
Abstract
Abstract
Background:
Totally laparoscopic total gastrectomy (TLTG) for gastric cancer is still uncommon because of the technical difficulty of performing the esophagojejunostomy laparoscopically. We have developed a secure technique for intracorporeal esophagojejunostomy and successfully performed the TLTG method using an endoscopic linear stapler. Our experiences with this method are reported here.
Subjects and Methods:
Between July 2009 and May 2010, 124 patients with gastric cancer underwent TLTG using endoscopic linear staplers in one institution. The clinicopathological data and surgical outcomes of the first 70 cases and the subsequent 54 cases were reviewed retrospectively and compared because technical improvements were instituted after the 70th case.
Results:
The two groups differed significantly in terms of mean operation time (189.0 versus 148.3 minutes, P<.001), overall postoperative complication rate (37.1% versus 13.0%, P=.003), severe postoperative complication rate (15.7% versus 3.7%, P=.030), and intraoperative event rate (12.9% versus 1.9%, P=.042).
Conclusions:
The early period of performing TLTG using an endoscopic linear stapler was associated with a high morbidity rate. This improved significantly when key technical changes were introduced. However, surgeons who are inexperienced in laparoscopic gastrectomy should be careful when performing TLTG because it involves many complex processes. The account in this report of our experiences with TLTG may help surgeons to master this method faster and more safely.
Introduction
More recently, several investigators reported various types of intracorporeal esophagojejunostomy.12–16 However, totally laparoscopic total gastrectomy (TLTG) procedures involve complex methods that can be difficult to perform. In particular, the outcomes of TLTG using linear staplers have not been reported previously.
The present report describes our method of TLTG using an endoscopic linear stapler. The clinical utility of TLTG for the surgical management of gastric cancer is assessed.
Subjects and Methods
Patients
The prospectively collected data of 124 consecutive patients who underwent TLTG for early gastric cancer between July 2009 and May 2010 at Asan Medical Center (Seoul, Korea) were reviewed. All patients underwent D1+β lymph node or D2 dissections. To evaluate the impact of the surgeon learning the TLTG method on early surgical outcomes, the 124 patients were divided into two groups: the first 70 cases and the subsequent 54 cases. This division reflects the introduction of several devised technical improvements after the 70th case.
Surgical techniques
The patient was placed in the reverse Trendelenburg position. A carbon dioxide pneumoperitoneum was formed from the umbilical port, with pressure maintained between 12 and 15 mm Hg. Total gastrectomy was performed using four trocar ports that were placed in a U-shape pattern (Fig. 1). To retract the liver, the intracorporeal suturing of the pars condensa and right crus was performed, and then the thread on both sides of the xiphoid process retrieved by a suture-passer was tied over the skin to serve as a lift for the liver (Fig. 2). If the operating field was not sufficient, an additional 5-mm trocar was inserted into the epigastric area to retract the liver.
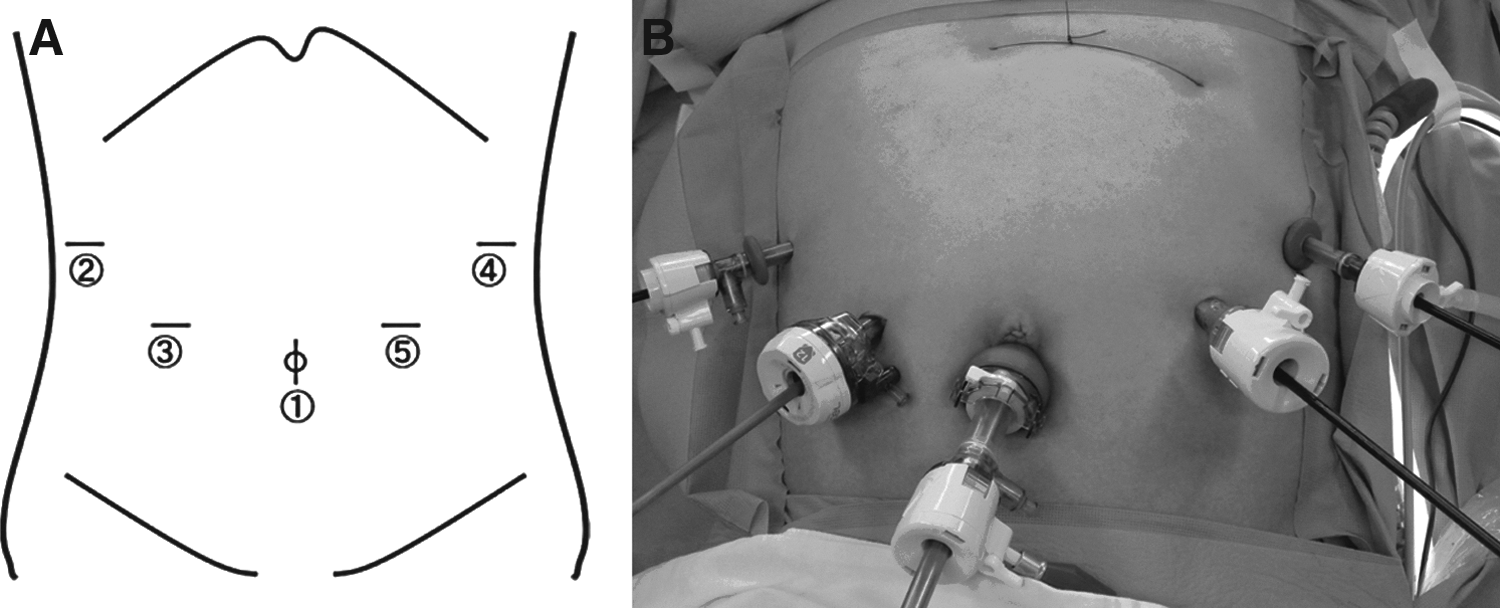
Placement of the trocar.

How to retract the liver during laparoscopic gastrectomy. To retract the liver, the intracorporeal suturing of the pars condensa and right crus was performed, and then retrieved thread on both sides of the xiphoid process by a suture-passer was tied over the skin to lift the liver.
Dissection was begun by dividing the greater omentum from the midportion of the gastroepiploic arcade to the left gastroepiploic vessel. The lymph nodes around the left gastroepiploic and short gastric vessels were dissected. After the lymph nodes around the short gastric area were dissected, the infrapyloric area was dissected. After lymph node dissection around the suprapyloric area, the duodenum was transected just below the duodenal bulb by using an endoscopic linear stapler (Echelon™ Flex™ 60; Ethicon, Blue Ash, OH) with a closed stapler height of 1.5 mm. Subsequently, the lymph nodes around the common hepatic, proximal or distal splenic, celiac, and left gastric arteries were dissected (in that order), followed by dissection of the lymph nodes around the right paracardial and lesser curvature areas.
After all lymph nodes were cleared, nearly two-thirds of the esophagus diameter was transected 2 cm above the gastroesophageal junction using the endoscopic linear stapler (Echelon Flex 60) (Fig. 3A), and the first intracorporeal suture was placed at the end of the stapled line to retract the esophageal stump (Fig. 3B). This suture was cut 15 cm from the esophageal stump, which it was retracted by the first assistant during reconstruction of the esophagojejunostomy. The unstapled esophageal stump was then transected with laparoscopic scissors after the remnant stomach was grasped with a laparoscopic intestinal clamp to avoid cancer cell spillage (Fig. 3C). To make the lumen of the esophagus easier to detect, a second round of intracorporeal suture was placed at the small esophagostomy of the esophageal stump, and it was extracted outside the abdomen through the right lower trocar to retract it, which prevented slipping of the esophageal mucosa and submucosa during reconstruction of the esophagojejunal anastomosis (Fig. 3D). The specimen was subsequently removed through the umbilical port site by extending the incision as an I-shaped incision that was approximately 3–4 cm long. After the specimen was removed, the umbilical trocar was reintroduced, and three or four interrupted sutures were tied at the umbilical incision to reinstate the pneumoperitoneum. The proximal resection margin of the specimen was examined pathologically.
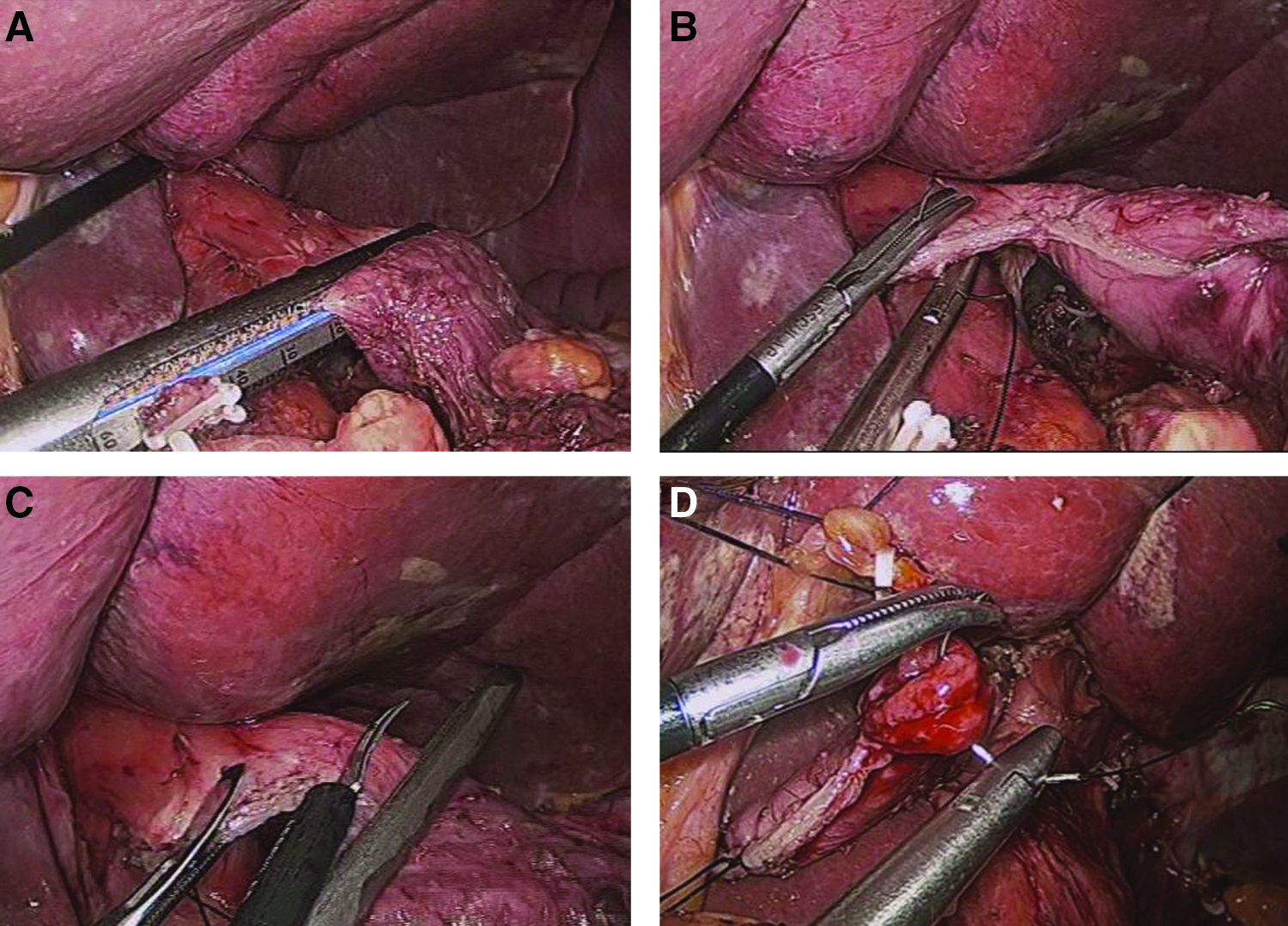
How to make an esophageal stump.
The jejunum was then divided 20 cm below the ligament of Treitz by using an endoscopic linear stapler (Echelon Flex 60), and an efferent loop was turned in a counterclockwise direction to reconstruct the esophagojejunostomy. An enterostomy of the jejunum was made in the anti-mesenteric side of the Roux-en-Y limb by using laparoscopic scissors, and an endoscopic linear stapler (ETS Straight™ 45; Endopath) with a closed stapler height of 1.5 mm was inserted into the esophagostomy and enterostomy of the jejunum to form an esophagojejunal anastomosis (Fig. 4B).
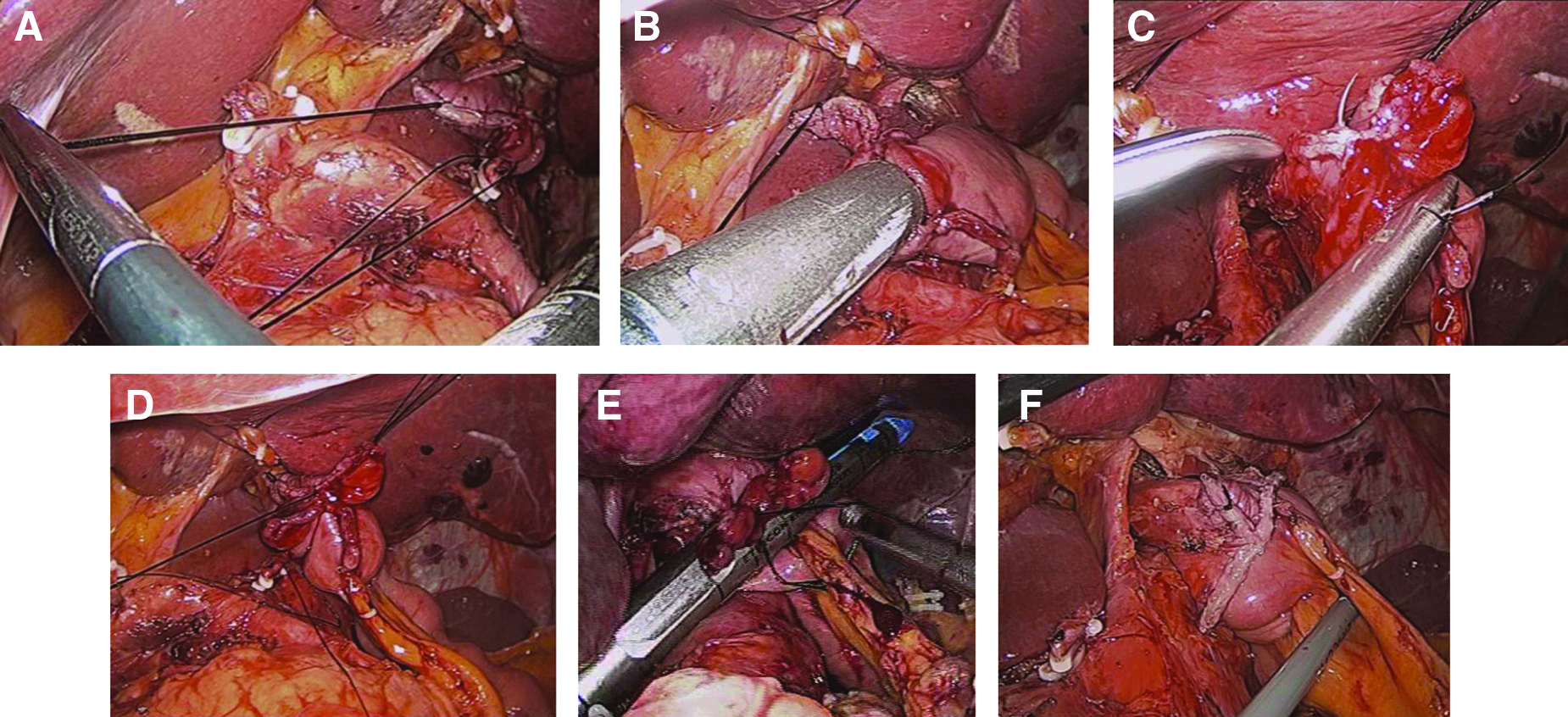
How to make an esophagojejunostomy.
To make an esophagojejunostomy, two sutures were retracted during the reconstruction. The first assistant retracted the first suture in the direction of the operator inside the abdominal cavity (Fig. 4A), and the second assistant retracted the second suture through the right lower trocar outside the abdomen (Fig. 5). This procedure is important for preventing the slippage of the esophageal stump into the thoracic cavity; it also guides the introduction of the anvil of the endoscopic linear stapler into the small esophagostomy of the esophageal stump during reconstruction of the eophagojejunostomy. An endoscopic linear stapler was inserted by the operator between the esophagostomy and enterostomy of jejunum to make an esophagojejunostomy (Fig. 4B). At this time, it is important and difficult to avoid insertion of the endoscopic linear stapler into a “pseudo” lumen, which is made artificially between the submucosal and muscular layers. After an esophagojejunostomy was constructed, the entry hole was closed with three sutures for tissue approximation (Fig. 4C and D) and then was finally closed by using a laparoscopic linear stapler (Echelon Flex 60) (Fig. 4E); in some cases, further suturing was necessary to complete the closure. Then, to construct the jejunojejunostomy, two small enterostomies of the jejunum are made: (1) on the anti-mesenteric side of the jejunum, 40 cm below the esophagojejunostomy (Fig. 6A) and (2) on the anti-mesenteric side of the afferent loop (Fig. 6B). The endoscopic linear stapler (Echelon Flex 60) was inserted into these enterostomies of the jejunum to construct a jejunojejunostomy, and the entry hole was closed with the endoscopic linear stapler (Echelon Flex 60) (Fig. 6C and D).

To make an esophagojejunostomy, two sutured threads were retracted during the reconstruction. The second assistant retracted the second suture through the right lower trocar outside the abdomen.
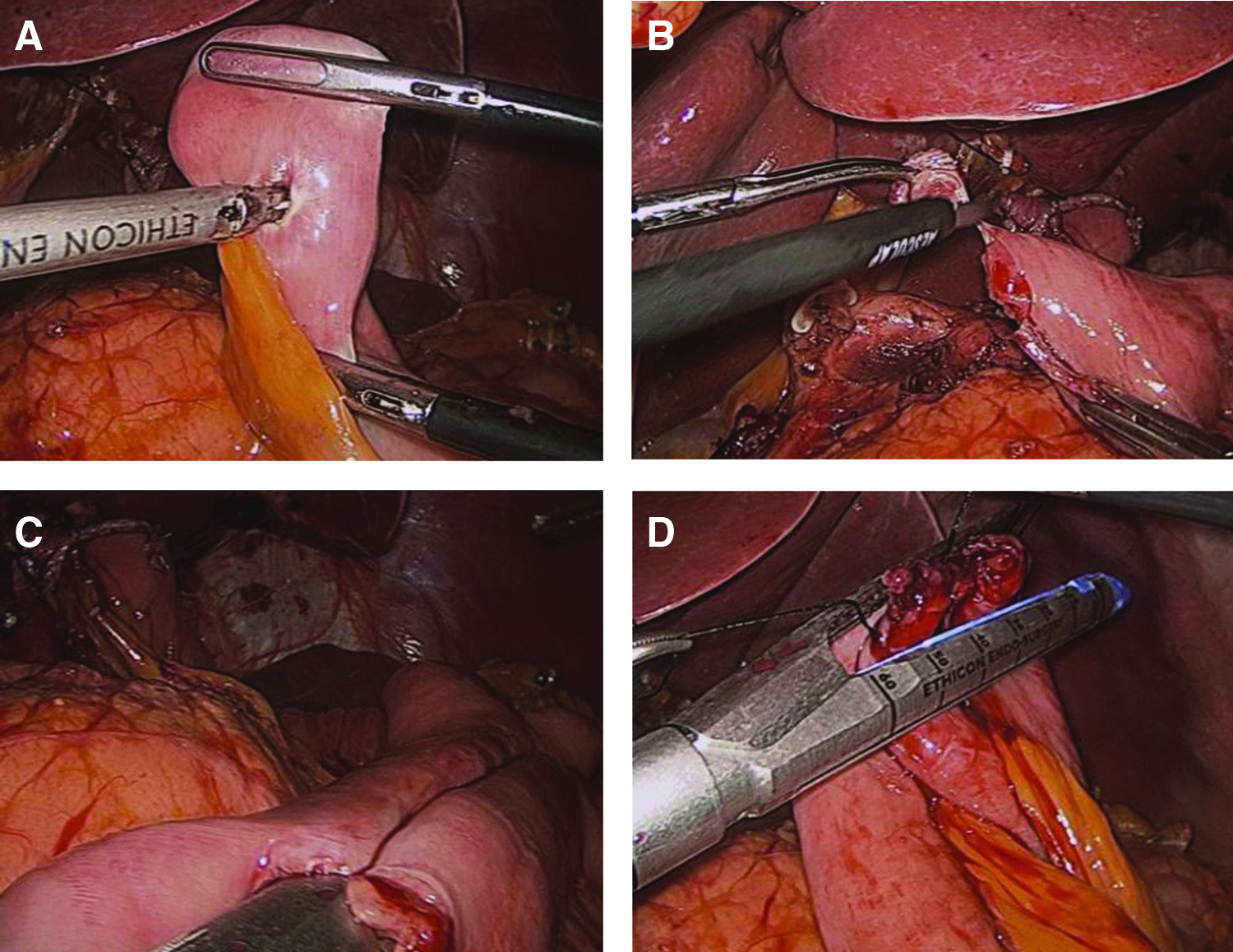
How to make a jejunojejunostomy. To reconstruct the jejunojejunostomy, two small enterostomies of the jejunum are made:
Finally, the mesenteric and the Peterson defects were sutured, and the operation was completed.
Clinical analysis of surgical outcomes of TLTG
The clinical data that were obtained from medical records were patient age, gender, body mass index, and American Society of Anesthesiologists score. Obesity was defined according to the World Health Organization Asia-Pacific Obesity classification, as normal weight (body mass index [BMI] 18.5 to 24.9 kg/m2), overweight (BMI 25.0 to 29.9 kg/m2), and obese patients (BMI≥30 kg/m2).17,18 The early surgical outcomes that were recorded were operation time, intraoperative events, overall postoperative complications, severe postoperative complications, time to first flatus, time to commencement of soft diet, administration of analgesics, and postoperative length of hospital stay. Pathological results that were analyzed were tumor size, number of retrieved lymph nodes, resection margins, and cancer stage according to the American Joint Committee on Cancer–International Union for Cancer Control, 6th edition. 19
The early surgical outcomes of the first 70 cases were compared with those of the subsequent 54 cases. This cutoff reflects the fact that after the 70th case, we instituted several devised technical improvements.
A postoperative complication was defined as any that required conservative or surgical treatment. Severe postoperative complications were defined as those requiring management by an endoscopic or interventional procedure or a re-operation without general anesthesia. 20
Postoperative pain control consisted of intravenous, patient-controlled analgesia (fentanyl [2,500 μg], ketorolac tromethamine [180 mg], and ondansetron hydrochloride [16 mg]). The degree of postoperative pain was assessed by a numerical rating scale and by the number of additional doses of analgesics required until discharge from the hospital.
Postoperative management
A diatrizoate meglumine and diatrizoate sodium (Gastrografin®; Bayer Schering Pharma AG, Berlin-Wedding, Germany) study was performed to evaluated leakage on postoperative Day 3 (Fig. 7A). The time to commencement of a soft diet was the day on which the patient felt comfortable enough to eat soft foods. Patients were discharged when they had no problems eating a soft diet, were generally comfortable, and demonstrated an absence of inflammatory conditions, including leukocytosis, unstable vital signs, and abrupt onset of abdominal pain. The final decision about discharge was made by the patient.
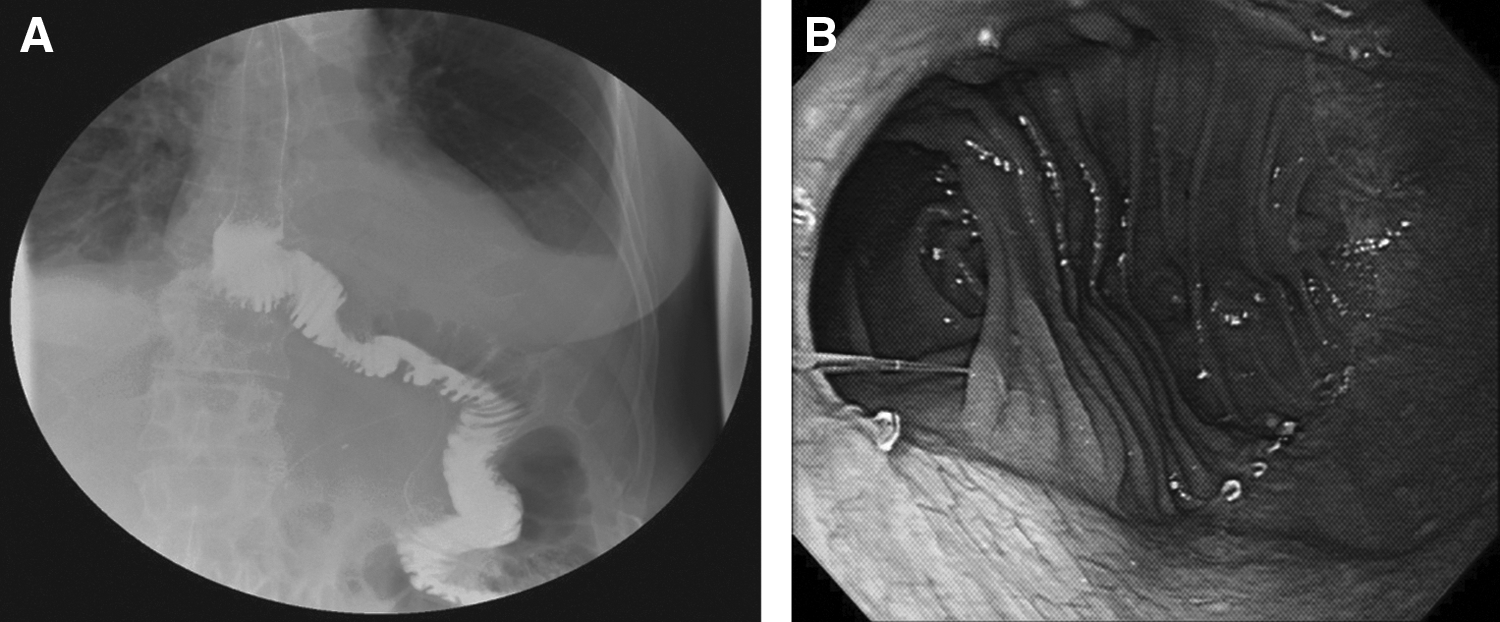
Postoperative Gastrografin and endoscopy study.
Statistical analysis
Statistical analyses were performed by using SPSS version 17.0 for Windows (SPSS, Inc., Chicago, IL). All data are expressed as mean±standard deviation values. Categorical variables were analyzed by using the chi-squared test and Fisher's exact test, and continuous variables were analyzed by using Student's t test. A value of P<.05 was considered statistically significant.
Results
Patient characteristics
The clinical characteristics of the 124 patients are presented in Table 1. The first 70 patients did not differ from the subsequent 54 patients in terms of clinical characteristics.
ASA, American Society of Anesthesiologists; BMI, body mass index; F, female; M, male; SD, standard deviation.
Early surgical outcomes
Table 2 shows the early surgical outcomes of the two groups. None of the patients required conversion to open surgery, and 30-day mortality was 0%. The first 70 cases were associated with a significantly longer mean operation time than the next 54 cases (189.0 versus 148.3 minutes, P<.001) as well as with more intraoperative events (P=.042), higher overall and severe postoperative complication rates (P=.003 and P=.030, respectively), longer times to commencement of soft diet (P=.027), and longer postoperative hospital stays (P=.017).
SD, standard deviation.
For intraoperative events during reconstruction of the anastomosis, there were 9 cases among the first 70 cases. Four cases were treated with more reinforcement of the esophagojejunal anastomosis line because slipping of the esophageal mucosa and submucosa occurred during reconstruction of the esophagojejunostomy. Three cases were treated by suturing on the injury site of the esophageal wall because of a vertical linear laceration of the esophageal wall during insertion of the endoscopic linear stapler into the small esophagostomy. Two cases were treated with more reinforcement of the jejunojejunostomy site because of jejunal serosa injury.
Among the subsequent 54 patients, an intraoperative event occurred in only 1 case; more resection of esophageal stump was performed to obtain an oncologically clear proximal resection margin, and therefore the esophageal stump was a little short to conclude the reconstruction of the esophagojejunostomy. So, it had a little tension between the esophagus and the efferent loop.
Table 3 shows the postoperative complications that occurred in the two groups. Among the first 70 cases, 11 patients (15.7%) had severe postoperative complications, including 4 with internal herniation, 2 with anastomotic leakage, 2 with anastomosis stricture, 1 with a duodenal stump leakage, 1 with extraluminal bleeding, and 1 with postoperative adhesive ileus. Of the 4 cases of internal herniation, in 1 case the patient had a diaphragmatic hernia, and another case was a Peterson herniation, both of which were managed by laparoscopic herniorrhaphy; the other 2 cases of internal herniation occurred through the mesenteric defect after a Roux-en-Y anastomosis and were resolved by themselves within 2 days. The 2 anastomotic leakage cases were managed by a combination of long-term parenteral nutrition and an interventional pig-tail catheter insertion with antibiotics. The 2 cases of anastomotic stricture of the esophagojejunostomy were managed by interventional balloon dilatation. The 1 patient with duodenal stump leakage was managed by a combination of laparoscopic tube duodenostomy insertion and conservative therapy. In the 1 case of extraluminal bleeding, the bleeding was stopped by ligation via laparoscopic suturing around the suprapancreatic area. Finally, the 1 patient with adhesive ileus was managed by laparoscopic adhesiolysis. Among the subsequent 54 patients, 2 patients (3.7%) had severe postoperative complications, including 1 with extraluminal bleeding and 1 with postoperative adhesive ileus. In the 1 case of extraluminal bleeding, the bleeding was managed by an interventional pig-tail catheter insertion with antibiotics for a large amount of hematoma. The 1 case with postoperative adhesive ileus was managed by laparoscopic adhesiolysis.
Table 4 presents the pathology findings of the two groups. They did not differ significantly in terms of tumor size (P=.287), the number of retrieved lymph nodes (P=.069), the proximal resection margin (P=.144), the distal resection margin (P=.272), the distribution of tumor depth (P=.128), or the presence of lymph node metastasis (P=.083).
AJCC/UICC, American Joint Committee on Cancer/International Union for Cancer Control; SD, standard deviation.
Fluorography demonstrated smooth passage of contrast medium through the anastomosis without leakage and stenosis (Fig. 7A). Postoperative endoscopy demonstrated a large anastomosis 6 months after the operation (Fig. 7B).
Discussion
Gastric cancer is one of the most common malignancies in Korea, and laparoscopic gastrectomy is more widely accepted for treating early gastric cancer. Recently, several types of totally laparoscopic gastrectomy using intracorporeal reconstruction were introduced. We have also reported on the benefits of totally laparoscopic distal gastrectomy with gastroduodenostomy using an endoscopic linear stapler.10,11 Although several articles have described TLTG using intracorporeal reconstruction, none has evaluated the early surgical outcomes of TLTG using endoscopic linear staplers.12,21,22 In terms of technical aspects, TLTG using endoscopic linear staplers is a difficult and complex procedure, which most surgeons are unable to perform. Indeed, TLTG can only be performed after accumulation of significant surgical experience in laparoscopic surgery; nevertheless, it still takes a long time to master the TLTG procedures. Thus, the present study describes our TLTG methods and how these methods changed as our experience grew. The hope is that this information will help other surgeons to master this technique more quickly and safely.
In our institution, the double stapling method using an EEA™ OrVil™ stapler (Covidien, Mansfield, MA) was not used because it is difficult to perform double stapling under the limited laparoscopic view, and then there is the possibility of injuring the esophagus while the OrVil is being inserted. In addition, this method needs a mini-laparotomy to divide the jejunum, insert the EEA into the jejunum, and make the jejunojejunostomy. Therefore, we reasoned that there would be no difference between this method and laparoscopic-assisted total gastrectomy using extracorporeal reconstruction in terms of early surgical outcomes. Regarding the lumen size of the esophagojejunal anastomosis, the lumen size is larger in the TLTG using an endoscopic linear stapler than in the double stapling method using the EEA OrVil (Fig. 7B). In addition, in our experiences of the subsequent 54 cases, there was no anastomotic stricture of the esophagojejunostomy.
Several investigators have reported that modified side-to-side anastomosis decreases postoperative complication rates.12,15,16 Clearly, this method can assure safe reconstruction because the uncut stomach enables the operator to retract the specimen and easily insert the endoscopic linear stapler, and the procedure is thus associated with a low rate of esophageal injury. However, this method cannot guarantee oncological safety during the reconstruction with regard to cancer cell spillage because this method created the esophagojejunal anastomosis before transection of the esophagus, so precise evaluation of the proximal resection margin of the esophagus was difficult. By contrast, in our TLTG method, the esophageal stump, which was established before the esophagojejunal anastomosis, was then transected with laparoscopic scissors after the remnant stomach was grasped with a laparoscopic intestinal clamp to avoid cancer cell spillage.
In practice, our experiences with intracorporeal esophagojejunostomy using an endoscopic linear stapler differed completely from our previous experiences with intracorporeal gastroduodenostomy. Soon after we started performing totally laparoscopic distal gastrectomy, we achieved satisfactory results without great difficulty because of our previous experiences. By contrast, when we started performing TLTG using an endoscopic linear stapler, the first 70 cases were highly problematic. Many intraoperative events occurred during the reconstruction process of anastomosis, such as anastomosis failure, in the first 70 cases. In particular, there were many events of vertical linear laceration of the esophagus by the endoscopic linear stapler. The esophageal lacerations arose because of imbalances between the pushing of the endoscopic linear stapler by the operator and the pulling of the esophagus and jejunum by the first assistant. In addition, in the first 70 cases of TLTG, the operator was required to make the reconstruction by first pulling the end of the stapled esophageal stump and the small gastrostomy of the esophageal stump with a laparoscopic grasper, after which the operator inserted an endoscopic linear stapler into the small esophagostomy and enterostomy of the jejunum. In this process, the operation field became very narrow, and in many cases the mucosa and submucosa of the esophagostomy slipped easily. Therefore, it was quite difficult to detect the true lumen of the esophagostomy, and this slippage of the esophageal stump decreased the size of the lumen of the esophagojejununal anastomosis. For these reasons, despite the skill of the participating assistants, it was difficult to make the esophagojejunostomy in TLTG by using an endoscopic linear stapler. Therefore, we had to devise several technical improvements that would help in reconstructing the esophagojejunostomy.
First, because the resected esophageal stump moves easily into the thoracic cavity, a wide operating field had to be obtained during the reconstruction to ensure the safety of the anastomosis. To prevent the slipping of the esophageal stump and to perform the anastomosis in the abdominal cavity, two intracorporeal sutures were performed: one at the end of the staple line and one at the small esophagostomy of the esophageal stump. The first suture was placed at the end of the stapled esophageal stump, and this suture was cut 15 cm from the esophageal stump, which was retracted by the first assistant during reconstruction of the esophagojejunostomy. The second suture was made at the small esophagostomy of the esophageal stump and was extracted outside the abdomen through the right lower trocar. To widen the operating field and prevent esophageal slipping during the reconstruction of the esophagojejunostomy, the first assistant pulled the first suture toward the operator in the abdominal cavity, while the second assistant pulled the second suture thread toward the operator's side from outside the abdominal cavity. This retraction meant that the operator could prevent the anastomosis from falling into the thoracic cavity while simultaneously confirming its safety. Furthermore, the operator was able to insert an endoscopic linear stapler without great difficulty between the esophagostomy and enterostomy of the jejunum to make an esophagojejunostomy. As a result, we were able to minimize the size of the remnant entry hole of the esophagojejunostomy, and, upon completion of the esophagojejunostomy, we could confirm the safety of both the posterior and anterior sides of the anastomosis (Fig. 4F).
Laparoscopic Roux-en-Y gastric bypass reportedly has a higher rate of postoperative internal herniation than open bypass surgery because of fewer adhesions.23,24 Recently, many authors prefer the anticolic route for the Roux limb, which reduces the potential sites for hernia from three to two, and close the mesenteric defect after a laparoscopic Roux-en-Y gastric bypass. In our early period of TLTG, 4 cases had an internal herniation after the operation because we did not close all of the defect. No patients in the later series had an internal herniation because of routine closure of all mesenteric defects using a laparoscopic locking clip. To prevent an iatrogenic diaphragmatic hernia, we avoided direct damage to the diaphragmatic tissue by an ultrasonic cutting and coagulation system (Harmonic® ACE™ curved shears; Ethicon) during dissection.
Our analysis of the early surgical outcomes of TLTG revealed that although the procedure was being performed by experts and a well-trained surgical team, the first 70 cases involved many intraoperative events and severe postoperative complications. However, the surgical outcomes of TLTG improved subsequently. It is possible that these improvements reflect not just our increased experience, but also the changes we made to the surgical procedure devised, which made it easier to perform the intracorporeal esophagojejunostomy.
In conclusion, with our TLTG method, we could obtain a wider operation field and effective retraction of the esophageal stump through this procedure. We strongly believe that TLTG using an endoscopic linear stapler may be one of the best ways to improve the early surgical outcomes of gastric cancer patients. However, surgeons who are inexperienced in laparoscopic gastrectomy should be careful when performing TLTG because this procedure involves many complex processes. We believe that this account of our early experiences with our TLTG method in a high-volume center can help surgeons to master this method faster and more safely.
Footnotes
Disclosure Statement
No competing financial interests exist.