
Abstract
Abstract
Background:
Gastric varices (GVs) are a common finding in Egyptian patients with portal hypertension due to cirrhosis or schistosomal hepatic fibrosis. These patients present with an acute attack or history of hematemesis. Endoscopic histoacryl injection is the standard treatment in Egypt; however, because of technical difficulties it is possible to inject only a little amount of this material, as it may endanger the channels of the flexible endoscope. We thought of a new surgical laparoendoscopic technique to obviate the need for repeated endoscopies and complete obliteration of GVs.
Patients and Methods:
This study was conducted on 20 patients with portal hypertension and GVs. After the patient was placed under general anesthesia, a small gastrostomy was done in the anterior gastric wall through which a 10-mm trocar was inserted for the laparoscopic camera. Injection of GVs was done via a spinal needle or a central venous line needle inserted directly. Injection of an adequate amount of histoacryl was done under direct vision.
Results:
This study was conducted from July 2009 to August 2011 on 20 patients with GVs. The age range was from 22 to 56 years, with a mean age of 39.8±7.85 years. There were 14 men (70%) and 6 women (30%). Fourteen patients (70%) showed complete obliteration of GVs after one session of treatment, whereas 6 patients (30%) had unsatisfactory results and were subjected to another session. GVs were completely obliterated after the second session in 4 patients. Two cases of recurrence of GVs were operated on.
Conclusions:
This new technique enabled us to inject GVs with a suitable amount of glue material under direct vision without harming the endoscope. Use of this procedure is recommended in patients fit for surgery and those who had failed endoscopic injection sclerotherapy.
Introduction
There are different classifications of GVs. 5 A simple approach proposed by Sarin et al. 6 classified GVs into gastroesophageal varices (GEVs) and isolated GVs (IGVs). GEVs are associated with EVs and extend for 2–5 cm beyond the gastroesophageal junction. This type can be divided into GEV1 (the most common type, 74% of all GVs), extending along the lesser curvature, and GEV2 (second most common type, 16% of GVs), which run in the direction of the cardia. IGVs occur independent of EVs and are subdivided into IGV1, extending along the fundus of the stomach (fundic varices, 8%), and IGV2, which occur anywhere in the stomach, including the body, antrum, pylorus, and duodenum (2%).
Bleeding is the most important clinical presentation in GV patients. Hosking and Johnson 7 reported that the variceal size and red spot appearance on endoscopy and Child's score were the predictive factors for bleeding from gastric fundal varices.
Various techniques, using endoscopy, surgery, and interventional radiology, are available for the treatment of GVs. Endoscopy is an effective tool for attaining hemostasis in the majority of emergency bleeding cases, even if the effects are not always sufficient as a curative treatment method. Current research has proved that the use of cyanoacrylate glue (histoacryl glue) is the first line in management options for GVs. 8
The aim of this work was to assess the role of transgastric laparoscopic injection of histoacryl glue in the management of GVs in patients with portal hypertension.
Patients and Methods
Subjects
Twenty patients with clinical, laboratory, and endoscopic evidence of portal hypertension with GVs were enrolled in the trial. This prospective study was done in the Gastrointestinal Surgery Unit, Main Alexandria University Hospital, Faculty of Medicine, Alexandria University, Alexandria, Egypt. This study approved by the Research Ethics Committee of the Hospital, and informed consent was obtained from all patients.
All patients were subjected to full history taking, general and local abdominal examination, and routine laboratory investigations (complete blood count with emphasis on platelet count and hemoglobin value, liver functions [alanine aminotransferase, aspartate aminotransferase, serum albumin, prothrombin time and activity, and serum bilirubin], renal function tests [urea and creatinine], fasting blood sugar, and hepatitis markers). Imaging included abdominal ultrasonography and triphasic computerized tomography of the abdomen.
Upper gastrointestinal endoscopy was performed to detect the site and number of varices and to detect if there were GVs only or in combination with EVs. We performed upper endoscopy with an Olympus GIF-30 gastroscope. Two units of blood were reserved for each patient before surgery.
Inclusion criteria
All patients with GVs, either GEV or IGV, age between 20 and 60 years, who had failed obliteration of GVs by endoscopic methods (patients subjected to three to five sessions of endoscopic injection of histoacryl), hemodynamic stability, and fitness for anesthesia and patients with a Child–Pugh classification of A or B were enrolled.
Exclusion criteria
Patients with active bleeding from GVs (until control by other methods such as tamponade or endoscopic treatment), patients with hepatocellular carcinoma or active hepatitis, hemodynamically unstable patients who were unfit for anesthesia, and patients with a Child–Pugh classification of C were excluded.
Procedure
Preoperative preparation using propranolol (Inderal®; Wyeth) (40 mg/day for 1 month before the procedure) was done to decrease the variceal pressure. The same drug was also given postoperatively.
After premedication with fentanyl, induction of anesthesia was carried out using propofol, cisatracurium, intermittent positive pressure ventilation, and endotracheal intubation. Anesthesia was maintained using sevoflurane and controlled mechanical ventilation. The end of the viewing endoscope was passed from the mouth across the esophagus and then to the stomach. Air was insufflated in the stomach so the anterior gastric wall came in direct contact with the anterior abdominal wall. Abdominal incision was done in the left hypochondrium, guided directly over the illumination of the endoscope, about 4 cm from the midline, midway between the left costal margin and the umbilicus. The length of the incision was about 3 cm, oriented transversely; the incision went through the skin, subcutaneous tissue, anterior rectus sheath, and the rectus muscle until the peritoneum was reached and opened. The stomach was identified, again by the light of the endoscope. A purse-string suture in the anterior gastric wall was done using Vicryl® (Ethicon) 2-0 suture on a rounded needle. A small (10-mm) incision was done with a scalpel or diathermy in the anterior gastric wall inside the purse-string suture, through which a 10-mm trocar was introduced into the stomach and connected to CO2 gas insufflators, and then the upper gastrointestinal endoscope was withdrawn. The laparoscopic camera was passed through the trocar, and CO2 was insufflated to visualize the GVs. A long spinal needle (22 gauge) or central venous line needle (7 French) was passed directly through the anterior abdominal wall in the most accessible point to the varices, guided by the laparoscopic camera to reach the varices, and injection of the prepared histoacryl glue was done under direct laparoscopic vision.
Up to 10 ampules of histoacryl dissolved in 20 mL of lipidol (each ampule of histoacryl was dissolved in a double amount of lipidol) were injected. Usually the injection was done intravariceally, at the end of the injection; bleeding was checked and dealt with if it occurred by more injection of histoacryl (Figs. 1–5).
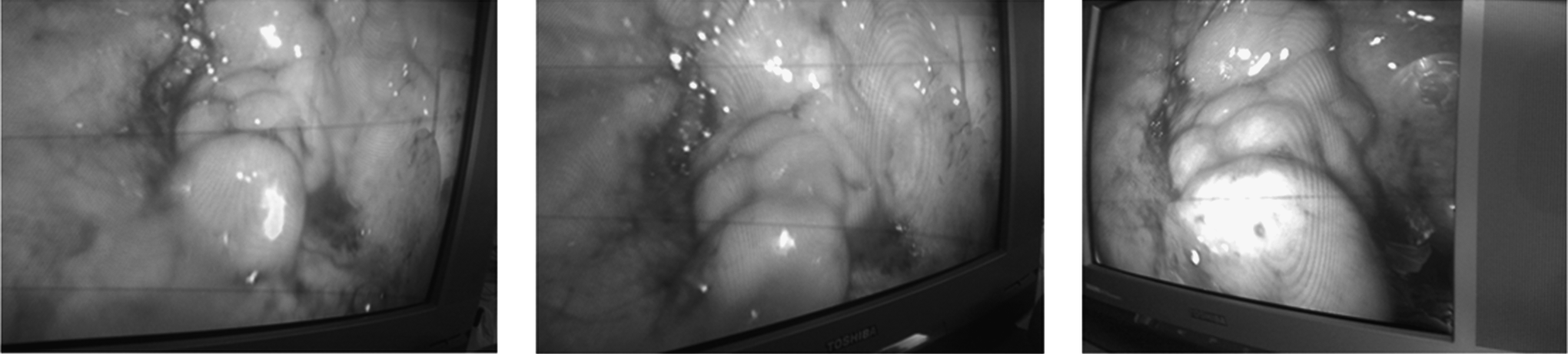
Intraoperative laparoscopic view of gastric varices (gastroesophageal varice type 2).
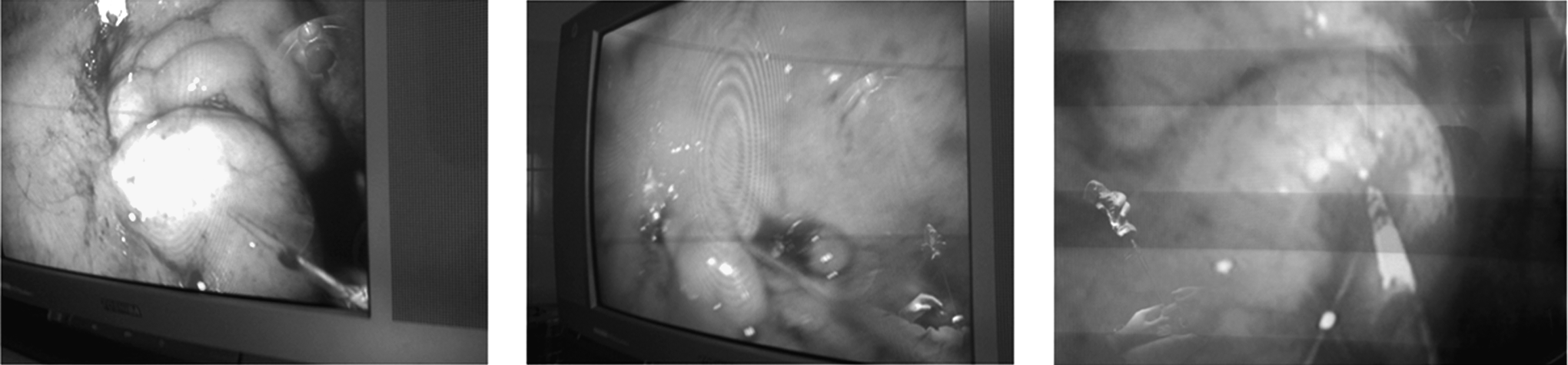
Intraoperative laparoscopic direct variceal injection by histoacryl via a spinal needle (gastroesophageal varice type 2).
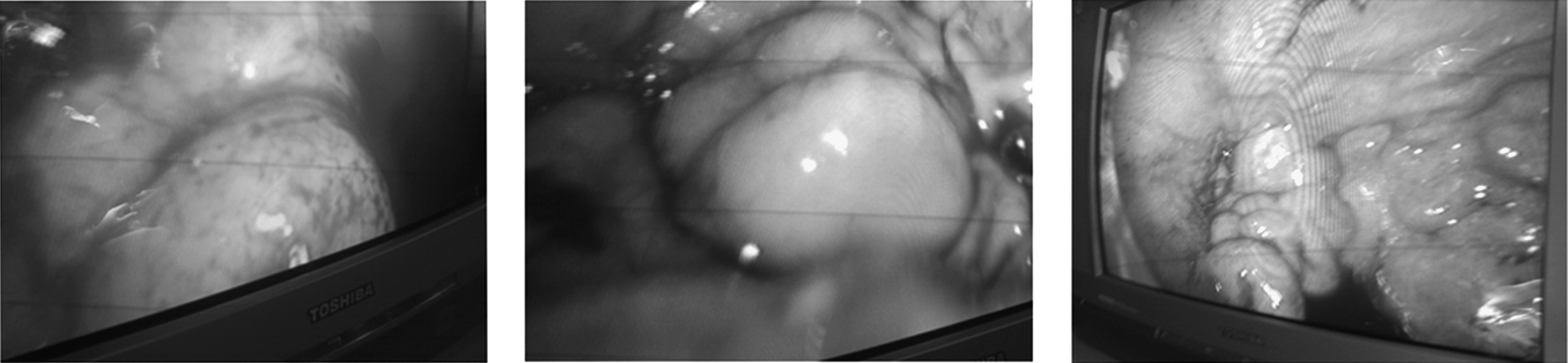
Laparoscopic view of gastric varices after histoacryl injection (gastroesophageal varice type 2).
Laparoscopic view of gastric varices after histoacryl injection (gastroesophageal varice type 1).
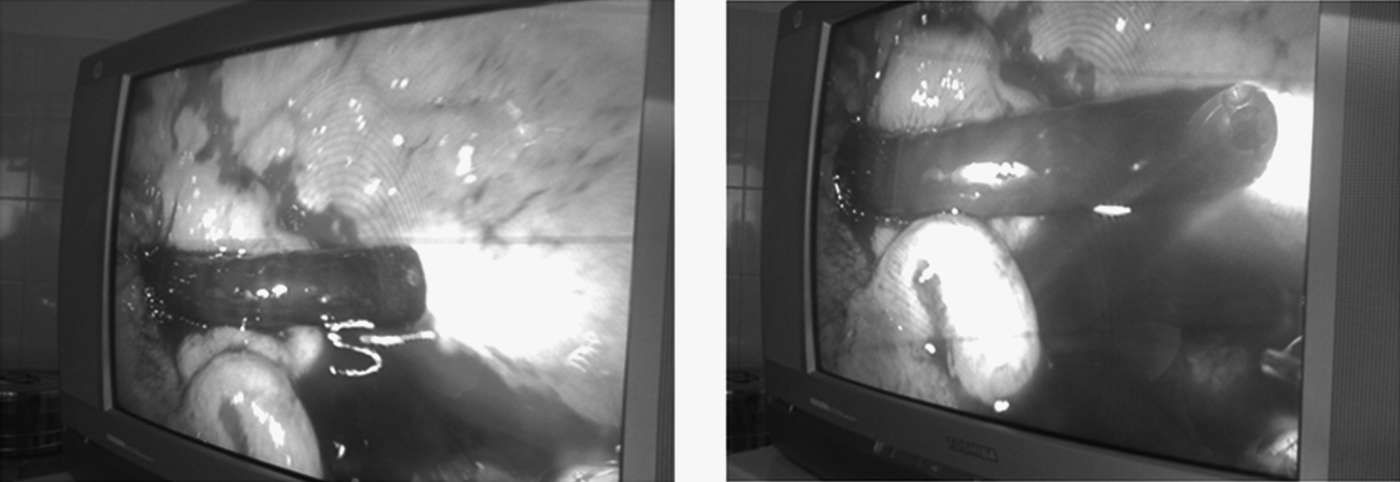
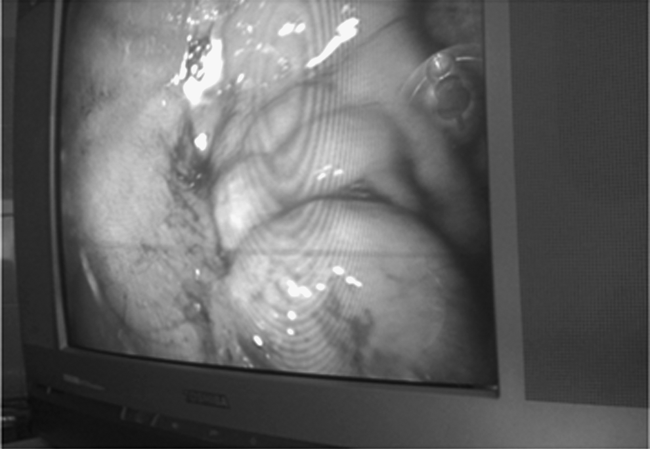
Laparoendoscopic view of gastric varices after histoacryl injection (gastroesophageal varice type 1). The endoscope is showen retroflected to the fundus.
The laparoscope was withdrawn under direct vision, and the purse-string stitch of the anterior gastric wall was closed. The purse-string suture was supported by additional two seromuscular sutures of Vicryl 2-0 on a rounded needle. A tube drain was put in the peritoneal cavity for drainage of any leakage of gastric content if present. Gastroscopy was done after injection for visualization of varices and looking for any postinjection bleeding. If there was no bleeding, the endoscope was withdrawn after aspiration of all the injected air and CO2 or leaked blood if present, and a nasogastric tube was inserted to continue drainage and for detection of rebleeding if present. Any associated EVs were injected with ethanolamine oleate or banded with a rubber band endoscopically at another session to avoid morbidity of these patients. The peritoneum, anterior rectus sheath, subcutaneous tissue, and skin were closed.
Follow-up
Early follow-up
During the postoperative period until patients were discharged from the hospital, extending into the first 5 days postoperatively, vital signs were measured regularly, the wound was dressed if needed, postoperative bleeding if it occurred was dealt with, and oral feeding was started after 3–5 days postoperatively.
Late follow-up
At intervals of 6 weeks, 3 months, 6 months, and 1 year, upper gastrointestinal endoscopy was done to follow the progression of the condition of GVs.
Results
This study was conducted from July 2009 to August 2011 on 20 patients with GVs, subjected to laparoendoscopic transgastric injection sclerotherapy using histoacryl glue to achieve complete variceal obliteration. The age range was from 23 to 55 years. Demographic data are given in Table 1.
Clinical presentation of the 20 patients included presentation with a history of upper gastrointestinal bleeding by 16 patients (80%) and admission with active upper gastrointestinal bleeding by 4 patients (20%), in whom the bleeding was controlled medically before they were subjected to the procedure. Fourteen patients (70%) had splenomegaly secondary to portal hypertension, and 3 patients (15%) presented with hepatic jaundice. Preoperative thrombocytopenia was detected in 4 cases (20%); platelet levels were 30,000, 35,000, 60,000, and 72,000/mm3. These cases were managed by platelet transfusion intraoperatively to avoid bleeding. Two of them had recurrent bleeding after the first session and were operated on after the second session (due to non-obliteration of GVs).
With regard to Child–Pugh classification (of the studied group patients), 8 cases (40%) were Child A, while 12 patients (60%) were Child B. The preoperative endoscopic examination revealed that 55% were GEV type 1 and 20% were GEV type 2, while 25% had IGV type 1. All cases showed risk signs of bleeding. In the 15 patients with GEVs, 86.7% of patients with EVs were treated by variceal band ligation (Table 2).
EVs, esophageal varices; GEVs, gastroesophageal varices; IGV, isolated gastroesophageal varice.
Patients in this study group were previously subjected to multiple (three to five) sessions of endoscopic injection of GVs with histoacryl at intervals from 3 weeks to 5 months between sessions, in order to obliterate the GV before laparoscopic injection (Table 3).
The operative time ranged from 25 to 50 minutes (mean, 35 minutes). The blood loss was so minimal that no patient needed operative blood transfusion.
Fourteen patients (70%) showed complete obliteration of GVs after one session of transgastric laparoscopic injection sclerotherapy, while 6 patients (30%) had unsatisfactory results and were subjected to another session 3 months later (2 of them had rebleeding between the first and second sessions). In 4 patients in the latter group, GVs were completely obliterated after the second session; in the other 2 cases, GVs showed no response, and the patients were subsequently subjected to a splenectomy–devascularization operation after 3 months from the second session (Table 4).
Postoperative complications
Complications occurred in the 6 cases (30%) subjected to the second session of transgastric laparoscopic injection sclerotherapy. Recurrence of GVs occurred in the 6 patients after the first session, with immediate postoperative bleeding from GVs occurring in 2 cases (10%); their ages were 48 and 53 years, their varices were of large size, and they had had preoperative thrombocytopenia. Rebleeding cases were controlled by mechanical tamponade by the insertion of a Minnesota tube and medical treatment. Failure to obliterate GVs after the second session in these 2 cases was an indication for surgery (decongestion splenectomy). There was no evidence of gastric leak or wound infection. The hospital stay ranged from 2 to 6 days postoperatively (mean, 3.7 days).
Discussion
GVs occur in about 20% of patients with portal hypertension. Although bleeding from GVs occurs less frequently than from EVs, the former is more severe and more difficult to treat. There are multiple treatment options for GVs, including placement of a Sengustakian–Blackmore tube, endoscopic sclerotherapy, performing transjugular intrahepatic portosystemic shunt, and balloon-occluded retrograde transvenous obliteration (B-RTO). 9
However, B-RTO is only possible in the presence of a splenorenal shunt. 9 A transjugular intrahepatic portosystemic shunt should mainly be used if there is a chance for liver transplantation. 10 Of the available endoscopic options, injection of N-butyl-2-cyanoacrylate sclerotherapy is highly effective for the obliteration and treatment of GVs and variceal bleeding. Surgical treatment is also available for management of GVs, either a shunt procedure or a devascularization–splenectomy procedure. So no single method is accepted as the ideal treatment of GVs.
The present study was done on 20 patients to evaluate the role of transgastric laparoscopic histoacryl injection in the treatment of GVs. There were 16 men (80%) and 4 women (20%). The age range was from 23 to 55 years, with a mean age of 38.9±7.55 years.
In the present study all patients suffered from hepatitis C, 3 of them presented with jaundice (15%), 14 patients had splenomegaly (70%), 16 patients (80%) had been subjected to routine endoscopic evaluation after previous episodes of upper gastrointestinal bleeding, and 4 patients (20%) presented with acute attacks of bleeding managed as emergency cases and then were enrolled in our study. With regard to hepatic function according to Child classification, 8 patients were Child classification A (40%), and 12 patients were Child classification B (60%). Patients of Child classification C were not enrolled in our study for surgical and anesthetic causes.
In the study of Sarwar et al., 11 76 patients (93.8%) suffered from cirrhosis due to hepatitis C, 2 patients (2.5%) had hepatitis B, and the cause of cirrhosis was not known in 3 patients (3.7%). The mean Child–Pugh score was 6.45±1.31, 44 patients (54.3%) belonged to Child classification A, 33 patients (43.2%) belonged to Child classification B, and 2 patients (2.5%) belonged to Child classification C. Secondary prophylaxis was the reason for follow-up in 47 patients, whereas 7 patients (8.65%) were brought to the endoscopy unit after an acute episode of upper gstrointestinal bleeding.
In the present study, 11 cases (55%) were GEV type 1, and 4 cases (20%) were GEV type 2, whereas 5 cases (25%) were IGV type 1 on first endoscopic examination. All these patients were subjected to endoscopic sessions of sclerotherapy before laparoscopic histoacryl injection. The number of endoscopic sclerotherapy sessions ranged from three to five (mean, 4.45 sessions), and failure of endoscopic management obligated us to use laparoscopic injection of histoacryl as a large amount of sclerosant material could be injected in well-visualized varices. In the 15 patients with GEVs, the EVs were treated by band ligation in 13 patients and by injection sclerotherapy in 2 patients.
Cheng et al. 12 showed that on endoscopic examination, GVs were composed of GVs accompanied by EVs in 495 patients (80.8%) and solitary GVs (fundal varices) in 118 patients (19.2%).
In the present study, histoacryl injection was done laparoscopically for GV obliteration in the 20 patients. Patients in the studied group were subjected to multiple sessions of injection with a mean of 1.2 sessions with amount of histoacryl ranging from 10 to 15 mL in a lipidol texture according to the size of varices: 14 patients (60%) were subjected to one session of injection, and 6 patients (30%) were subjected to two sessions. Complete obliteration of GVs occurred in 18 (90%) patients after the duration of follow-up, and failure to obliterate GVs occurred in 2 patients of the studied group, who were then subjected to decongestion splenectomy after 3 months from the second session.
In the study of Alsherbiny et al., 13 a comparative study among GV obliteration by histoacryl injection (45 patients), GV sclerotherapy by alcohol injection (30 patients), and GV band ligation (40 patients) was done in 115 patients. Successful variceal obliteration wasachieved in 43/45 patients in Group I (95.6%), 14/30 patients in Group II (46.7%), and 14/40 patients in Group III (35%).
In the study done by Cheng et al. 12 for evaluation of endoscopic sclerotherapy of GVs using butyl-cyanoacrylate on 635 patients, 146 of them were managed on an emergency basis with bleeding GVs, and 489 patients were managed as scheduled. A success rate of hemostasis was achieved in 134 out of the 146 cases of emergency butyl-cyanoacrylate injection with a hemostatic rate of 95.2%. After injection of butyl-cyanoacrylate the vessel was immediately occluded. Follow-up was scheduled at 1 week, 1 month, 3 months, 6 months, 12 months, and 24 months after sclerotherapy. On follow-up, complete obliteration of varices occurred in 387 patients (76.9%), partial disappearance of varices occurred in 87 patients (17.3%), and patent remnant varices in 24 patients (5.8%) were observed between 1 month and 12 months after the treatment. Of the 24 patients who had remnant varices, 20 of them received a second butyl-cyanoacrylate injection, and 1 case received a third injection. Nine of 118 cases of IGVs showed appearance of EVs during the follow-up period, and of these, 2 cases were treated with sclerotherapy, 2 cases with band ligation, and 1 case with surgery. Recurrence of GVs was noted after the mentioned outcome had been observed. The number of recurrent cases was 18, 14, 4, 0, and 1 at 1, 2, 3, 4, and 5 years, respectively, after the treatment.
In the study done by Katoh et al. 14 the role of B-RTO for the treatment of GV was evaluated in patients who had GVs and splenorenal shunt (47 patients). In 37 cases, the technique was successful, and complete thrombosis of varices was observed on enhanced computerized tomography. Among those 37 cases, 3 were lost to follow-up, and 2 died soon after the procedure; the remaining 32 cases were followed up for detecting the recurrence of GVs and progression to EV if progression occurred. During the median follow-up period of 746 days (range, 134–136 days), GVs recurred in 2 patients (one appeared after 13 months and the other after 28 months), so the overall cumulative relapse-free rate was 90% at 3 and 5 years of follow-up after the first B-RTO. The 2 patients who had recurrence of GVs were subjected to another B-RTO procedure, and complete thrombosis of the GV and gastrorenal shunt was achieved. In the 3 cases in which GV recurred after emergency endoscopic sclerotherapy by histoacryl, the gastrorenal shunt remained patent, and residual GV appeared occluded during B-RTO.
Hasahizume et al. 15 used gastric devascularization and splenectomy in treatment of GVs in 42 patients with IGVs. GVs were eradicated in all 42 patients. Survival rate was 77.6% after 1 year, 88.1% after 3 years, and 76.5% after 5 years (mean follow-up period was 46 months).
In the present study, propranolol at 40 mg/day was used for 1 month before and after the procedure. Complete eradication of GVs occurred in 18 patients (90%) of the studied group, and 2 cases were subjected to surgery because of no response even after the additional session. No patient died during the follow-up period. So this novel method achieved a 90% success rate with complete eradication of GVs. With regard to EVs, although they were seen by upper gastrointestinal endoscopy, we preferred not to tackle them during the procedure to avoid more morbidity of these fragile patients, and these results are comparable to the international results achieved and published by Sarin 2 and Wantable et al. 16 using conventional endoscopic methods.
Pharmacological treatment might be effective in control of bleeding from GEV type 1 according to Sarin's classification. GEV type 2 and IGV type 1 are mostly associated with major portosystemic shunt, so portal vein pressure is lower in these patients than in patients with EVs. As a result, the efficacy of conventional drugs such as vasodilators or vasoconstrictors is doubtful in the management of GVs because of the hyperdynamic state and presence of a major portosystemic shunt. 17 Mishra et al. 17 examined a beta-blocker on secondary prophylaxis of GV rebleeding. In this study, a beta-blocker or terlipressin was shown to be inferior to endoscopic cyanoacrylate injection therapy.
Complications encountered during the study were in the form of rebleeding (2 patients [10%]). These 2 cases had massive varices, occupying most of the cardiac region; they engulfed all the histoacryl injected. They were managed conservatively by blood transfusion and tamponading then by another modality of treatment. A 10% rebleeding rate of cases is better than that for other conventional methods. Failure of obliteration of GV after the second session in these 2 cases was an indication for surgery.
In the study done by Alsherbiny et al., 13 the complications encountered during the study were rebleeding (28%), ulceration of the GV (24%), dysphagia (12%), and chest pain (12%). These complications were fewer in patients subjected to GV obliteration by histoacryl injection (20%) than the second group who were subjected to alcoholic sclerotherapy (37%) and the third group who were subjected to endoscopic band ligation (30%).
This technique is a promising way to treat GVs and needs to be experienced on a wide scale of patients to be sure about its effectiveness and safety. It gives a direct vision of the GV with easy injection with no harmful effect on the scope. But, after all, it is a surgery that is subject to the hazards of anesthesia and general complications of surgery. It can be done in cases of failure of endoscopic injection of GVs.
Conclusions and Recommendations
Laparoscopic transgastric injection can be tried after failure of conventional endoscopic methods. This new technique enables us to inject a large amount of glue material (histoacryl) under direct vision and gives direct access to varices without harming the endoscope. This technique achieved a high success rate in the management of GVs with a low rate of complications, so its use is recommended to gain experience with a wide variety of patients, especially patients fit for surgery and patients who had failed endoscopic injection sclerotherapy.
Footnotes
Disclosure Statement
No competing financial interests exist.