
Abstract
Abstract
A comprehensive review of intraluminal duodenal diverticulum (IDD) is presented, along with a report of a completely laparoscopic excision of this duodenal abnormality as well as a report of magnetic resonance cholangiopancreatography demonstrating the classic fluoroscopic “wind sock sign” pathognomonic appearance of IDD. IDD may easily be missed unless one specifically considers this entity in patients presenting with symptoms of foregut disease. Patients with IDD typically present in the fourth decade of life with duration of symptoms less than 5 years that typically include pain, nausea and vomiting, pancreatitis, and gastrointestinal bleeding. Diagnosis usually requires imaging studies and upper gastrointestinal endoscopy. Laparoscopic excision is recommended because of superior visualization of significant intestinal anatomic abnormalities, the need for accurate ampullary localization, and the ability to facilitate complete diverticular excision while maintaining biliary and pancreatic ductal integrity. Review of surgical literature suggests that IDD results from congenital duodenal developmental abnormalities matured by long-term duodenal peristalsis.
Introduction
Subjects and Methods
A thorough computer search of the English surgical literature from 1885 to 2009 yielded 70 reports of IDD representing 81 cases.1–70 Data were collected identifying age of onset, length of symptoms, symptoms on presentation, prediagnostic imagery, prediagnostic abdominal surgery, extraduodenal congenital abnormalities, foreign body entrapment, web attachment, and juxtaposition to ampulla, as well as diverticular dimensions and aperture size. Not all reports included each data point.
Results
The median age of presentation of IDD is in the fourth decade of life (Fig. 1), with over half of cases presenting with symptoms less than 5 years prior to diagnosis (Fig. 2). IDD demonstrates an equal gender distribution (41 men:38 women).
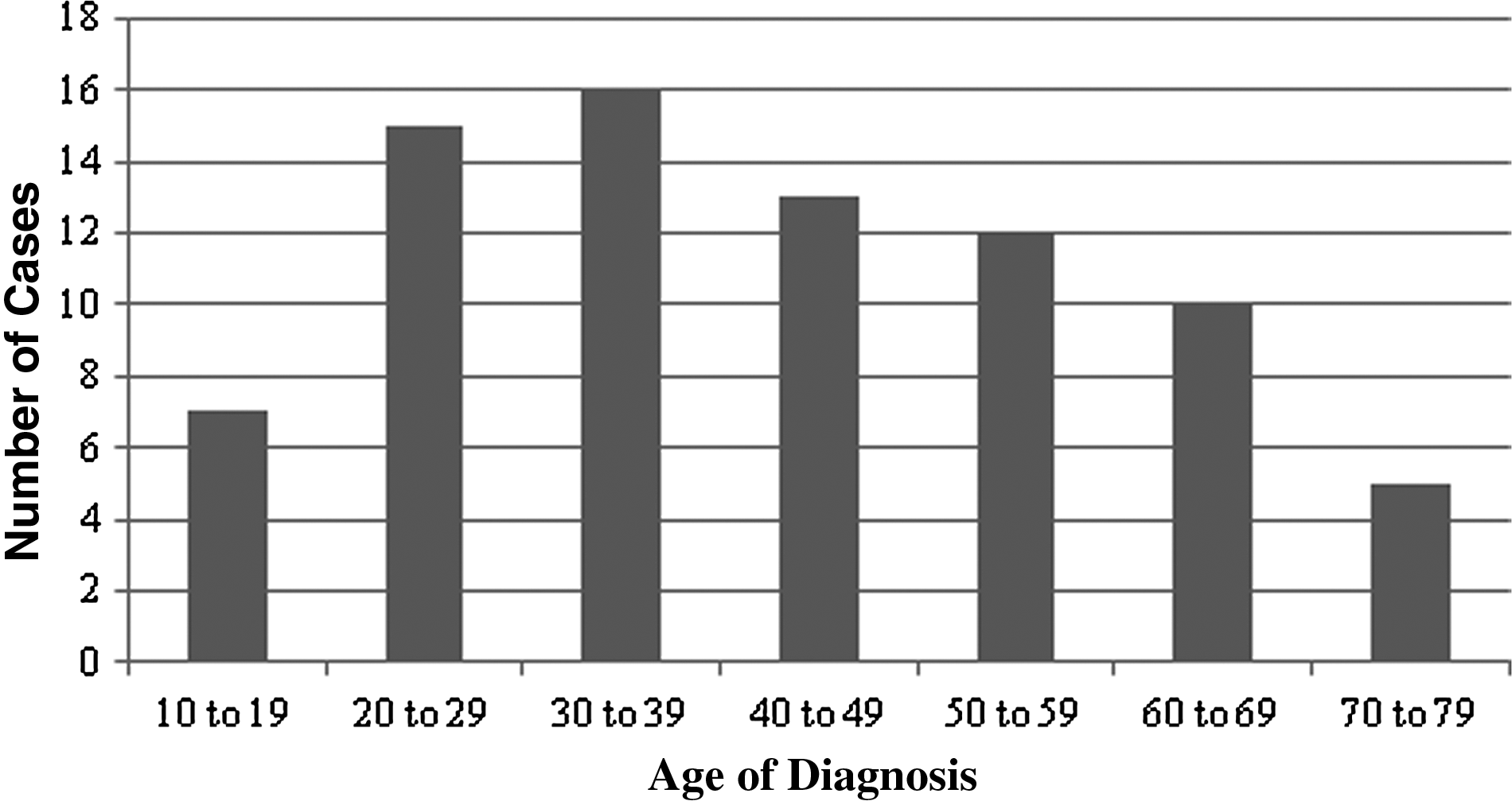
Age (years) at diagnosis of intraluminal duodenal diverticulum based on literature review.
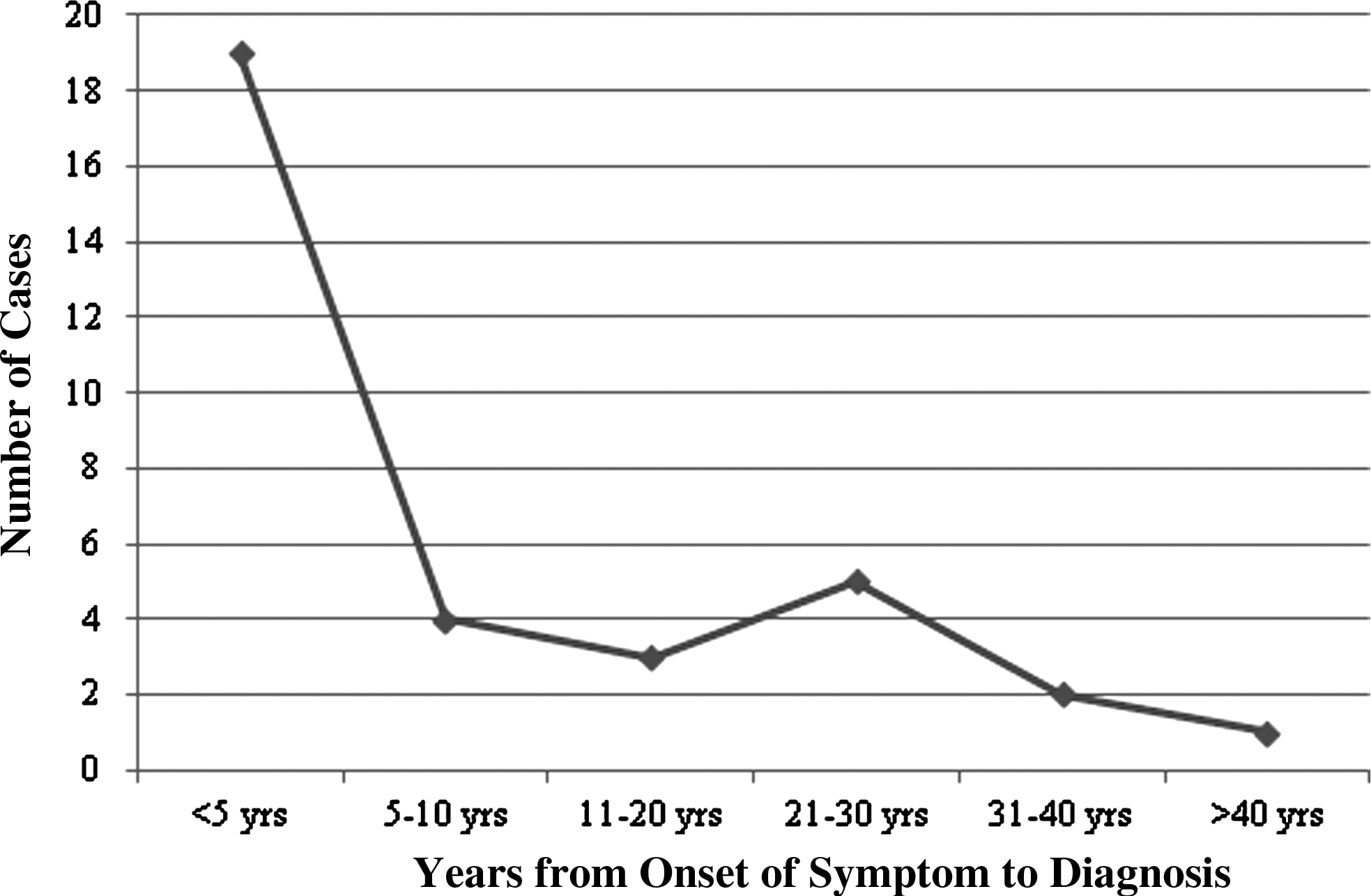
Onset of symptoms prior to diagnosis of intraluminal duodenal diverticulum (IDD) based on literature review.
Fifty-nine reports included symptoms at presentation. Pain was the predominant presenting symptom (68%), with nausea and vomiting (46%), pancreatitis (32%), and gastrointestinal bleeding (17%) being the most common presenting symptoms (Table 1).
The preoperative diagnostic imaging study (n=72) most commonly used to diagnose IDD was upper gastrointestinal (UGI) contrast study followed by UGI endoscopy (UGIE) (Table 2).
GI, gastrointestinal; IVC, intravenous pylography; OCG, oral cholecystogram.
The prime indication for surgery prior to diagnosis of IDD was for the symptoms of gastric outlet obstruction. Relevant prediagnostic abdominal surgery included single cases of pyloromyotomy, gastrojejunostomy for annular pancreas or duodenal atresia, vagotomy with pyloroplasty, gastrocystostomy for pancreatic pseudocyst, cholecystectomy, and appendectomy.
The predominant procedure performed to address the symptoms of IDD was complete open excision of the diverticulum (55%), with anatomic bypass (gastrojejunostomy, duodenojejunostomy, and duodenoduodenostomy) the second most commonly performed procedure (29%) (Table 3). Sphincteroplasty was required in only 3 cases (5%).
IDD, intraluminal duodenal diverticulum.
Extraduodenal abnormalities identified in this review include two reports of annular pancreas,2,6 three reports of extrapancreatic tissue rests,7–9 four reports of malrotation of intestines,2,6,10 pancreatic divisum, and single reports of trisomy 21, Meckel's diverticulum, and situs inversus.11,12 Other congenital conditions reported include congenital cardiac abnormalities, imperforate anus, Hirschsprung's disease, omphalocele, hypoplastic kidney, extrophy of the bladder, and superior mesenteric artery syndrome.13,14
Five reports describe foreign bodies trapped in the web and include peas and “other food debris,” 15 multiple gallstones, 14 marbles, 13 an eroded penny, 16 and one diverticulum that contained three coins ingested when the patient was 13 years old. 17
The position of the web in relation to the ampulla of Vater (n=44) identifies the web usually attached to the duodenal wall proximal to the ampulla (52%), followed by the web attached at or near the ampulla (30%), and least often attached distal to the ampulla (18%) (Table 4). The position of web attachment is predominantly medial (11/16 cases) and less commonly posterior (3/16) and lateral (2/16). Of those reports that recorded the degree of intraduodenal wall attachment (n=12), the web was most commonly attached 100% circumferentially (8/12) and less commonly to 20% of the internal duodenal wall (3/12) or 50% of the wall circumference (1/12).
IDD, intraluminal duodenal diverticulum.
Many authors emphasize an unpredictable ampulla/IDD juxtaposition and stress the importance of maintaining biliary and pancreatic drainage during web excision. In 17 of the 81 cases the authors noted significant abnormalities in ampullary/IDD orientation, with the most common presentation of these two structures within 2–3 mm (7/17 cases), followed by the ampulla identified between two webs (3/17). The pancreatic duct joined the duodenum separately from the biliary duct in 18% of cases, most commonly above the web attachment (Table 4).
The mean length of IDD is 6.7 cm, with the median length 5.0 cm (n=21). The width of the IDD reported is under 3 cm (6/9 cases), with three cases reporting widths of 4, 5, and 6 cm. The IDD opening that allows luminal passage of food contents ranged from a “pin hole” to 20 mm, with a mean of 6.8 mm and a median of 5 mm.
First Report of Laparoscopic Excision of IDD
A 32-year-old Greek woman presented with persistent vomiting and severe epigastric pain, which radiated to the chest and lower back. The patient's history included a 2-year history of epigastric pain, with gastroesophageal reflux disease and recurrent pancreatitis. There was no history of excess alcohol intake or previously identified gallstones. Biochemical investigation, including white blood cell count, sedimentation rate, pancreatic enzymes (amylase and lipase), and urinalysis were all within normal limits.
Contrast-enhanced computed tomography of the abdomen and pelvis failed to diagnose IDD but did identify multiple congenital abnormalities, including complete malrotation of the bowel, a septate or didelphys uterus, and suggested possible pancreas divisum. The duodenum, ligament of Treitz, and the small bowel occupied the right hemi-abdomen, and the entire colon was located in the left hemi-abdomen.
Magnetic resonance cholangiopancreatography without gadolinium was performed to further evaluate the pancreas. Fat-suppressed coronal single-shot fast spin echo T2-weighted images identified a 3.6-×4.5-cm fluid collection with two concentric round foci of circumferential T2 hypo-intense signal, immediately inferior to the gallbladder fossa. These appearances were typical of a “wind sock” deformity, illustrating the two adjacent mucosal surfaces of the duodenum and the intraluminal diverticulum. No pancreatic abnormality was identified (Figs. 3 and 4).
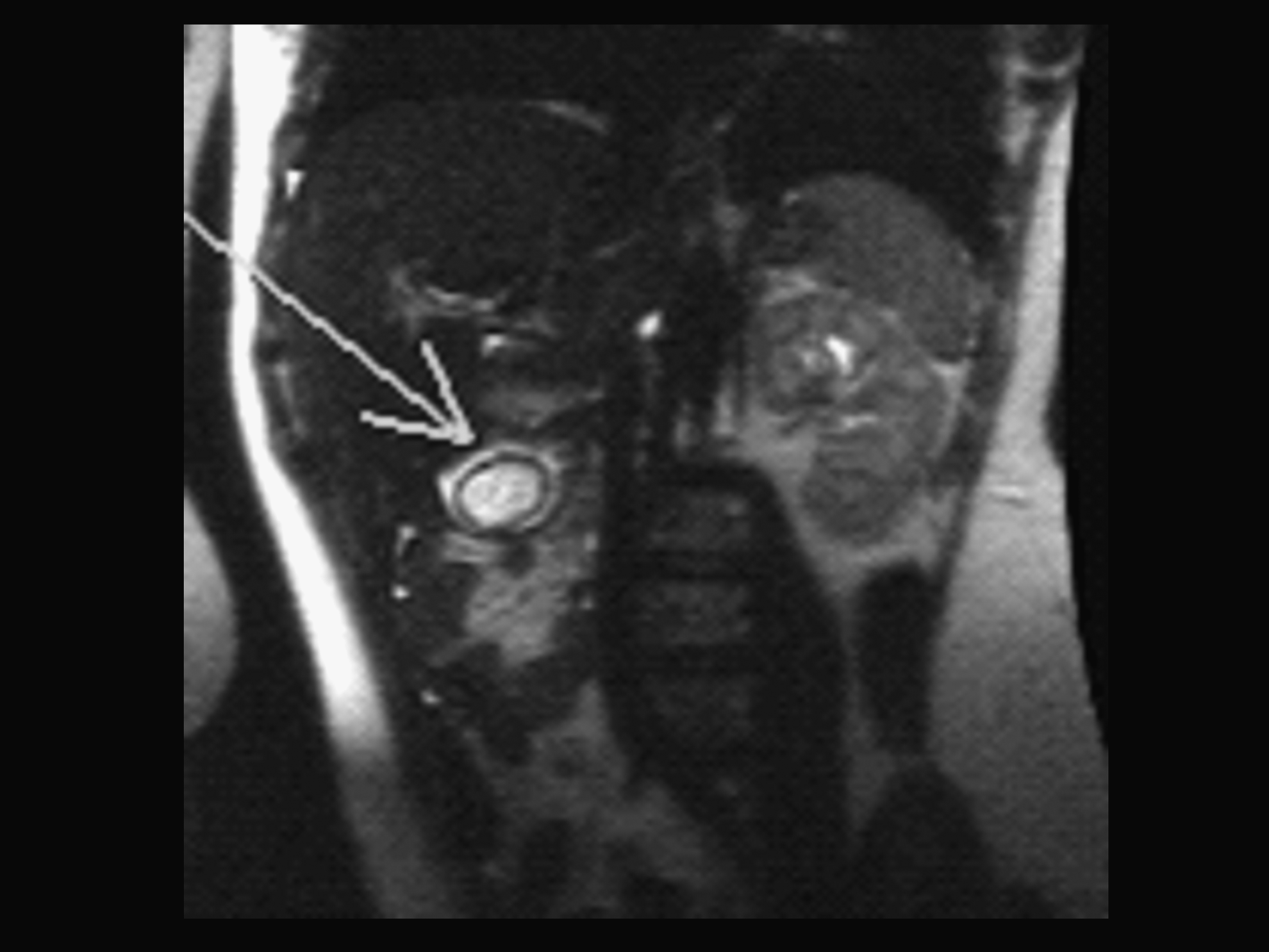
Magnetic resonance imaging of our patient with intraluminal duodenal diverticulum. Fat-suppressed coronal single-shot fast spin echo T2-weighted image demonstrates a 3.6-×4.5-cm fluid collection (arrow) with two concentric round foci of circumferential T2 hypointense signal immediately inferior to the gallbladder fossa.
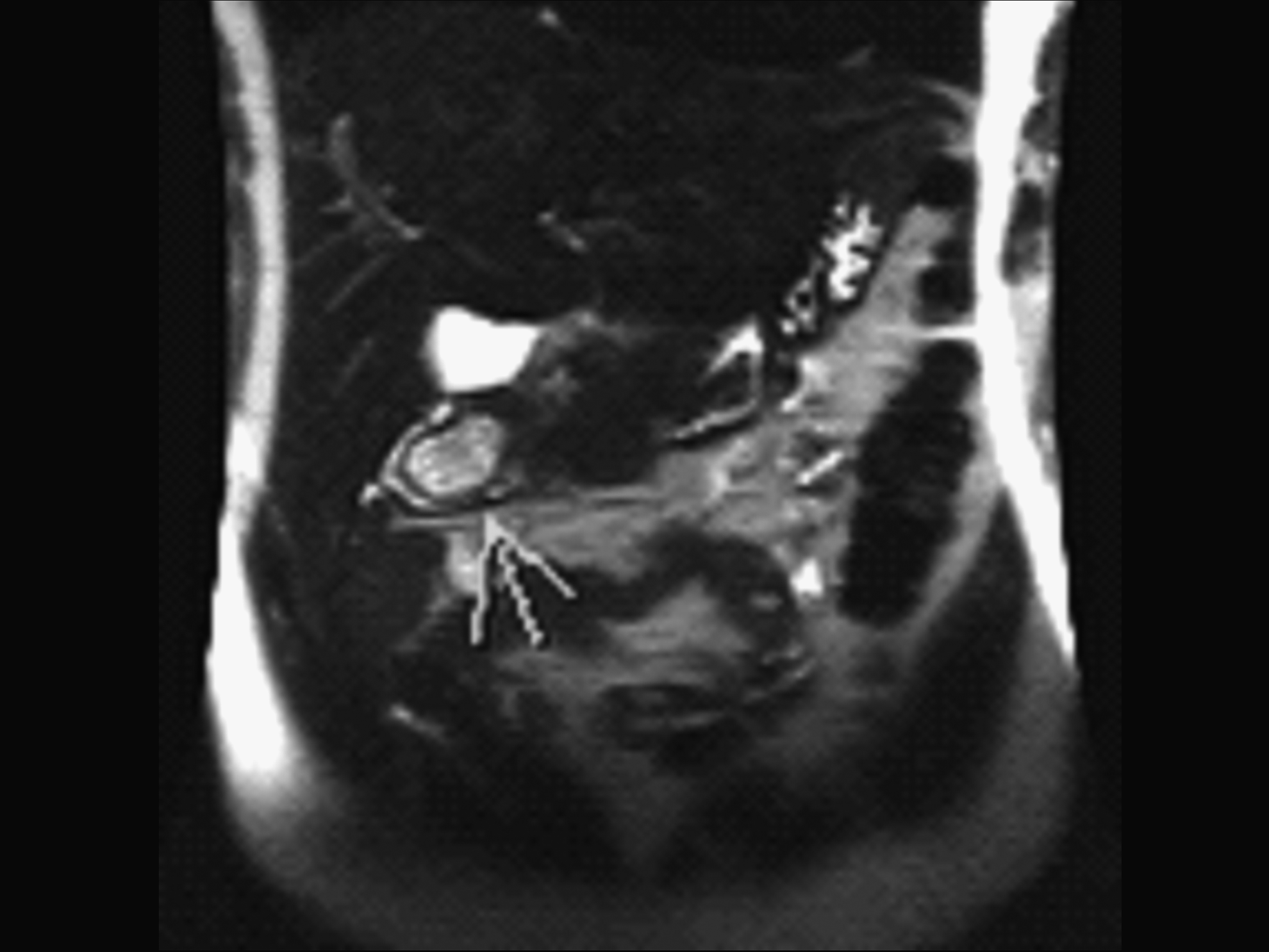
Magnetic resonance imaging of our patient with intraluminal duodenal diverticulum. Fat-suppressed coronal oblique single-shot fast spin echo T2-weighted image shows the “wind sock sign” pathognomonic of intraduodenal diverticulum (arrow).
Esophagogastroduodenoscopy showed a moderate quantity of food in the duodenum obscuring the diverticulum. Repeated attempts to clear the lumen were unsuccessful as food particles continued to “re-enter” the lumen. This finding was suggestive, but not diagnostic of, an IDD.
A UGI contrast study demonstrated a barium-filled sac lying within the duodenum, separated by a narrow, radiolucent line or “halo,” representing the wall of the diverticulum (Fig. 5). This study confirmed the magnetic resonance imaging finding of a “wind sock sign,” pathognomonic of an IDD.

Upper gastrointestinal contrast study of our patient with intraluminal duodenal diverticulum. Upper gastrointestinal contrast study demonstrating a barium-filled sac, lying entirely within the duodenum, surrounded by a narrow radiolucent line classic of the “wind sock sign” pathognomonic of intraduodenal diverticulum. Barium fills the diverticulum and surrounding duodenum. The radiolucent line depicts the normal duodenal mucosal lining of the diverticulum arising just 3–4 cm distal to the pyloric thickening.
With the patient in a split leg prone position, a 12-mm laparoscopic trocar was placed in the umbilical position with two manipulating 12-mm trocars 8 cm to the left and right of the umbilical position. Two 5-mm trocars were placed in the left and right upper quadrants for retraction.
Laparoscopic surgical exploration identified complete intestinal malrotation, with the colon residing to the left of the abdominal cavity and the small bowel to the right. The duodenum did not sweep medially, and with minimal peritoneal posterior attachment, neither a Ladd's procedure nor a Kocher maneuver to expose the site of the diverticulum was required. The duodenum was dilated proximal to the barium-filled IDD. Following an antimesenteric duodenotomy, the ampulla of Vater could not be identified; however, bile was found flowing from a nondescript fold of mucosa near the outflow of the IDD distal to the diverticular attachment. This opening was catheterized, and a cholangiogram was performed, which showed unimpeded passage of contrast into the common duct and common hepatic ducts. The pancreatic duct was not demonstrated.
Extension of the limited duodenotomy revealed attachment of the diverticulum just proximal to the ampulla of Vater, with the outlet of intestinal flow through the diverticulum at the level of the ampulla (Figs. 6 and 7). Fortunately, a protective catheter could be placed in the common bile duct during laparoscopic resection of the diverticulum using a Harmonic® scalpel (Ethicon, a Johnson and Johnson Company, Cincinnati, OH). This allowed detachment of the diverticulum from the luminal surface without compromising ampullary flow of biliary and pancreatic secretions. An inability to identify the ampulla would require either an extension of the duodenotomy with a more complete visualization of the mucosa or common bile duct cannulation before proceeding with diverticular excision. The duodenal mucosa at the diverticular detachment was not re-approximated to minimize the possibility of ductal injury or encroachment. Using stay sutures at the midpositions of the enterotomy, the longitudinal duodenotomy was partially closed in a horizontal direction using intracorporeal staples, with the remaining small portion hand-sewn with a single layer of 2-0 silk. A transnasogastric air tube was shown to distend the duodenum without evidence of leak. The periduodenal drain was removed following a postoperative diatrizoate meglumine/diatrizoate sodium (Gastrografin®; Bracco Diagnostics, Princeton, NJ) UGI series that revealed unobstructed contrast flow through the site of diverticular resection once the patient tolerated regular diet. The patient was discharged home on postoperative Day 5. Pathologic evaluation of the diverticulum revealed small bowel mucosa without significant inflammation. Focal granulomatous mucosa was noted on both the superior and inferior surfaces. The surrounding duodenal tissue revealed congestion and edema but no inflammatory changes. There were no ectopic gastric, pancreatic, or malignant elements identified. Evaluation of the patient 4 years after laparoscopy confirmed the absence of both gastric outlet obstructive symptoms and recurrent pancreatitis.
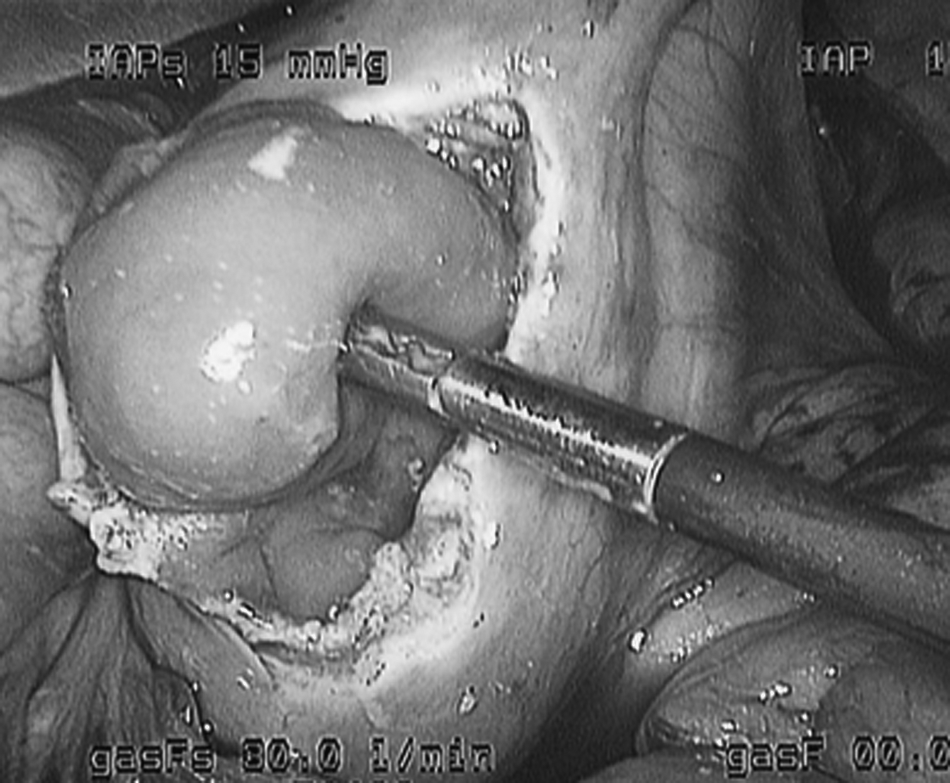
Intraoperative laparoscopic photograph of our patient with intraluminal duodenal diverticulum shows the intraduodenal diverticulum presenting through an antimesenteric duodenotomy supported by a laparoscopic grasper elevating the intraluminal duodenal diverticulum to reveal the small opening at the base of the diverticulum through which enteral flow escapes. The opening of diverticulum is at the level of the ampulla of Vater.
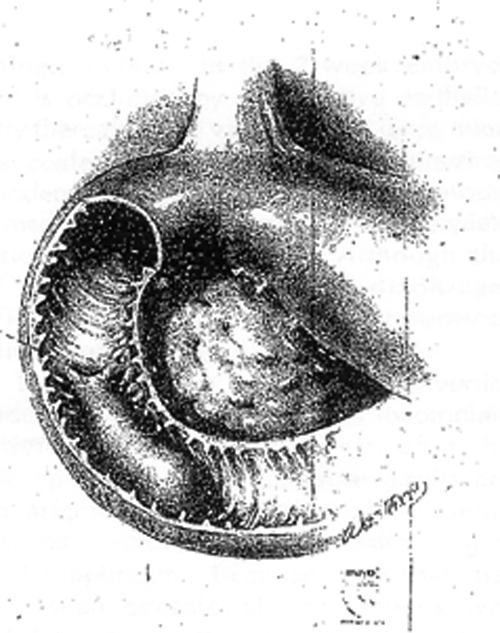
Intraduodenal diverticulum. Reprinted with permission from Fleming et al. 7
Discussion
Anatomy
The anatomic positions of both the diverticulum and ampulla, as well as the degree of diverticular attachment, are unpredictable (Table 4), making preoperative and intraoperative identification of duodenal anatomy and ampullary position essential prior to diverticular excision in order to maintain unimpeded postoperative biliary and pancreatic drainage.
We have found that IDD most often attaches circumferentially (8/12 cases), in contrast to previous reports suggesting predominantly partial attachment to the walls of the duodenum,4,13,18 on the medial, posterior, or lateral duodenal walls.14,17,19,20 Partial attachment of the anterior duodenal wall has not been reported.
Diverticular attachment is most commonly proximal to the ampulla (52%), followed by attachment at or near the ampulla (30%) and least commonly distal to the ampulla (18%). With the ampulla near or distal to diverticular attachment in over 80% of cases, endoscopic identification of the ampulla can be difficult or impossible without blind transection of the diverticulum, endangering biliary drainage. This finding is in contrast to previous articles that have reported nearly equal attachments above and below the ampulla.14,21
Diverticular length is approximately 5–7 cm and has been described reaching the transverse duodenum, 22 making endoscopic diagnosis of IDD challenging unless the endoscope is advanced to the apex of the diverticulum. Depending upon the degree of wall attachment, IDD can range from 3 to 6 cm in width. D'Allessio et al. 6 and Hiraoka et al. 23 described three configurations of IDD, including funnel, pocket, and oval shapes, based upon degree of attachment, size of aperture, and sac contents. Identification of a small (5–8 mm), eccentric luminal aperture 24 at the apex,14,18,25 or less commonly at the proximal attachment, 24 of the diverticulum is important to confirm diagnosis. Food and ingested foreign bodies often obscure the end of the diverticulum, making diagnosis difficult. Some reports have identified foreign bodies incarcerated within an IDD for many years. 17
Embryology
At 7 weeks of gestation, the primitive duodenum is occluded by epithelial cells that subsequently recanalize with the coalescence of lateral and medial vacuoles that define the mature duodenal lumen.3,12,26,27 Any disruption of this process can result in duodenal atresia, web formation, and duodenal stenosis in 9000–40,000 live births12,13 as well as contributing to a myriad of other congenital abnormalities.2,13,18,26–28 Most anatomic duodenal abnormalities, including IDD, are close to the ampulla. 12 Heilbrun and Boyden 4 believed that IDD is a vestigial remnant of either the medial or lateral vacuole but did not reject the possibility that IDD can result from the maturation of a congenital duodenal web elongated by peristaltic transformation.7,14,18,20,29 The concept that IDD forms as an initial developmental abnormality matured over time by peristaltic action is consistent with our observation that most patients with symptomatic IDD present in midlife with recent onset of symptoms (Figs. 1 and 2).
Presentation
Classic presentation of a patient with IDD is in the fourth decade of life with an acute exacerbation of chronic epigastric pain presenting intermittently for less than 5 years (Fig. 1). Incomplete obstruction of the duodenal lumen, characteristic of IDD, can delay onset of gastric outlet obstruction symptoms for many years. 13 Nausea and vomiting are noted in half of patients, acute or chronic pancreatitis in a third, 30 and gastrointestinal bleeding in a sixth of patients5,9,19,25,31 (Table 1). With these nonspecific symptoms, the differential diagnosis includes a wide range of foregut pathology, often allowing IDD to be overlooked. 5
Imaging
Nelson 32 was first to report radiographic imaging of IDD in 1947, followed by Kinzer 33 2 years later, who is credited with coining the term “intraluminal duodenal diverticulum.” The diagnosis of IDD is difficult to make based upon presentation of symptoms alone. Imaging studies are a necessary component of diagnosis. The majority of IDD were diagnosed with UGI contrast studies (55%); however, UGIE (20%) and, less commonly, computed tomography (7%) have been used more recently to confirm the diagnosis (Table 2). Many authors stress the difficulty in identifying IDD on endoscopy.2,6,14,18,25 This is due to both the length and the circumferential attachment of the diverticulum, as well as trapped food that frequently obscures the apex of the diverticulum. Other diagnostic modalities that have been used to diagnose IDD have included oral cholecystogram, intravenous cholangiogram, 34 biliary scintogram, abdominal ultrasound, cholangiogram, and even barium enema (Table 2). Although we have presented a report of definitive imaging of IDD using magnetic resonance cholangiopancreatography (Figs. 3 and 4), the more commonly used diagnostic modalities of UGIE and computed tomography are both adequate and less expensive initial diagnostic studies.
Treatment
The prime indication for surgery performed prior to the diagnosis of IDD was for gastric outlet obstructive symptoms, with gastrojejunostomy most commonly performed. After diagnosis, the most common corrective procedure was complete excision of the diverticulum (55%), with gastrojejunostomy and duodenojejunostomy performed less often and described predominantly in earlier surgical reports.
For definitive correction of IDD, we agree with most authors that complete excision of the diverticulum with generous mobilization of the duodenum (the Kocher maneuver) through an antimesenteric duodenotomy is recommended20,28,35 (Table 3). Unequivocal identification of the ampulla of Vater along with clarification of ductal anatomy with intraoperative cholangiography prior to diverticular incision or excision is advised to preserve biliary and pancreatic drainage.2,3,6 Variable diverticular and ampullary anatomy makes the precise location and protection of the ampulla difficult. 15 Sphincterotomy or sphincteroplasty may be necessary to maintain adequate biliary drainage.
Hajiro et al. 10 reported the first case of successful endoscopic resection of an IDD in 1979 with good long-term results but was unable to identify the ampulla prior to excision. Four years later, Karoll et al. 36 reported endoscopic dilatation of IDD with their patient asymptomatic at 2-year follow-up. Finnie et al. 15 reported sphincterotome enlargement of the tip of a diverticulum in 1993 with an asymptomatic 12-month follow-up.
Recognizing the characteristically limited visualization of endoscopic examination of the duodenum 17 and the inconsistent duodenal anatomy with IDD and considering the morbidity of open exploration, we advise laparoscopic excision of the IDD. Laparoscopic approach allows complete visualization and evaluation of intestinal malrotation, identification of altered duodenal anatomy including proximal dilatation, ampullary localization, and canalization, and complete diverticular excision while maintaining biliary ductal integrity. Excision of the diverticulum with a Harmonic scalpel results in excellent healing of the duodenal mucosa without the need for mucosal re-approximation. Prior to opening the duodenum, proximal dilatation is often reported, but duodenal narrowing is rarely observed. 14
Pathology
Microscopic evaluation of IDD demonstrates normal small bowel mucosa without significant inflammation.3,35 Often a poorly formed muscularis mucosa will be identified, but a muscularis propria is rarely noted. 11 Focal granulomatous mucosa can be identified on either superior or inferior surfaces of the diverticulum. The surrounding duodenal tissue will often show congestion and edema, but rarely inflammatory changes. Ectopic pancreatic elements have been identified.7–9
Conclusions
IDD may be easily missed unless one specifically considers this entity in patients presenting with symptoms of foregut disease. Patients with IDD typically present in the fourth decade of life with duration of symptoms less than 5 years that typically include pain, nausea and vomiting, pancreatitis, and gastrointestinal bleeding. Diagnosis usually requires imaging studies and UGIE. As opposed to open laparotomy, the laparoscopic approach is recommended because of superior visualization of significant intestinal anatomic abnormalities, the need for accurate ampullary localization, and the ability to facilitate complete diverticular excision while maintaining biliary and pancreatic ductal integrity.
Review of surgical literature suggests that IDD results from duodenal developmental abnormalities matured by duodenal peristalsis. Magnetic resonance cholangiopancreatography is an adjunctive diagnostic modality that clearly demonstrates the classic fluoroscopic “wind sock sign” pathognomonic appearance of an intraluminal duodenal diverticulum.
Footnotes
Acknowledgments
We would like to thank Evan Wasserman, MD, from the Department of Radiology, Norwalk Hospital, Jill Golrick, Chief Medical Librarian, Norwalk Hospital, Christopher Meinke for development of figures and proofreading, and, most importantly, Lori Anne Meinke for sustained and unwavering support services.
Disclosure Statement
No competing financial interests exist.