
Abstract
Abstract
Complete (R0) resection and extent of lymphadenectomy are important prognostic factors for survival in patients undergoing surgery for esophageal carcinoma. We describe the first case of combined open and thoracoscopic esophagectomy with extended lymphadenectomy including abdominal, cervical, right, and left mediastinal (four-field, four-phase) nodal clearance in a 37-year-old woman with squamous cell carcinoma of the esophagus. This report provides a tailored strategy to achieve a high level of tumor clearance and complete resection. The approach described challenges the limitations of standard radical nodal clearance and may encourage surgeons to consider more extensive resections.
Introduction
In this report, we describe the first case of a combined open and thoracoscopic four-phase approach to esophagectomy with extended four-field lymphadenectomy including abdominal, cervical, mediastinal, and left paravertebral clearance to achieve R0 resection in a patient with squamous cell carcinoma of the esophagus.
Case Report and Methods
A 37-year-old woman, otherwise fit and well, presented with a short history of dysphagia and weight loss while breastfeeding her third child. Endoscopy revealed an area of squamous dysplasia from 27 to 30 cm and a squamous carcinoma from 30 to 36 cm.
Staging investigations
Computed tomography (CT) scanning revealed thickening of the lower esophagus but no enlarged lymph nodes or distant metastases. Endoscopic ultrasound staged the tumor as T3, N1. Positron emission tomography (PET)-CT (Fig. 1) showed the [18F]fluoro-2-deoxy-

Positron emission tomography scan in a patient with esophageal squamous cell carcinoma. [18F]Fluoro-2-deoxy-
Ultrasound-guided fine-needle aspiration of the right retrothyroid neck node confirmed the presence of metastatic squamous cell carcinoma, giving the initial staging as cT3 N1 pM1b. Multidisciplinary team discussion considered the tumor to be metastatic with no curative option. The patient was managed with palliative chemotherapy, receiving four cycles of epirubicin, oxaliplatin, and capecitabine followed by maintenance oral capecitabine.
The outcome was a good clinical response that rendered the patient asymptomatic. There was metabolic resolution on PET-CT and significant endoscopic regression up to 18 months following diagnosis. At 20 months, however, the patient developed recurrent dysphagia, and endoscopy confirmed local disease progression. Restaging by FDG PET-CT showed no evidence of distant metastatic disease with uptake only at the site of the primary tumor.
Following further multidisciplinary discussion, the decision was to offer surgical resection provided that removal of all previously identified tumor sites was achievable.
Surgical technique
Phase 1: left thoracoscopic resection of aortovertebral nodes
With the patient prone, three thoracoscopic ports were introduced into the left chest (Fig. 2a). Using hook diathermy the pleura was opened from the diaphragmatic hiatus to the thoracic inlet (Fig. 2b and c). All tissue between the aorta, the anterior longitudinal ligament, and the hemiazygos vein was mobilized (Fig. 2d), and nodes above and below the aortic arch were resected. The vagus was divided 1 cm below the aortic arch, and the left pleura above and below the arch was resected en bloc with the esophagus.
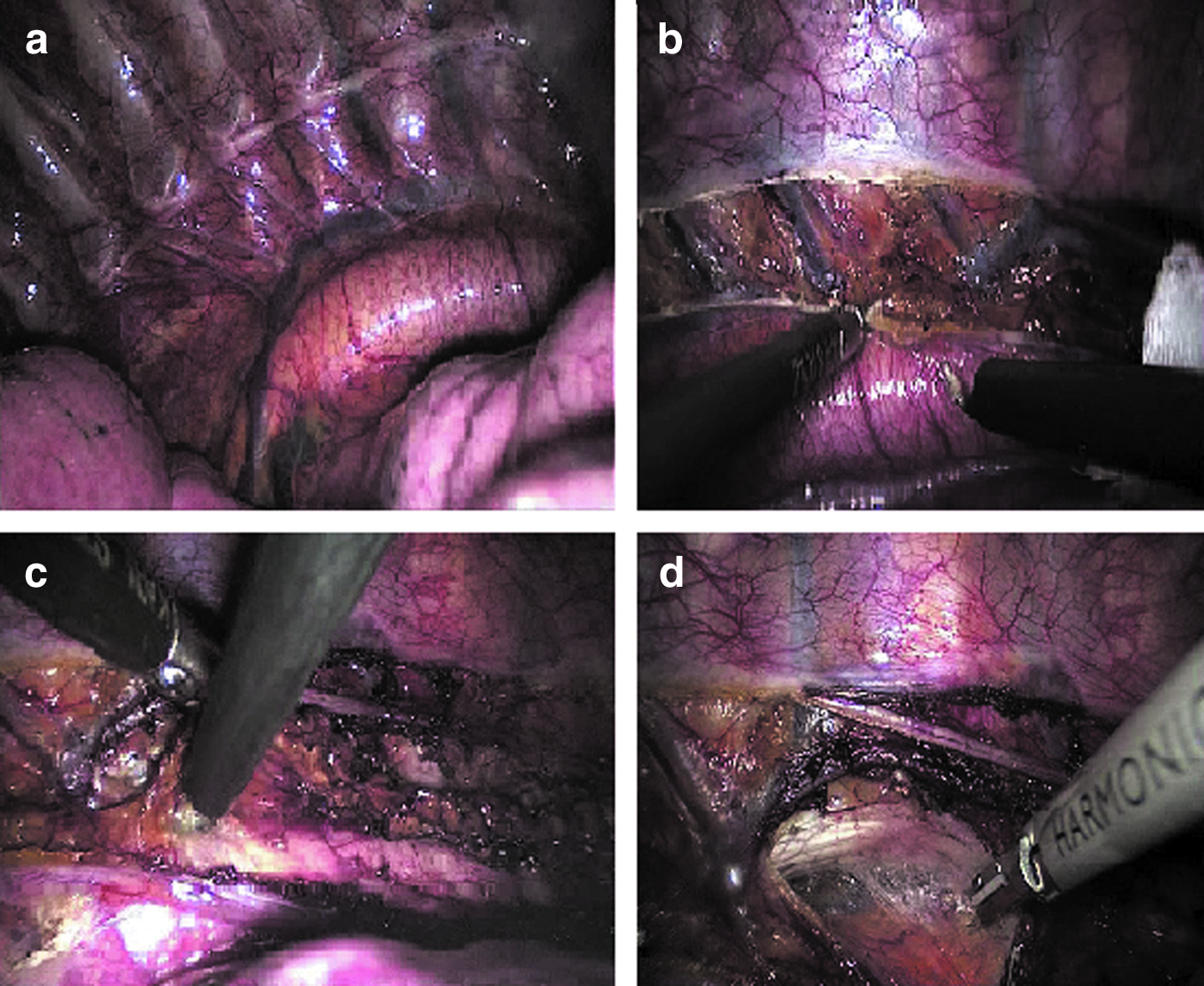
Thoracoscopic resection of the left aortovertebral lymph nodes:
Phase 2: esophageal mobilization and radical lymph node dissection
The patient was placed in a left lateral decubitus position. Through a right fourth intercostal space thoracotomy the esophagus was mobilized from the hiatus into the root of the neck with en bloc resection of all peri-esophageal, bronchial, and carinal nodes, thoracic duct, para-aortic nodes, and the overlying pleura. In addition, a right and left paratracheal dissection, clearing both recurrent laryngeal nerves, was performed (Fig. 3a and b), and a window of pericardium was excised where the tumor was adherent (Fig. 3c).

Mediastinal dissection in the right chest:
Phase 3: gastric mobilization with radical suprapancreatic nodal dissection
The patient was placed supine, and a midline laparotomy was performed. The Kocher maneuver was performed on the duodenum, and the stomach was mobilized on the right gastric and right gastro-epiploic pedicles. Nodal stations 1–3, 7, 8a, 8p, 9, 11p, 11d, and 12a were resected en bloc (Fig. 3d). The esophagus was delivered into the abdomen following division in the neck. The gastric tube was fashioned, a Heineke–Mikulicz pyloroplasty was performed, and a feeding jejunostomy was inserted.
Phase 4: right thyroid lobectomy, bilateral level IV and VI lymph node dissection, and esophagogastric anastomosis
Synchronous with the abdominal phase, through a collar-line incision, the right lobe of the thyroid and bilateral level IV and VI cervical lymph nodes were resected. The gastric tube was delivered into the neck, and a hand-sewn end-to-side esophagogastric anastomosis was performed.
Results
The patient was extubated the morning after surgery and spent 4 days on the critical care unit. She developed a mild respiratory infection treated with intravenous antibiotics but otherwise made a steady recovery and was discharged home on postoperative Day 16.
Histopathology revealed a poorly differentiated squamous cell carcinoma of the distal esophagus, stage ypT3-L1-V0-N1-G3. Two lymph nodes out of the 75 resected contained tumor: one right paracardial (station 1) and one left thoracic aortovertebral node. No residual tumor was identified in the cervical nodes or thyroid.
The patient is alive and well 15 months following surgery (37 months following diagnosis), with no evidence of disease recurrence.
Discussion
Esophageal cancer has a poor overall survival because of the high percentage of patients with inoperable and incurable disease at the time of presentation. In Japan, where squamous cell carcinoma is the predominant histological type, a strategy of aggressive extended lymphadenectomy has resulted in improved long-term survival.3–5 Despite this, such radical resections are rarely performed in Western countries.
In this report we present a young patient with locally advanced distal esophageal squamous carcinoma with evidence of cervical and paravertebral node metastases, initially considered beyond operable or curative treatment. Palliative chemotherapy resulted in good short-term disease control with the subsequent development of recurrent symptoms due to progression at the primary site alone. A novel strategy of surgical resection was devised to achieve tumor clearance by adding a left paravertebral lymphadenectomy to a Japanese-style radical three-phase esophagectomy with three-field lymph node dissection. Whether or not this radical approach has altered the natural history of her disease is uncertain, yet the patient is clinically well and disease-free 15 months following resection. We acknowledge that this is a tailored approach to an individual stage and disease pattern, but the fundamental principles of cancer surgery have been adhered to with a positive outcome thus far. We would emphasize the critical importance of accurate staging for appropriate treatment and a tailored surgical approach to achieve complete (R0) resection in this challenging disease.
Footnotes
Acknowledgments
We thank Professor S. Michael Griffin, Royal Victoria Infirmary, Newcastle Upon Tyne, United Kingdom, for his involvement in the extended discussion beyond our own multidisciplinary team.
Disclosure Statement
No competing financial interests exist.