
Abstract
Abstract
Treatment of kidney stones in pelvic ectopic kidneys of children is a challenging procedure for urologists. Herein we report a case of laparoscopy-assisted “microperc” in a 3-year-old girl with a stone in her pelvic ectopic kidney. This micro-optical system is helpful in confirming the percutaneous access and provides the possibility of fragmenting the stone without the necessity of dilating the tract.
Introduction
“
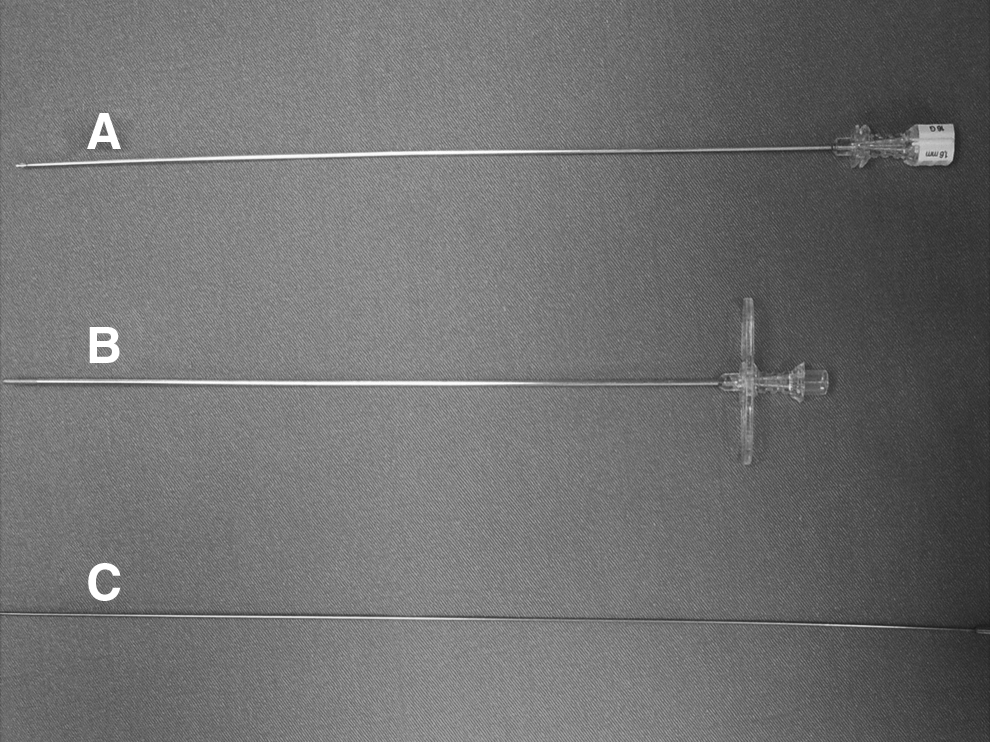
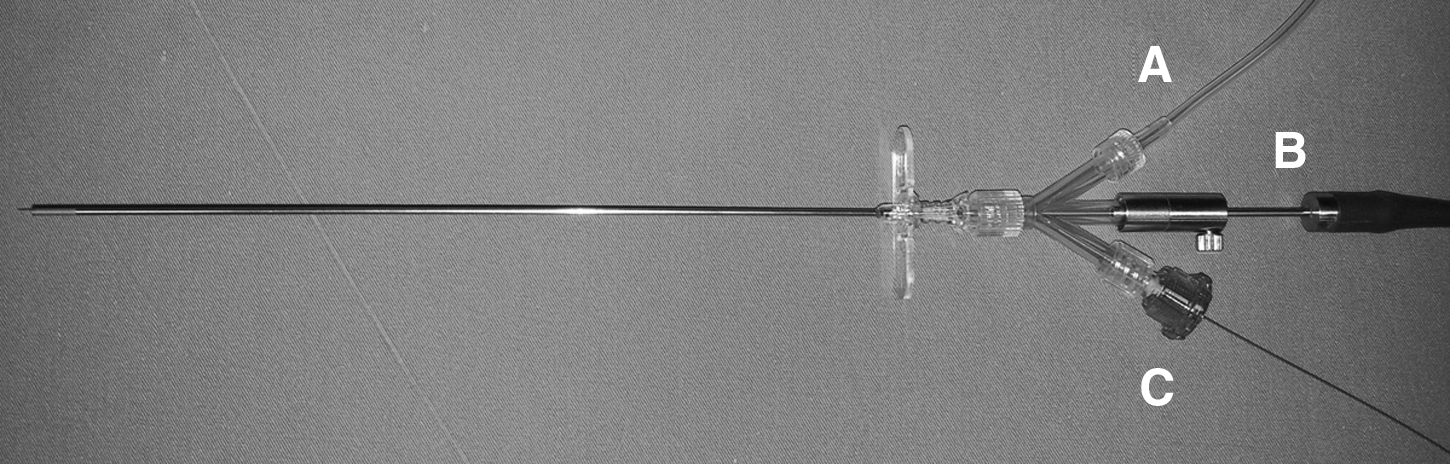
The microperc system: a three-way connector that allows the use of
The stone in pelvic ectopic kidneys is an uncommon situation and requires special intervention whenever detected. Combination of laparoscopy and PNL has been previously described in such cases.4–8
Herein we report a case of a stone located in an ectopic pelvic left kidney and treated with laparoscopy-assisted microperc.
Case Report
A 3-year-old girl was diagnosed with 12 mm of an upper pole stone refractory to shock wave lithotripsy in the left pelvic ectopic kidney (Fig. 3). After the signed informed consent was obtained, the patient was placed under general anesthesia, and a 5 French ureteral catheter was placed transurethrally and attached to the urethral catheter draining the bladder prior to the procedure. Then the patient was placed in the supine position, allowing the use of fluoroscopy. A 5-mm trocar was primarily inserted to the peritoneal cavity under direct vision through the infra-umbilical incision. Pneumoperitoneum was created at a pressure of 6 mm Hg. Then the other 5-mm trocars were placed in the right and left margins of the rectus muscle. The pelvic kidney located above the bladder in the midline was exposed laparoscopically. After the lateralization of the bowels, retrograde pyelogram was performed, and the collecting system with the renal stone in the upper pole was visualized. Subsequently, a 4.85 French all-seeing needle was used to access the collecting system under direct vision (Fig. 4). Then the three-way connector was attached to the proximal end. Stone fragmentation was performed using a holmium:YAG laser fiber (200 μm) through the same needle sheath. The irrigation pump system with pressure set to 50 mm Hg was controlled by the operating surgeon and was used whenever the vision was blurred. To minimize heat loss during the operation, 0.9% NaCl warmed to 37°C was used as an irrigant. The stone was completely fragmented, and no complication occurred. No nephrostomy tube or double-J stent was inserted, and the patient was sent to bed rest totally stent free. No postoperative complication was recorded, and no ancillary procedure was required. The patient was discharged within 48 hours. Kidney, ureter, and bladder ultrasonography on postoperative Day 7 confirmed the complete clearance of the stone.
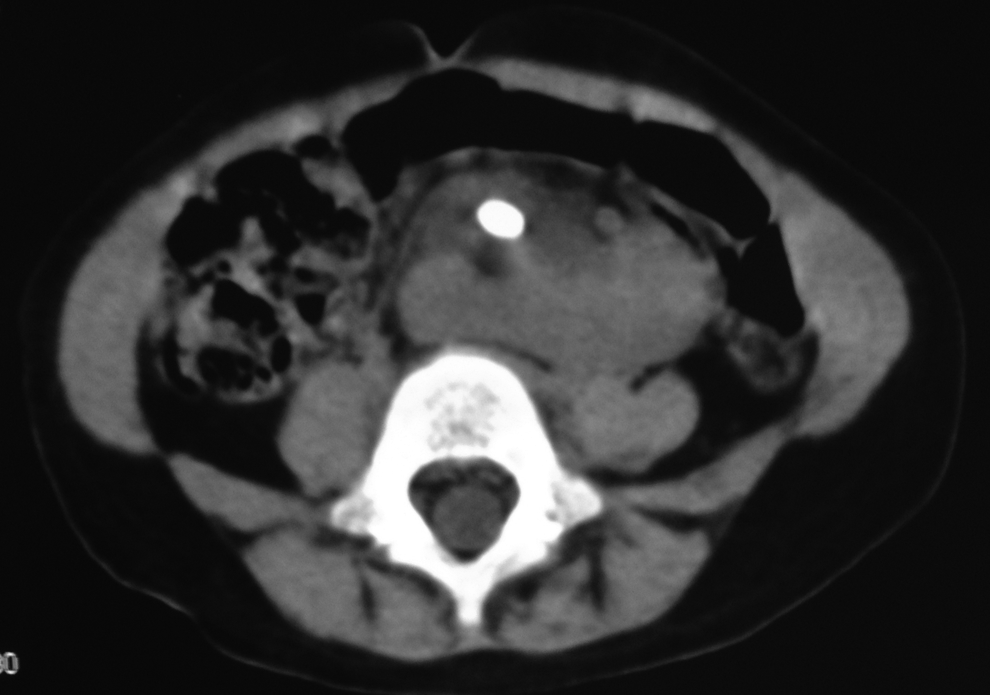
Preoperative abdominal computed tomography demonstrates 12-mm calculi in the ectopic pelvic kidney.

Laparoscopic appearance of the introduction of the all-seeing needle into the renal paranchyma.
Discussion
The incidence of pelvic-located kidneys is reported to be 1:2200–3000 in autopsy series. 6 Although there is no increased risk of diseases in such kidneys, the risk of nephrolithiasis and hydronephrosis is thought to be elevated. 7 Therefore, whenever such positioning is detected, the treatment of stones, especially in children, is a challenging procedure. To overcome this anatomical difficulty, combination of laparoscopy and PNL has been previously described in several series.4–8 Laparoscopy is primarily used to avoid any bowel injury and allows better visualization during dilatation of the tract for performance of PNL. Ensghi et al. 9 were the first to use the assistance of laparoscopy in the treatment of a staghorn stone located in a pelvic kidney. Subsequently, similar reports have been published with limited numbers of cases. Holman et al. 10 have reported 15 cases that were managed successfully; the only complication reported was the delayed urine leakage into the abdominal cavity in 1 patient. Other researchers have reported 11 cases of laparoscopy-assisted treatment of pelvic kidney stones. 8 In that series, the authors performed PNL in 5 cases refractory to shock wave lithotripsy; pyelolithotomy was performed in the other 6 patients with relatively large calculus. They concluded that the combination of laparoscopy and nephroscopy is safe and effective. Our patient had a semi-opaque calculus that was also refractory to shock wave lithotripsy, and because of her young age we chose not to perform flexible ureteroscopy. Therefore, we have decided to use the combination of laparoscopy and microperc in order to facilitate a safer access to the kidney. Finally, the procedure was successful, and no complication was encountered.
Miniaturization of the instruments in PNL has brought us microperc, which has the smallest available tract size to date. One of the advantages of this system is the introduction into the collecting system with the all-seeing needle. This helps urologists to facilitate the renal access, which is an important step of PNL. Another advantage is the very small size of the instrument, which is 1.6 mm. Although there is no comparative study up to now, this approach is expected to have minimal trauma to the renal parenchyma and less bleeding compared with standard or mini-PNL. There are only a few reports about this novel system in the current literature,1–3,11 and more investigations are required. The initial study was conducted in 10 patients, and 1 of them had an ectopic kidney. 2 That patient had two unsuccessful attempts with flexible ureterorenoscopy, and microperc was able to fragment the stone in the pelvic kidney. The authors concluded that the all-seeing needle helps to avoid bowel injury and that microperc is useful in such cases with anatomical abnormalities. In our patient, a 3-year-old girl, the preoperative computed tomography scan revealed that the pelvic kidney was surrounded with the bowels. Therefore we have decided to use the laparoscopic system for the lateralization of the bowels and combined with the microperc. We can conclude that this minimally invasive combination helped us to treat the patient appropriately without any complication.
Footnotes
Disclosure Statement
No competing financial interests exist.