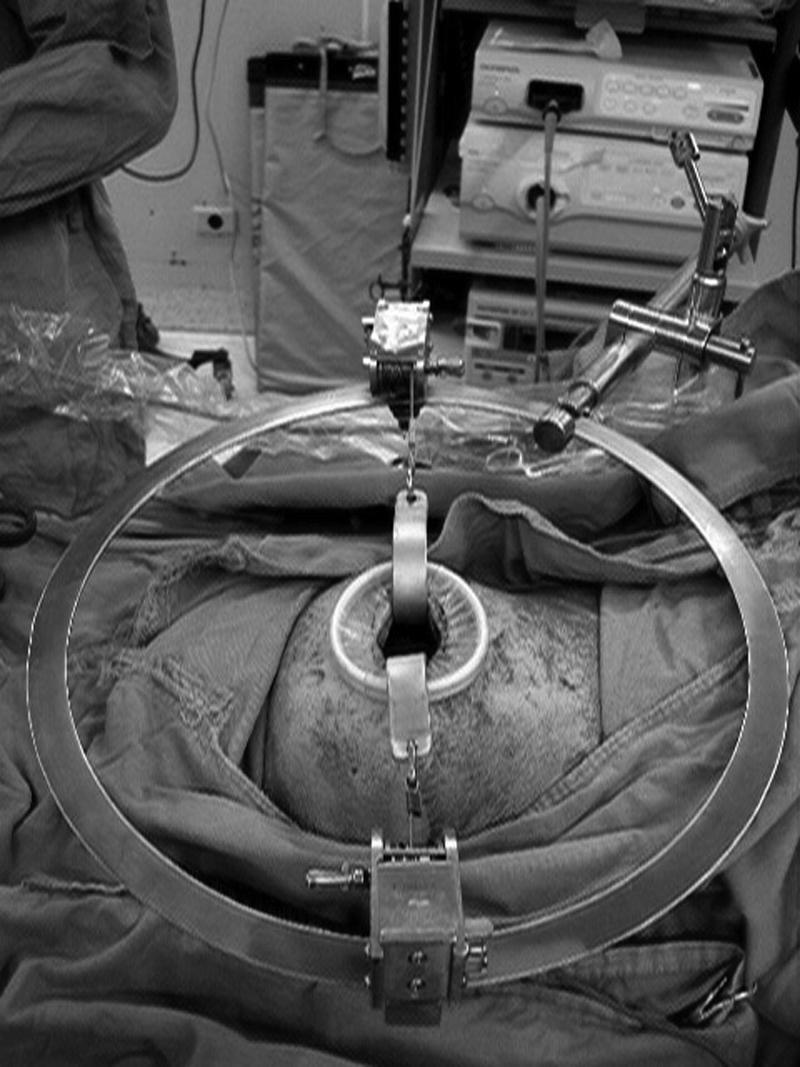
Abdominal lifting system and special-designed abdominal traction hook whose width is 2.5 cm are applied to perform the single-incision laparoscopic surgery-assisted procedure.

Extracorporeal manipulation of the small bowel with large laparoscopic and conventional open instruments.
Results
Ten patients (six women and four men) with a median age of 52 years (range, 28–89 years) underwent transumbilical SILS-SBO. Of these 10 patients, 4 had simple adhesion bands, 2 had intraluminal tumors, 2 showed external compression caused by a diverticular abscess, 1 patient had a bezoar, and 1 presented with ischemic stenosis of the jejunum due to past mesenteric trauma. The median operative time was 140 minutes (range, 90–210 minutes) (Table 1).
ASA, American Society of Anesthesiologists physical status classification; F, female; M, male; MILS, multi-incision laparoscopic surgery.
In addition to adhesiolysis and decompression, 5 patients underwent bowel resection and anastomosis, and 1 patient required enterotomy for bezoar removal. Conversion to MILS was necessary in 1 patient (Case 5) who had adhesions with bowel necrosis and required the introduction of an additional trocar port to obtain better surgical vision for traction. One patient (Case 7) experienced sigmoid diverticulitis rupture with abscess formation. After resection of the perforated colon, a 2-cm incision was made in the left lower quadrant abdomen for end-colostomy formation. Conversion to open laparotomy was not required in any of the patients. The median time to resume oral intake was 3 days (range, 1–7 days). The median time to ambulation was 3 days (range, 1–6 days), and the median hospital stay was 7.5 days (range, 3–14 days) (Table 2). There were no pulmonary or wound infections, postoperative intra-abdominal abscess formations, or mortalities in this series. The median follow-up time was 13.5 months (range, 4–26 months). No incisional hernias or adhesions were observed. One patient presented to the emergency department within 30 days after surgery with acute enterocolitis (Case 2). The umbilical incision was nearly invisible at the 1-month follow-up visit.
HLOS, hospital length of stay.
Discussion
In recent years, SILS has emerged as a safe and effective minimally invasive approach for the correction of several abdominal emergencies. Studies have shown that SILS is associated with reduced postoperative pain, an acceptable incision, a short hospital stay, and quick recovery.7–9,12 However, to our knowledge, reports on SILS-SBO in the literature are limited, 14 suggesting that the safety and feasibility of SILS-SBO require evaluation. In this preliminary study, we described 10 consecutive patients who underwent SILS-SBO with acceptable results.
Evidence of the safety of a new technology needs to be provided before its implementation in routine clinical practice. The present results indicated that SILS-SBO is a safe and feasible procedure. There were no intraoperative complications such as bowel injury or uncontrollable bleeding associated with the procedure, and none of the patients required additional surgery. There was no mortality among the patients included in the study. The median time to resume oral intake was 3 days, and none of the patients had prolonged ileus after the operation. Although a prolonged hospital stay was prevalent in our series (median, 7.5 days; range, 3–14 days), the median time to ambulation was 3 days (range, 1–6 days). The early oral intake resuming and ambulation noted in our patients indicated SILS-SBO allows early recovery. The prolonged hospitalization could be related to patient expectations and the low hospital fees in our country. The median follow-up time was 13.5 months (range, 4–26 months). No incisional hernias or recurrent obstructions were observed in the present group, although the follow-up period was too short to exclude the possibility of these complications completely.
The most common etiology of SBO was postoperative adhesions, which in 49%–73% of the cases were simple or single fibrous adhesions that could be resolved by laparoscopic surgery.1–3,7,15,16 These adhesions could be identified and lysed using SILS-SBO. In most of the patients included in our study (80%), adhesiolysis and decompression were performed using SILS-SBO. Because postoperative adhesions are one of the most common causes of bowel obstruction, the advantages of SILS-SBO are obvious. Several studies have reported that decreasing the size and number of incisions results in a lower incidence of adhesions and incisional hernias.17,18 Compared with MILS, SILS-SBO is associated with fewer incisions and limited parietal trauma; therefore, the SILS-SBO procedure should theoretically decrease postoperative adhesion formation. Furthermore, in agreement with the findings of previous studies, the postoperative pain reported by our patients was lower than that reported by patients who underwent MILS.7,8
After postoperative adhesions, the most common etiologies of SBO are neoplasm and diverticulum.1,3,7 In the present study, SILS-SBO enabled the resection of the bowel and its recovery through a transumbilical incision with limited extension of the wound. The use of a wound retractor prevented the development of infections, and none of the patients in our series had an infected wound. A decrease in the incidence of wound infection associated with SILS has been reported previously.12,13 Another advantage of SILS-SBO is the improvement in the cosmetic results associated with the reduced number of trocars. In most of our patients, the wound was not visible after surgery, and even in patients requiring extension of the incision the final scar was acceptable.
One of the disadvantages of laparoscopic release of SBO is the difficulty in decompressing the bowel content. In patients with insufficient decompression, laparoscopic surgery is often contraindicated.2,15,16 Another complication of laparoscopic surgery for SBO is related to the use of instruments for handling the bowel. If the bowel is distended and edematous, it is prone to perforation by small laparoscopic instruments. In a study by O'Connor and Winter, 1 the common reasons for the conversion to laparotomy were poor decompression and incidental injury to the bowel. However, SILS-SBO overcomes these disadvantages. The umbilicus provides a natural orifice to enter the peritoneal cavity with a limited scar. The use of a wound retractor enables the extension of the 2-cm umbilical incision to a 3-cm opening, which permits the decompression of the dilated small bowel. In cases showing a distended and fragile bowel, enterolysis and decompression with small laparoscopic instruments are hard to perform. We extended the umbilical incision to 3 cm and dilated it to 5 cm using a wound retractor as a mini-laparotomy. Then, an abdominal lifting system was used to generate ample space to manipulate the small bowel with larger laparoscopic instruments or conventional open instruments. This modified SILS-assisted procedure allows the inspection and manipulation of the bowel and mesenterium intracorporeally and extracorporeally with improved safety. To date, no bowel injury has been reported in association with this modified SILS-assisted procedure. After enterolysis and decompression, the pneumoperitoneum is reestablished with the glove method, sealing the transumbilical port to examine for the presence of ischemia, injury, or insufficient decompression of the bowel. A combination of laparoscopic observation and direct inspection through the incision during SILS-SBO increases the diagnostic capacity and reduces the complication rate.
Proper selection of patients is important to increase the success rate. Patients with simple adhesion bands, bezoars, tumors, or diverticula smaller than 5 cm may be suitable for SILS-SBO. The contraindications of SILS-SBO, which are similar to those of laparoscopic surgery for SBO, include hemodynamic instability, inability to tolerate pneumoperitoneum, the presence of extensive intra-abdominal soiling, or dense adhesions.1,2,5 Although our results confirmed the safety and feasibility of SILS-SBO, there are several problems associated with the procedure that need to be addressed. Prolonged operative times were noted in this series, with a median of 140 minutes (range, 90–210 minutes), and it increased the cost of surgery compared with that of open laparotomy and MILS. There is a learning curve associated with SILS-SBO, as it is a relatively new technique for most surgeons. The suboptimal viewing angles, crowded instruments, and loss of triangulation may have also contributed to the prolonged operative time. Increased experience will certainly lead to shorter operative times in our series (Fig. 5). Previous studies have shown that there is a learning curve associated with the performance of SILS. 19 Increased experience and technical developments in the instrumentation for SILS-SBO will enable surgeons to become more skilled and therefore shorten the operative times. Although the umbilicus is the ideal site as a portal of entry, its use limits the number of candidates who are appropriate for this type of surgery. If the obstruction is caused by a diverticulum or neoplasm larger than 5 cm, the retrieval of the specimen is difficult without extending the incision to more than 3 cm, which has been associated with an increased complication rate, thus compromising the benefits of this procedure.8,20,21 For patients with past laparotomy incision, including umbilicus, another 2-cm incision away from the umbilicus is necessary. It decreases the cosmetic benefit of SILS-SBO and adds the possibility of adhesion.
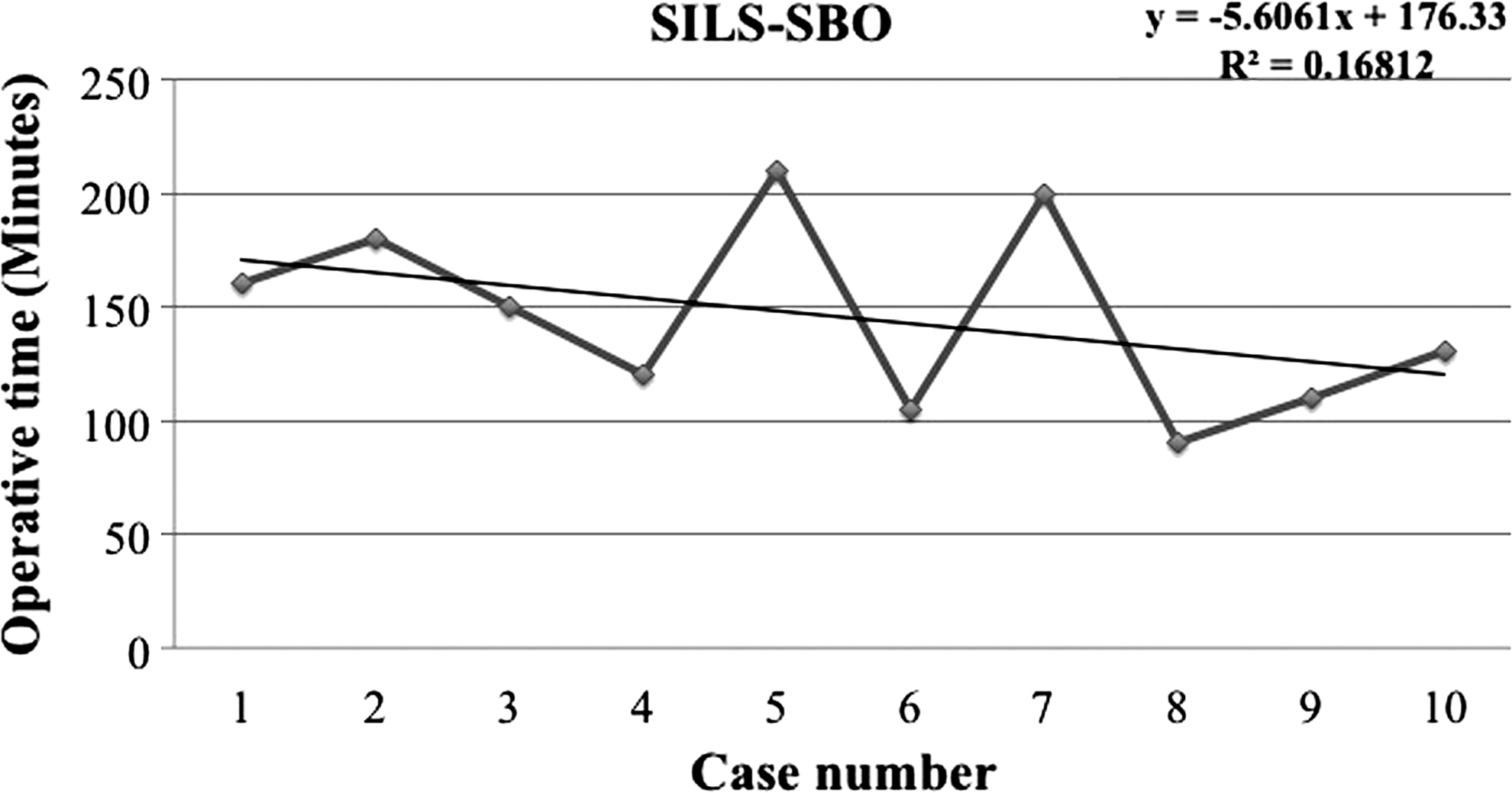
Linear regression analysis of operative times over the course of our experience. SILS-SBO, single-incision laparoscopic-assisted surgery for the release of small bowel obstruction.
In conclusion, SILS-SBO is a feasible and safe procedure that can be performed in a select group of patients with bowel obstruction as initial surgery. Transumbilical SILS-SBO enables the resection and decompression of the small bowel intra- and extracorporeally with a nearly invisible scar. Several procedures can be performed using SILS-SBO with all the expected benefits of this minimally invasive procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.