
Abstract
Abstract
Objective:
To retrospectively review our initial experience with respect to evaluating the feasibility and safety of retroperitoneal laparoendoscopic single-site surgery (LESS) for renal cyst decortication using the single trocar technique.
Patients and Methods:
Between April 2010 and November 2011, 45 patients with symptomatic simple renal cyst have undergone retroperitoneal LESS using the single trocar technique by the same experienced laparoscopic surgeon. A 10-mm 0° laparoscope with a 6-mm working channel and straight conventional laparoscopic instruments were used during all the procedures. Salient demographic and operative data were recorded, including age, body mass index, operative time, estimated blood loss, perioperative complications, analgesic requirement, etc.
Results:
Forty-three cases were accomplished successfully. In the remaining 2 patients dense adhesions around the renal cyst were encountered, and the operations were completed with an additional 5-mm trocar. The mean operative time was 49 minutes. The mean estimated blood loss was 12 mL. The mean in-hospital analgesic requirement was 2.8 mg of morphine equivalent. The mean time for ambulation postoperatively was 2 days; at the same time the drainage catheter was removed. The mean hospital stay was 3 days. There were no major perioperative complications, but superficial wound infection was noted in 1 patient.
Conclusions:
Our initial experience with retroperitoneal LESS by the single trocar technique shows the safety and feasibility for renal cyst decortication and provides acceptable operative outcomes.
Introduction
In most LESS surgery the transperitoneal approach is generally used, and limited substantive experience supports LESS via the retroperitoneal approach. 3 Nonetheless, the retroperitoneal approach is exceedingly familiar to the urologist and has some advantages, such as more direct access to the retroperitoneal organs and a potential reduction in invasiveness. In the published reports about the retroperitoneal LESS, commercial or homemade LESS platforms were generally used.4,5
We present our institution's initial experience with retroperitoneal LESS for renal cyst decortication by the single trocar technique, which is different from the aforementioned LESS platforms. The present study retrospectively reviewed our procedures for this novel LESS; as well, the feasibility and safety, its technical details, potential advantages, and limitations are also discussed.
Patients and Methods
Between April 2010 and November 2011, 45 patients with symptomatic renal cyst underwent retroperitoneal LESS by the single trocar technique. One experienced laparoscopic surgeon (B.X.) performed all the procedures. Prior to surgery, we gave all patients a full description and explanation about various treatment options, including percutaneous aspiration with or without sclerotherapy and open, conventional retroperitoneal laparoscopic or this novel retroperitoneal LESS decortication. The surgical decisions were made after obtaining informed consent from the patients and institutional review board of our hospital. All patients presented with flank pain, with the symptoms having been present for 2–6 months (mean, 3 months). Severity of pain was characterized using the 10-point visual analog pain scale (VAPS), where no pain and the worst pain are scored at 0 and 10 points, respectively. The same inclusion and exclusion criteria that are used for conventional retroperitoneal laparoscopic surgery were applied. The diagnosis of renal cyst was established by ultrasonography and computed tomography imaging. All the cases underwent intravenous urography in order to exclude a possible communication with the collecting system. All the renal cysts were simple, unilateral, solitary, and peripheral. The patients' characteristics are shown in Table 1.
BMI, body mass index.
Operative technique
Under general endotracheal anesthesia, the patient was placed in the full lateral position and securely fixed on the operating table with all pressure points well padded. The table was flexed at the waist level to maximize the space between the lowermost rib and the iliac crest. Then, a transverse skin and fascia incision was made over the midaxillary line, halfway between the ipsilateral lower costal margin and the iliac crest. The underlying muscles (obliques and transversalis) were bluntly split up to the anterior thoracolumbar fascia. The thoracolumbar fascia was penetrated for entrance to the retroperitoneum. By gentle finger dissection to push the peritoneum forward, a retroperitoneal space was initially developed between the psoas muscle posteriorly and Gerota's fascia anteriorly. Subsequently a 12-mm blunt-tip trocar was placed in position through the incision, and carbon dioxide was instilled through the insufflation channel of the trocar to a maximum pressure of 12–15 mm Hg. Then, a rigid 10-mm 0° laparoscope (Karl Storz, Tuttlingen, Germany) with a 6-mm working channel (Fig. 1) was inserted to bluntly dissect the retroperitoneum under direct vision. Thus an adequate working space was safely created outside Gerota's fascia. Straight conventional laparoscopic instruments were used for subsequent manipulation. Retroperitoneal fat tissue outside Gerota's fascia was sharply dissected until it prolapsed downward to the iliac fossa. After the Gerota's fascia was incised longitudinally, the blue-domed renal cyst was separated from the retroperitoneal attachments by blunt and sharp circumferential dissection (Fig. 2A and B). Then, a suture with a straight needle was delivered into the retroperitoneum by directly puncturing at the posterior axillary line below the 12th rib, through the renal cyst wall and then out through the body wall again (Fig. 2C and D). By suspension of the suture with extracorporeal handling, the renal cyst wall was excised enough for wide deroofing, and cyst fluid was aspirated (Fig. 2E). Then, the suture was cut and removed. The margins of the residual cyst wall were fulgurated (Fig. 2F), and the cavity was then packed with perinephric fat to minimize the recurrence. The specimen was directly retrieved through the single trocar for pathological analysis. Air pressure then was decreased to between 5 and 6 mm Hg to identify potential bleeding sites, and satisfactory hemostasis was confirmed. We routinely placed a rubber drainage catheter in situ through the incision. Fascia and skin were carefully sutured to avoid the possible development of a hernia.
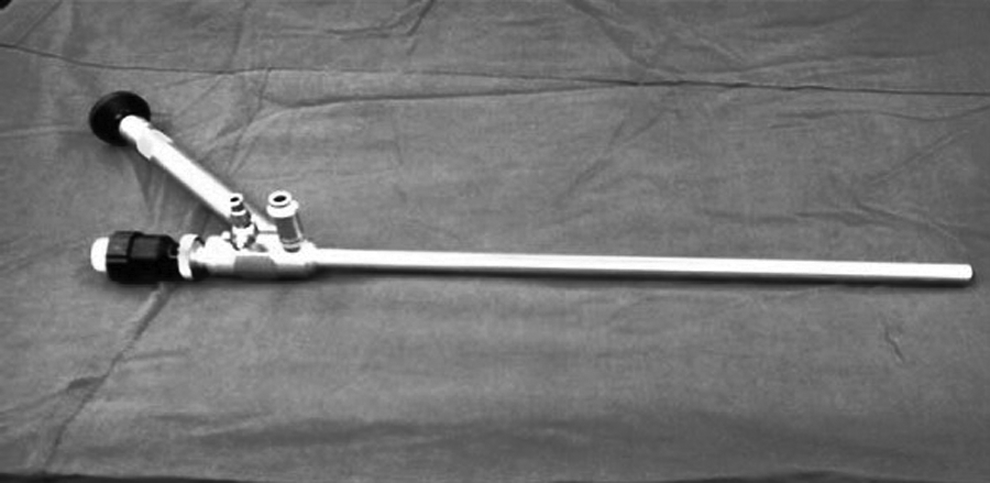
Operative laparoscope (10-mm 0°; Karl Storz).
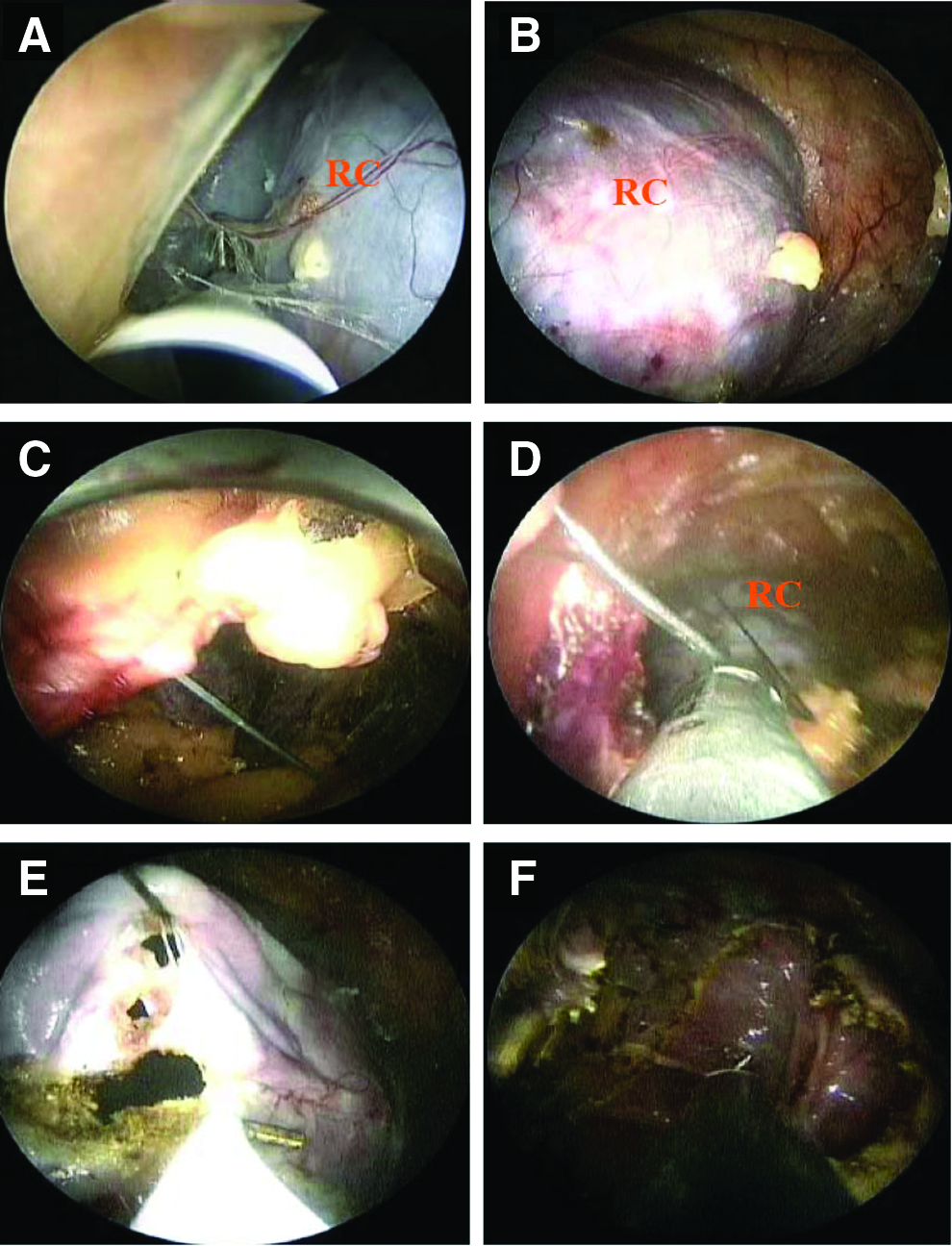
Intraoperative views.
Statistical analysis
Perioperative and postoperative data were obtained retrospectively for all patients, including incision length, operative time, estimated blood loss, the number of conversions to standard laparoscopy or open surgery, the time to oral intake resumption and ambulation, the duration of hospital stay, etc. The dose of analgesics needed postoperatively was converted to dose (in mg) of parenteral morphine equivalent. The patients were followed up by ultrasonography for objective evidence of recurrence. Preoperative and postoperative VAPS scores in patients were compared using Student's paired t test, with statistical significance indicated at P<.05. Data are presented descriptively with mean (range) values.
Results
Retroperitoneal LESS for a renal cyst was successfully accomplished in 43 of the 45 patients by the single trocar technique. In the remaining 2 patients, the operations were completed with an additional 5-mm trocar placed in the posterior axillary line below the 12th rib because of dense adhesions around the renal cyst. There was no conversion to an open procedure. Among all these cases, blood transfusion was not required, and no intraoperative complications (e.g., peritoneal tear, subcutaneous emphysema, or bleeding) occurred.
The perioperative and postoperative variables are detailed in Table 2. Mean operative time was 49 minutes, and mean estimated blood loss was 12 mL. The mean in-hospital analgesic requirement was 2.8 mg of morphine equivalent. Twenty-eight patients required no postoperative analgesia, and only 5 needed pain medication 24 hours postoperatively. The mean time for ambulation postoperatively was 2 days; at the same time the drainage catheter was removed. The mean hospital stay was 3 days. A minor postoperative superficial wound infection developed in 1 patient that prolonged his hospital stay to 1 week, and the remaining patients had good wound healing (Fig. 3). The pathological diagnosis of each case was benign simple renal cyst. VAPS scores decreased from a mean of 8.5 preoperatively to 1.2 at 1 month postoperatively (P<.05). At a mean follow-up of 3.5 months, no local recurrence was detected by ultrasonography in any case.

Postoperative scar at the trocar insertion site.
EBL, estimated blood loss.
Discussion
Simple renal cysts are common in the general population and generally asymptomatic. However, several symptoms may be indicative of renal cysts, which include flank pain, hematuria, hypertension, infection, and urinary tract obstruction. When these features are present, treatment is usually required. The management of symptomatic simple renal cysts is usually by minimally invasive procedures such as percutaneous aspiration with or without sclerotherapy and laparoscopic decortication. Percutaneous aspiration (with or without sclerotherapy) had a high recurrence rate and some complications, such as bleeding, urine leak, and spillage of the sclerosing agent into the retroperitoneum, which can induce severe perirenal inflammation and secondary ureteropelvic junction obstruction. 6 Another limit of the technique is that there is no histopathological evaluation, missing, in rare cases, a cystic tumor. Since the advent of laparoscopy in the 1990s, laparoscopic management of renal cysts has been confirmed as safe and effective. 7
Following application to various urological diseases, laparoscopic surgery has been shown to result in less postoperative pain for the patient, improved cosmetic outcomes, and shorter hospitalizations and convalescence compared with open procedures. Conventional laparoscopic surgery achieves the performance of major intra-abdominal operations through multiple (three to six) small incisions and placement of the respective number of trocars and instruments. However, each working port risks morbidity from pain, bleeding, port-site hernia, internal organ damage, and even undesirable cosmesis.8,9 A new alternative to the conventional laparoscopy is LESS. In LESS the multiple incisions and trocars are replaced by a single incision and a multichannel single port that provides access to several instruments. The LESS technique was initially attempted and reported about 10 years ago in the general surgical and gynecologic literature.10,11 Recently LESS has witnessed a renaissance owing to the development of various single-port devices and flexible operating instruments.
In the urologic field, LESS was initially described in an abstract and video presentation by Rane and associates during the 25th World Congress of Endourology meeting in Cancun, Mexico, in 2007. Also in 2007 Raman et al. 12 reported their initial experience with transumbilical keyhole nephrectomy in pigs and humans by the multitrocar technique (a single incision to introduce three adjacent trocars). In the last 3 years, numerous initial experiential reports have confirmed the feasibility and safety of LESS within the field of urology. 13
In general, both transperitoneal and retroperitoneal routes have been described for LESS with variable strategies in terms of patient positioning, incision site, and port placement. But, most laparoscopic surgeons have not preferred the retroperitoneal approach, particularly for LESS, because of a smaller working space and difficulty in identifying anatomic structures. However, the retroperitoneum is exceedingly familiar to the general urologist because of the preponderance of genitourinary organs located therein. The advantages of the retroperitoneal approach, compared with the transperitoneal approach, include more direct access to the retroperitoneal organs, less need for visceral retraction or bowel manipulation, elimination of the risk of hollow viscous injury and intraperitoneal contamination with tumor cells or infectious organisms, less postoperative paralytic ileus, and absence of peritoneal irritation by insufflated CO2.14,15 It is especially valuable for patients who need to maintain peritoneal integrity or those with an abnormal or obliterated peritoneal space. Moreover, the distance from the port site to retroperitoneal organs is shorter than that of the transumbilical approach; therefore, a wider range of motion is obtained, and the bent instruments are not as useful as in transperitoneal procedures. Although the transumbilical LESS is a virtually scar-free procedure, a small port-site scar on the back is usually acceptable to patients.
In 2005, Hirano et al. 16 described the first series of retroperitoneoscopic single-port adrenalectomy performed with a 4-cm-diameter rectoscope tube and conventional laparoscopic instruments through a 4.5-cm single incision. Although this procedure was not truly laparoscopic, it provided a platform for the evolution of retroperitoneal LESS. In 2008, Kaouk et al. 17 described their first 10 cases with the LESS procedure, including the first-ever retroperitoneal LESS for cryoablation of renal tumors. In the series of retroperitoneal LESS reported by Ryu et al., 5 renal cyst decortication, adrenalectomy, nephroureterectomy, nephrectomy, and ureterolithotomy were involved, and the Alexis wound retractor attached with a surgical glove outside the wound was used as a homemade LESS platform. Several other clinical series from multiple academic institutions have continued to support the feasibility and safety of retroperitoneal LESS in patients with urologic disorders (Table 3).
Commercial products were manufactured as follows: TriPort™ by Olympus, SILS Port™ by Covidien, GelPOINT™ by Applied Medical Resources Corp., and Uni-X™ by Pnavel Systems, Inc.
In 1 patient, renal cyst decortication and renal biopsy were performed simultaneously.
LESS, laparoendoscopic single-site surgery; NR, not reported.
Commercial LESS platforms (e.g., R-Port™ [Advanced Surgical Concepts Ltd.] or Uni-X™ Single Port [Pnavel Systems, Inc.]) are not only expensive but also not generally available in China. Although the homemade LESS platform as described above is cheap, it still takes some time to construct the device during surgery and has the risk of surgical glove tear, gas leaking, or losing insufflation pressure. 22 A 10-mm laparoscope similar to a nephroscope with a 6-mm working channel, as used in our study, let us successfully perform retroperitoneal LESS for renal cyst decortication by the single trocar technique in 95.56% of the patients. In 1998 Esposito 23 reported his experience in performing one-trocar laparoscopic appendectomy by a 10-mm operative laparoscope with a 5-mm working channel. Using the similar operative laparoscope, Micali et al. 18 performed retroperitoneal LESS for renal biopsy in 4 patients, 1 of whom simultaneously underwent renal cyst decortication and renal biopsy. In the aforementioned conventional LESS, the surgeon and assistants need to work together in close proximity, which leads to an indigent posture and requires constant coordination. But during our retroperitoneal LESS by the single trocar technique, the surgeon held the laparoscope by himself, which reduced the burden of assistants. Through the working channel of the laparoscope, we can insert straight conventional laparoscopic instruments by turns and complete circumferential dissection of renal cysts. This may avoid the inevitable collision of instruments in the conventional LESS. LESS is more challenging for performing proper tissue manipulation and traction because placing several parallel instruments makes triangulation between the right- and left-hand instruments and the laparoscope more difficult. Navarra et al. 24 placed transparietal sutures anchored in the gallbladder wall for gallbladder suspension and exposition during the laparoscopic cholecystectomy. Enlightened by them, we used transparietal sutures anchored in the renal cyst wall and grasped with extracorporeal handling, which enables us to obtain better angulations for the deroofing of the renal cyst and partially offsets the technical difficulty. However, we had difficulty in removing intra-abdominal retained smoke, which often blurred the surgical field, and even opening the laparoscope valve intermittently was not effective.
Our study shows that retroperitoneal LESS can be safely and feasibly performed in patients with a renal cyst using the single trocar technique within a reasonable time with limited blood loss. In addition, there was no conversion to open procedures, and no intraoperative complications occurred. This is likely attributable to all procedures being performed by an experienced surgeon with confident laparoscopic skills who had previously completed more than 1200 cases of laparoscopic surgery. This new technique offers several tangible benefits, such as better cosmetic results, less postoperative pain, and better convalescence. First, only one small scar remains on the back (Fig. 3), which raises patient satisfaction in terms of esthetic outcome. Second, on the basis of our initial experience, retroperitoneal LESS by the single trocar technique offers a substantial reduction of pain after surgery, as revealed by the postoperative analgesic requirement. Third, patients recover rapidly as reflected by the short time for oral intake and ambulation postoperatively in the present study.
In our opinion, less technically demanding procedures such as renal cyst decortication offer surgeons an appropriate introduction to the retroperitoneal LESS by the single trocar technique. With cumulative experience we can master the basic laparoscopic skills of this new technique, such as intracorporeal suturing, dissection, and ligation. On this basis, we will be able to expand the indication in urologic surgery. Even among those with considerable laparoscopic experience, adaptation to this new technique requires time and patience. Therefore the learning curve with this novel LESS should be expected. We did not attempt to evaluate the superiority of this novel LESS over conventional LESS or laparoscopy because our cumulative observational outcomes are retrospective and preliminary. Additional surgical experience, longer follow-up, and large-scale randomized controlled trials are indeed necessary to answer this question.
Conclusions
On the basis of our initial experience, retroperitoneal LESS by the single trocar technique shows the safety and feasibility for renal cyst decortication and provides acceptable operative outcomes. Additional improvement of instruments and future cumulative surgical experience with larger patient numbers may enable us to minimize the challenges of more complex procedures in urology, such as ureterolithotomy, adrenalectomy, or even simple nephrectomy. Future prospective, randomized controlled trials are underway to better establish the role of this novel LESS in urologic surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.