
Abstract
Abstract
Objectives:
Brunner's adenoma is a rare benign tumor of the duodenum. The traditional management option was close follow-up and surgical tumor resection. With the development of endoscopy devices and techniques, endoscopic resection is considered an alternative treatment option. However, whether small lesions require treatment has been controversial. We planned to study the feasibility, efficacy, and safety of endoscopic resection for the treatment of Brunner's adenomas.
Subjects and Methods:
In total, 30 Brunner's adenomas from 29 patients were treated with endoscopic resection between August 2007 and June 2011 in our hospital. Endoscopic ultrasonography (EUS) was performed preoperatively to evaluate tumor origin and size. Tumor characteristics, complications, en bloc resection rate, and local recurrence rates were evaluated.
Results:
Of the 29 patients, 13 (44.8%) were men. The median age was 55 years (range, 29–72 years). The mean maximal dimension of the lesions was 1.7±0.1 cm (range, 0.6–7 cm). Overall, 9 lesions were treated with snare resection, 12 lesions were treated with conventional endoscopic mucosal resection (EMR), and 9 lesions were treated with endoscopic submucosal dissection (ESD). Only 1 case of delayed bleeding occurred on Day 2 after EMR. The en bloc resection rate was 100% (30/30). One lesion resected by EMR exhibited indeterminate tumor margins. The overall curative resection rate was 96.7% (29/30). During the follow-up period (median time, 13 months; range, 2–39 months), 1 patient, whose tumor exhibited indeterminate margins, showed recurrence 1 year after EMR; ESD was recommended. No recurrence was observed during the subsequent follow-up period.
Conclusions:
Our study provides evidence of the efficacy of endoscopic resection for the localized treatment of duodenal Brunner's gland adenomas with relatively few complications and a low mortality rate.
Introduction
Subjects and Methods
We retrospectively analyzed our database of patients who underwent endoscopic treatment for duodenal lesions at the Endoscopic Center of Zhongshan Hospital between August 2007 and June 2011. In total, 30 Brunner's adenomas from 29 patients were included in this study. Endoscopic ultrasonography (EUS) was performed preoperatively with a UM-2000 system (Olympus, Tokyo, Japan) to evaluate tumor origin and size (Fig. 1A and B). Tumor characteristics, complications, en bloc resection, and local recurrence were evaluated in all patients. Informed consent was obtained from each patient. This study was approved by the Institutional Review Board of Zhongshan Hospital.

Different endoscopic and ultrasonographic endoscopic manifestations of duodenal Brunner's adenomas:
Standard single accessory-channel endoscopes (GIT-H260; Olympus) and/or dual-channel endoscopes (GIF-2T240; Olympus) were used during the procedures. A short, transparent cap (ND-201-11802; Olympus) was attached to the tip of the gastroscope to provide a constant endoscopic view and to apply tension to the connective tissues during dissection. An insulated-tip (IT) knife (KD-611 L; Olympus) and a hook knife (KD-620 LR; Olympus) were used during endoscopic submucosal dissection (ESD) procedures. The Erbe HybridKnife® system (ICC 200; Erbe, Tübingen, Germany) was used as a high-frequency generator. The following endoscopic resection treatment options were utilized: snare resection (SR), endoscopic mucosal resection (EMR), and ESD.
SR procedures
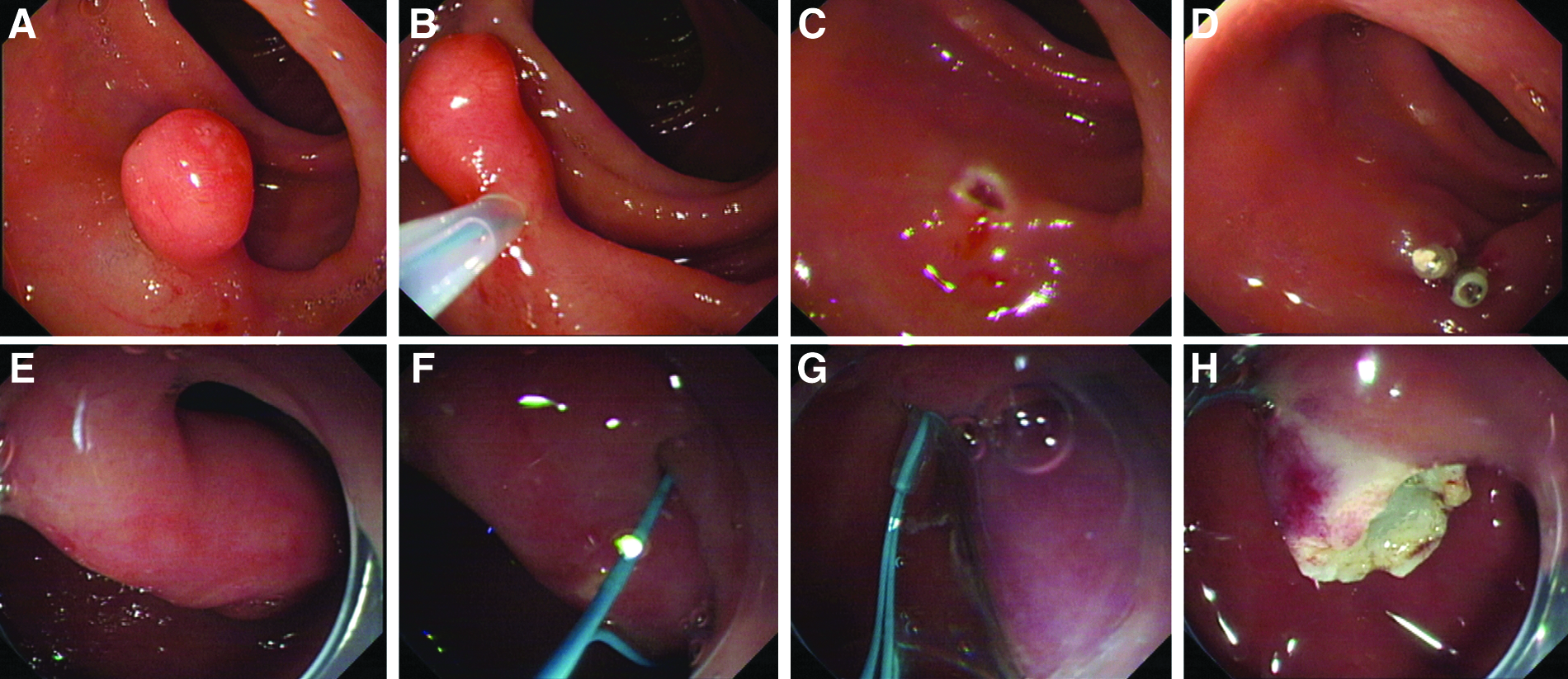
SR procedures were performed using a snare, which was used to encircle and lift up duodenal lesions. Subsequently, cauterization on coagulation mode was applied to the base of the lesion for lesion removal. 5 If the Brunner's adenomas were polyps with long pedicles, SR should follow nylon rope ligature (Fig. 2E–H).
Duodenal Brunner's adenoma
EMR procedures
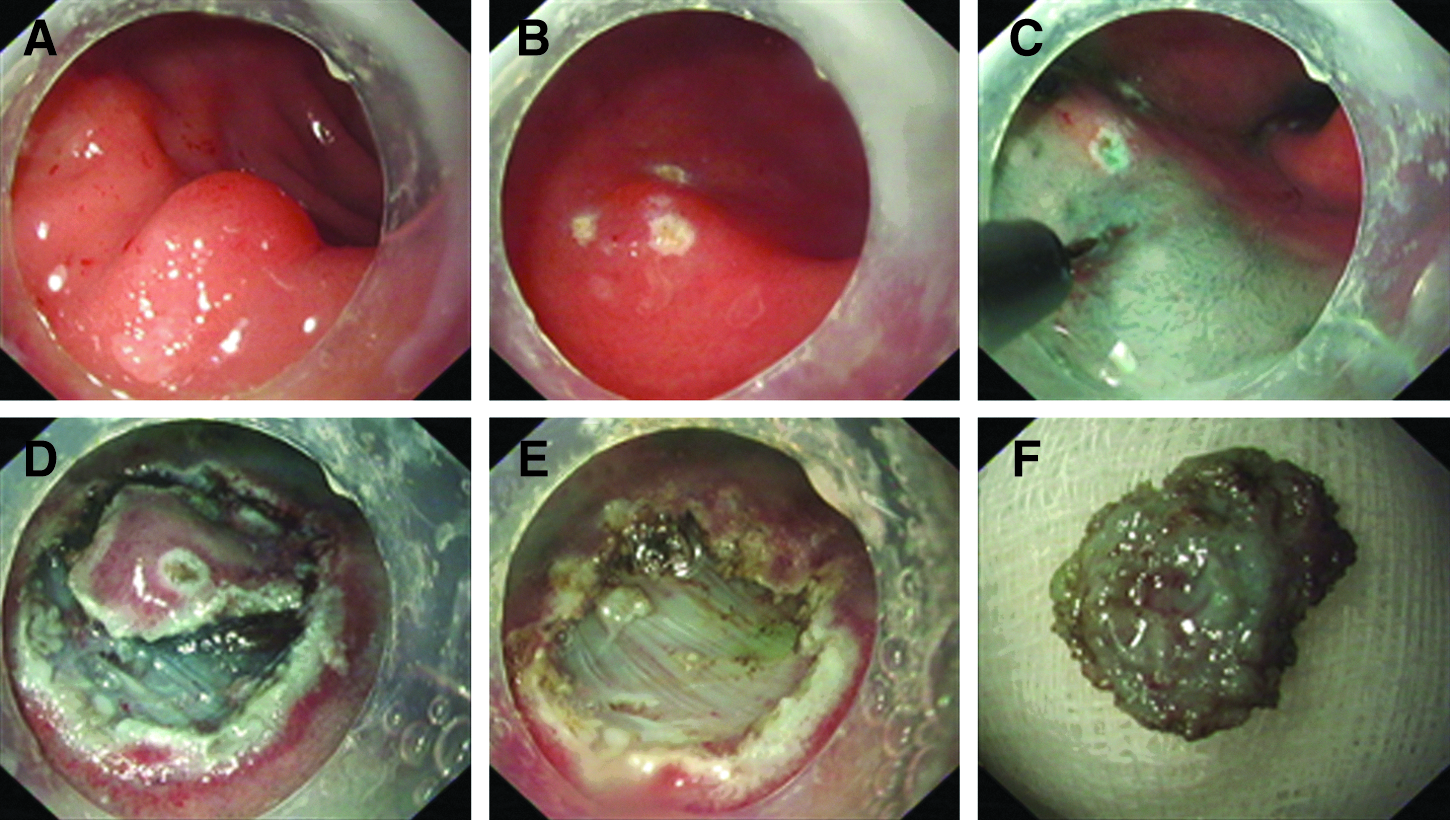
EMR was performed using a snare after saline was injected into the submucosal layer. Blended current was used for resection. After EMR, the resected space was examined carefully to determine if any residual tumor was left. If any residual tumor was observed, additional EMR, hot biopsy, heater probe, or argon plasma coagulation procedures were performed immediately6,7 (Fig. 2A–D).
ESD procedures
ESD procedures were performed as shown in Figure 3. Several marker dots were made around the lesion with argon plasma coagulation. After the injection of several milliliters of submucosal injection solution (100 mL of saline + 5 mL of 0.2% indigo carmine+1 mg of epinephrine) into the submucosal layer, the mucosa was incised outside the marker dots with an IT or hook knife. The submucosal tissue underneath the lesion was then gradually dissected with an IT or hook knife. Submucosal injection solution was injected repeatedly during the dissection whenever necessary. If the lesion did not lift during or after the submucosal dissection, an IT knife or hook knife was used to carefully dissect the lesion along the tumor margin to ensure that no residual tumor remained. Exposed vessels on the artificial ulcer were coagulated with argon plasma coagulation or hot biopsy forceps to prevent delayed bleeding; metallic clips were always used to close deeply dissected areas8–10 (Fig. 3).
Duodenal Brunner's adenoma endoscopic submucosal dissection procedure:
Postoperative treatment
All patients were given 40 mg of omeprazole i.v. twice daily postoperatively. Patients were allowed oral intake from the third day unless serious complications occurred. 4 Patients usually remained hospitalized for 2–3 days following the ESD procedure. However, if the tumor was very small (<0.5 cm) and the surgeon was able to close the wound satisfactorily, patients remained in the endoscopic center for 2–3 hours and were then discharged in the absence of specific complaints.
Pathologic evaluation
A resection with a tumor-free margin, in which both the lateral and basal margins were free of tumor cells, was considered a complete resection. In contrast, a resection in which the tumor extended into the lateral or basal margins was considered an incomplete resection; these cases were recommended for close follow-up. Histopathologic evaluations were performed after ESD by two different pathologists.9,10
Follow-up
The patients were followed up with endoscopy at 1, 2, 6, and 12 months after endoscopic resection and annually thereafter. EUS was performed when the prior resection site appeared suspicious for a residual or recurrent lesion.
Results
In total, 30 Brunner's adenomas from 29 patients were treated during the study period. One patient received ESD for lesion recurrence after the initial EMR procedure. Among the patients, 13 (44.8%) were men. The median age was 55 years (range, 29–72 years). In total, 8 patients (27.6% [8/29]) reported upper abdominal discomfort/pain. Melena was observed in 27.6% (8/29) of patients; all other patients were asymptomatic (Table 1).
EMR, endoscopic mucosal resection; ESD, endoscopic submucosal dissection.
Tumors were located in the first portion of the duodenum in 20 cases (66.7% [20/30]), at the intersection of the first and second portions in 6 cases (20% [6/30]), and in the second portion in 4 cases (13.3% [4/30]). Of the 26 lesions located in the first portion and the intersection of the first and second portions of the duodenum, 9 (34.6%) were found in the greater curvature, 6 (23.1%) were in the anterior wall, 5 (19.2%) were in the lesser curvature, and 6 (23.1%) were observed in the posterior curve. The mean maximal dimension of the lesions was 1.7±0.1 cm (range, 0.6–7 cm). Overall, 60% (18/30) of tumors were less than 1 cm in size, 20% (6/30) were between 1 and 2 cm, and 20% (6/30) were larger than 2 cm in size. In total, 11 lesions (36.7% [11/30]) were characterized as long pedicle or subpedicle lesions.
Of the 11 long pedicle or subpedicle lesions, 9 were treated with SR. EMR procedures were performed in a total of 12 cases, including 10 lesions with submucosal tumor (SMT) presentation and a tumor diameter of <1 cm and 2 subpedicle lesions when SR was difficult. ESD was used to treat 9 lesions (30%), including 4 lesions with a diameter larger than 1 cm, 4 lesions where EMR was difficult, and 1 recurrent lesion that presented after an initial EMR procedure. The time required for ESD was measured from the time of marking the area until lesion resection. The median operation time for successful ESD cases was 35 minutes (range, 15–70 minutes).
As all lesions were resected in a single piece that included the surrounding markings, the en bloc resection rate was 100%. One EMR-resected lesion exhibited indeterminate tumor margins. As the tumors displayed benign features, patients were advised to undergo close follow-up without further intervention. The overall curative resection rate was 96.7% (29/30). Pathomorphological features of Brunner's gland are characterized by the presence of nondysplastic, lobulated Brunner's glands.
Only 1 case of delayed bleeding occurred; it was initially observed on Day 2 after the EMR procedure. Red-tinged fluid was aspirated from the patient's nasogastric tube on Days 2 and 3 after ESD; in addition, the patient's stool samples were black, and hemoglobin levels were decreased. An emergent gastroscopy, using hot biopsy forceps, was performed to achieve hemostasis. Following treatment, hemostatic drugs were administered, and the patient did not have further bleeding. No cases of delayed perforation or stenosis were observed (Fig. 4).
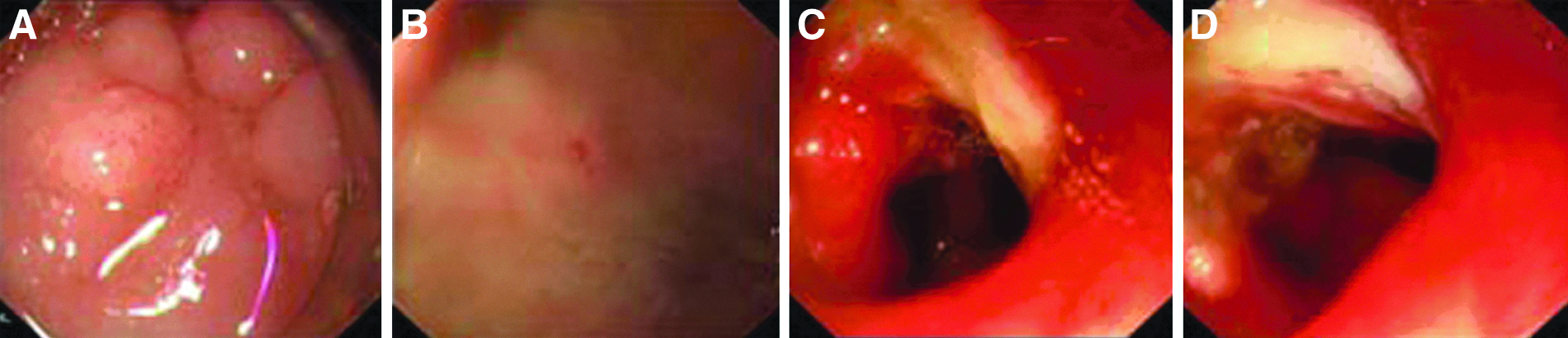
Common complications:
In the first month's follow-up visit, 14 lesions (46.7% [14/30]) exhibited wound healing. The remaining lesions exhibited signs of healing at the 2-month follow-up visit. Over the follow-up period (median, 13 months; range, 2–39 months), 1 patient whose resected tumor exhibited indeterminate margins presented with a lesion recurrence 1 year after the initial EMR procedure. An ESD procedure was recommended, and no additional recurrence was found during the subsequent follow-up period.
Discussion
Brunner's glands are normally located in the duodenum and extend from the pylorus to the second duodenal portion. They secrete mucus, pepsinogen, and urogastrone to protect the duodenum from acid chyme. Increased acid secretion, Helicobacter pylori infection, 11 and other inflammatory conditions are known to stimulate Brunner's gland hyperplasia. However, administration of acid secretion inhibitors or eradication of H. pylori infection could not induce regression, so Brunner's adenoma was not a simple hyperplasia; therefore, it was hypothesized to be a kind of adenoma. Consistent with the normal distribution of Brunner's glands, Brunner's adenomas are most often found in the proximal duodenum, with 70% of adenomas reported in the duodenal bulb, 26% in the second portion of the duodenum, and 4% in the third duodenal portion. 2 The majority of Brunner's adenomas commonly range between 1 and 2 cm in diameter. Endoscopically, Brunner's adenoma was recognized as a polypoid elevation or polyp lesion. It was histologically characterized by neoplastic proliferation of the gland. 12 These results are consistent with our findings. However, endoscopically, Brunner's gland hyperplasia was also recognized as an elevated or polyp lesion. It was histologically characterized by hyperplastic proliferation of the gland. In biopsy specimens, differentiation from Brunner's gland adenoma was occasionally difficult. 12 We found the difference between them from the endoscopic treatment of the resection specimen.
Brunner's adenomas are usually asymptomatic and diagnosed incidentally during upper gastrointestinal endoscopy. However, they can sometimes cause symptoms such as gastrointestinal bleeding, intestinal obstruction, and, rarely, an ampullary obstruction, pancreatitis, and intussusception, conditions that require surgical laparotomy or laparoscopy interventions. 4 It is noteworthy that carcinoma may arise from Brunner's gland adenoma. 12
The majority of Brunner's adenomas that we found were small and asymptomatic. The traditional management option is close follow-up and surgical tumor resection. Recently, with the development of endoscopy devices and techniques, endoscopic resection has emerged as an alternative treatment option. However, whether small lesions require treatment has been controversial within the field. Based on the following findings, we believe that treatment of small lesions is necessary. Although Brunner's adenomas are usually described as entirely benign lesions, malignant transformation has been identified in several reports. As the biological behavior of Brunner's adenomas is unknown, Brookes et al. 13 postulated that it may be dangerous to presume that all cases of Brunner's adenomas are nondysplastic and nonmalignant based on tumor size.14,15 Additionally, even asymptomatic benign tumors can cause the development of complications such as obstruction, bleeding, or twisting due to tumor growth. Thus, it may be preferable to undergo microvasive endoscopic resection early, as opposed to requiring laparotomy after allowing tumor growth. Furthermore, preoperative imaging studies, such as ultrasonography, EUS, and computerized tomography, lack suitable specificity for diagnosis. 16 The use of EUS with fine-needle aspiration with respect to brunneromas is controversial. EUS with fine-needle aspiration has a sensitivity of 80%–100%, but it is not suitable if the tumor is too small. Additionally, sampling increases the risk of tumor metastasis through the channel of the needle if the tumor has undergone malignant transformation. 17 Bite-on-bite biopsies do not yield the precise pathological result if the tumor is too deep, and they can carry the risk of bleeding in some cases. Thus, we recommend endoscopic resection for small Brunner's tumors, not only for treatment, but also to enable precise diagnosis.
Based on our experiences and the anatomic features of the duodenum, different lesions should be treated with different methods. If the Brunner's adenomas were polyps with long pedicles or subpedicles, polypectomy was chosen, no matter the lesion diameter. If the lesions presented as SMTs on gastroscopy, the lesion diameter was not larger than 1 cm, and the lesions were not associated with the muscularis propria, as diagnosed by preoperative EUS, EMR was chosen. ESD was chosen if the lesion diameter was larger than 1 cm or if lesions were associated with muscularis propria. Additionally, if, during the EMR procedure, saline spread into surrounding normal tissues and the lesions became flattened, making them impossible to remove, ESD was performed. Recurrent lesions should also be treated with ESD.
As shown in our data, the EMR technique exhibits limitations for the treatment of duodenal SMTs, including Brunner's adenomas. During several EMR procedures, saline spread into surrounding normal tissues, and the lesions became flattened, making it impossible to remove them by EMR. Thus, surgeons were required to change to ESD. In our study, EMR treatment failed in 25% (4/16) of cases. 18 The duodenum exhibits a double blood supply system with abundant blood vessels in the submucosal layer. Postoperative gastric acid erosion in the artificial ulcer may increase the risk of delayed bleeding. In contrast to EMR, ESD procedures could directly observe the hemostasis of the exposed artery, possibly reducing complications. As shown by our group, delayed bleeding was only observed following EMR treatment, but not in patients treated with ESD. Additionally, in contrast to EMR, tumor resection along the tumor margin was performed under direct vision in ESD procedures, ensuring that no residual tumor remained. ESD also could give a sufficient tumor margin (circumferential margin and vertical margin) for precise pathologic diagnosis. In our study, tumor recurrence occurred in 1 patient following EMR and was associated with indeterminate tumor margins at the time of the original procedure.
Conclusions
Endoscopic treatments offer an effective localized treatment for Brunner's adenomas in the duodenum with relatively low complication and mortality rates. SR was chosen for lesions with long pedicles or subpedicles. If the lesions were SMTs, ESD was the first choice rather than EMR. We share our experiences and hope that they will be useful for the rational treatment of Brunner's adenomas in the duodenum. However, large, prospective, multicentered studies are required to further corroborate these results.
Footnotes
Acknowledgments
This work was supported by grants from the Shanghai Science and Technique Committee (numbers 09DZ1950102, 09411967100, and 10411955900) and the National Natural Science Foundation of China (number 81101566).
Disclosure Statement
No competing financial interests exist. Y.-S.Z. and L.-Q.Y. designed the research. Q.S. and S.-Y.C. analyzed and interpreted the data. Q.S., H.-F.W., and Y.-S.Z. drafted the article. P.-H.Z. and M.-D.X. performed a critical revision of the article for important intellectual content. L.-Q.Y. provided the final approval of the article. All authors read and approved the final manuscript.