
Abstract
Abstract
Background:
Single-incision laparoscopic surgery is a new procedure used to treat a variety of diseases requiring surgical intervention. The aim of this prospective comparative study is to compare the technical feasibility and safety of single-incision and three-port laparoscopic appendectomy.
Study Design:
Between February 2009 and April 2010, 102 patients with appendicitis were enrolled in this study. The patients were randomly assigned to two groups: single-incision or three-port laparoscopic appendectomy. Patients with perforated appendicitis were not excluded. We analyzed the patients' clinical characteristics and surgical outcomes.
Results:
There were no significant differences in preoperative patient demographics between the two groups with respect to body mass index (22.03±4.07 kg/m2 in the single-incision group versus 21.97±3.49 kg/m2 in the three-port group, P=.930). The pain score on the visual analog scale on postoperative Day 1 was significantly lower in the single-incision group than in the three-port group (3.22±1.22 versus 3.90±1.46, P=.012). Additionally, recovery time to daily life was significantly shorter in the single-incision group than in the three-port group (3.22±1.04 versus 3.94±1.43 days, P=.005). In patients with perforated appendicitis, the single-incision procedure took approximately 10 minutes less than the three-port procedure (44.11±7.75 versus 54.14±32.21 minutes, P=.449), and the postoperative hospital stay (P=.033) and recovery time to daily life (P=.001) were significantly shorter in the single-incision group.
Conclusions:
Single-incision laparoscopic appendectomy is a feasible and safe procedure, even in patients with perforated appendicitis, and this procedure is even less invasive than three-port laparoscopic surgical techniques.
Introduction
Two of the goals of minimally invasive surgery are to reduce the number and/or size of incisions. To that end, innovative methods such as natural orifice translumenal endoscopic surgery (NOTES™; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society for American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) and single-incision laparoscopic surgery (SILS) were recently introduced.4–7 NOTES is a technique that uses natural orifices as the entry point to the abdomen (transgastric, transvaginal, transvesical, transcolic, etc.). However, in most cases, an additional port must be placed at the umbilicus, so the term “scarless” is not a valid description. In SILS, one incision is made directly through the umbilicus, which is defined as a natural embryonic scar. Because of familiarity based on the laparoscopic procedure, the popularity of SILS rose. This procedure has also been referred to as embryonic-NOTES (e-NOTES). 8 To establish the feasibility and safety of SILS procedures, this approach has been used for relatively simple procedures, such as appendectomies and cholecystectomies. Although there have been many reports in the literature on SILS, most have been retrospective studies and have considered the technical aspects of the procedure.9–13
In 2010, we reported that laparoscopic transumbilical single-incisional appendectomy is feasible and has good postoperative outcomes based on retrospective data. 14 In this study, we conducted a prospective, randomized trial comparing single-incision laparoscopic appendectomy (SILA) with conventional three-port laparoscopic appendectomy (CTLA) for acute appendicitis.
Patients and Methods
Sample size and randomization
After approval by the Institutional Review Board, patients were randomized to the SILA group or the CTLA group. The primary outcome variable was postoperative wound pain. Using a power of 0.8 and an alpha of 0.05, we determined that we needed a sample size of 102 patients. We enrolled 102 patients with acute appendicitis, including perforated appendicitis, in this study from February 2009 to April 2010. The patients were enrolled after we obtained informed consent from the patient or the patient's legal guardian. A computer-generated individual unit of randomization was used.
Surgical procedure
Before the operative procedure, the same prophylactic antibiotics were administered intravenously to all patients. All appendectomies, whether SILA or CTLA, were performed by a single surgeon (D.L.) during the interval of this study.
CTLA
A 10-mm trocar was inserted through a vertical transumbilical incision for the videoscope. Then, two 5-mm trocars were inserted for surgical instruments: one was located suprapubically, and the other was located in the left lower quadrant of the abdomen. The appendix and mesoappendix were divided using ultrasound-activated scissors (laparoscopic coagulation shears [LCS®]; Ethicon Endo-Surgery, Cincinnati, OH). After the appendiceal base was ligated with an endo-loop (SJ Medical, Paju, Korea), the appendix was resected by ultrasound-activated scissors. The resected specimen was removed through the 10-mm trocar site using a disposable bag. If needed, closed suction drainage was inserted through the suprapubic 5-mm trocar site after irrigation. After the fascia was closed at the 10-mm trocar site, incisions for the three ports were closed.
SILA
Before making the skin incision, we prepared a single-port device that was made of a surgical glove and three 5-mm trocars. After a 2-cm skin incision was made through the umbilicus, we applied a double-ringed wound retractor (Alexis wound retractor XS®; Applied Medical, Rancho Santa Margarita, CA) to the incision site. Then, the single-incision device was latched to the wound retractor and rolled over to provide a seal (Fig. 1). The appendectomy was performed by a procedure identical to a classic laparoscopic appendectomy. The specimen was extracted through the incision site. If drainage was necessary, a closed suction drain was placed through the umbilical incision site. Then, the fascia and skin incisions were closed.
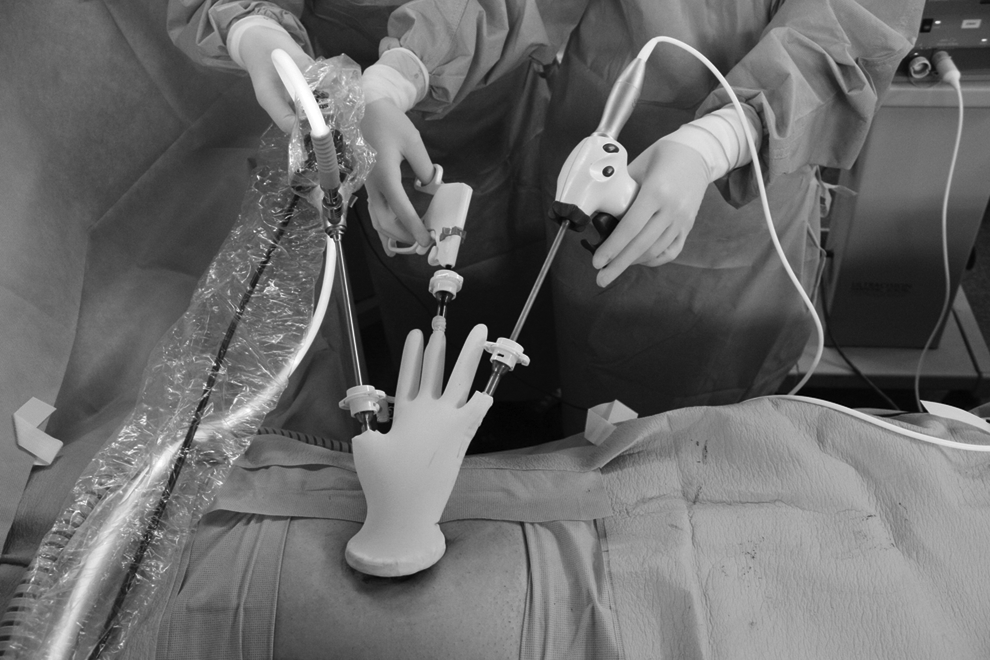
Depiction of a single-incision laparoscopic appendectomy with installation of a double-ringed wound retractor with a surgical glove to the transumbilical incision site.
Follow-up
Usually, when the condition at which usual activities of daily life were recovered had been achieved, we recommended that the patient be discharged from the hospital. After hospital discharge, patients visited the outpatient clinic on 1 week, 1 month, and every 6 months after hospital discharge. Also, whenever a patient had an abdominal problem after discharge, we recommended that the patient visit our hospital.
Parameters
We compared age, body mass index, leukocyte count, C-reactive protein level, and duration of symptoms preoperatively between the two groups. The operative time was measured by total procedure time and total anesthesia time. On postoperative Day (POD) 1 and POD 2 (i.e., at 24 and 48 hours after appendectomy), wound pain was measured by the visual analog scale (VAS) pain score system and frequency of analgesic use by the doctor who had worked in the ward and was not part of the surgical team. Additionally, we compared the postoperative complication rate, the length of postoperative hospital stay, and the recovery time to daily life between the two groups. The recovery time to daily life was defined as the ability to tolerate a regular diet and to return to full physical activity.
Statistical analysis
Continuous variables including age, body mass index, leukocyte count, C-reactive protein, preoperative duration of symptoms, operative time, pain score using the VAS system, frequency of analgesic use, hospital stay, and recovery time to daily life were compared using Student's t test and expressed as mean±standard deviation values. Categorical variables including perforation, conversion, and postoperative complication were analyzed with the χ2 test. Significance was defined as a P value of ≤.05. All statistical analyses were performed using the Statistical Package of the Social Sciences (SPSS) version 15.0 for Windows (SPSS, Inc., Chicago, IL).
Results
Preoperative period
There were no significant differences in age, body mass index, duration of symptoms, and leukocyte count between the two groups (Table 1).
Continuous variables are given as mean±standard deviation values.
CTLA, conventional three-port laparoscopic appendectomy; SILA, single-incision laparoscopic appendectomy.
During the operation
The mean operative time of the SILA group was slightly shorter than that of the CTLA group, but the difference was not statistically significant (37.00±15.46 minutes versus 38.45±15.26 minutes, P=.635). There were no intraoperative complications in either group. One patient in each group required conversion to an open procedure (Table 2). One patient in the SILA group underwent conversion to open appendectomy because the appendiceal base was in poor condition. Although we attempted an intracorporeal base repair with two additional ports, open conversion was performed because the repair was incomplete. One patient in the CTLA group underwent conversion to open appendectomy because a mass-forming lesion was identified. This lesion was confirmed to be appendiceal tuberculosis. None of the cases required additional ports except for 1 case in the SILA group that required conversion.
Continuous variables are given as mean±standard deviation values. Categorical variables are given number (%).
CTLA, conventional three-port laparoscopic appendectomy; POD, postoperative day; SILA, single-incision laparoscopic appendectomy; VAS, visual analog scale.
Postoperative period
The pain score (VAS score) was significantly lower in the SILA group than that in the CTLA group on POD 1 (3.22±1.22 versus 3.90±1.46, P=.012). However, on POD 2, the pain scores using the VAS system were not significantly different (P=.460). The patients in the SILA group returned to daily life faster than those in the CTLA group (3.22±1.04 versus 3.94±1.43 days, P=.005) (Table 2). There were two postoperative complications in the SILA group and two in the CTLA group (Table 3). A patient with an intra-abdominal fluid collection who underwent SILA was treated by ultrasound-guided percutaneous drainage, and a patient who developed a minimal fluid collection after CTLA was managed with antibiotics. One patient developed a wound infection after CTLA that was managed in an outpatient clinic, and 1 patient developed paralytic ileus after SILA and was managed conservatively. In terms of the cosmetic outcome, both CTLA and SILA led to acceptable scars (Fig. 2). The mean length of follow-up was 20.8±5.1 months (range, 6–30 months). We did not experience any long-term complications including incisional hernia.
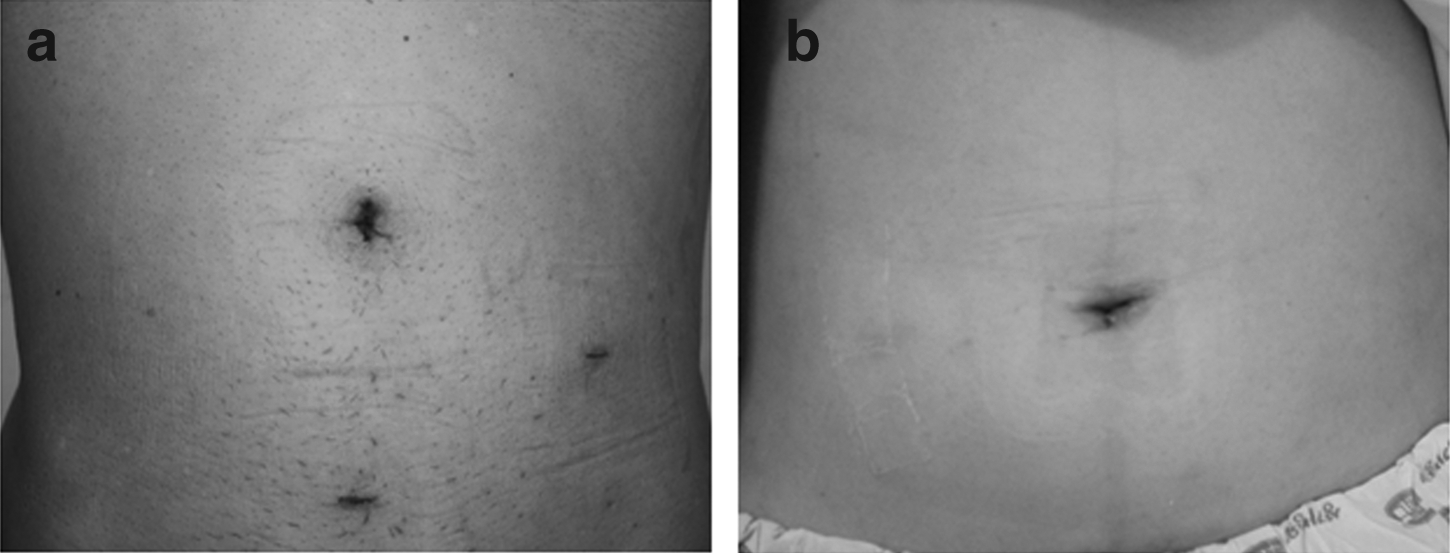
Scarring after appendectomy procedures:
CTLA, conventional three-port laparoscopic appendectomy; SILA, single-incision laparoscopic appendectomy.
Acute appendicitis with perforation
The operative time was not significantly different between the SILA procedure and the CTLA procedure (44.11±7.75 versus 54.14±32.21 minutes, P=.449). The postoperative hospital stay (P=.033) and the return time to daily life (P=.001) were significantly shorter in the SILA group than in the CTLA group (Table 4).
Continuous variables are given as mean±standard deviation values.
CTLA, conventional three-port laparoscopic appendectomy; POD, postoperative day; SILA, single-incision laparoscopic appendectomy; VAS, visual analog scale.
Discussion
Laparoscopic surgery has become the gold standard procedure for many abdominal operations. As surgical techniques and instruments have progressed and patients have demanded procedures that inflict less pain and have better cosmetic outcomes, surgeons have pursued minimally invasive techniques. NOTES may represent the final frontier for minimally invasive surgery, eliminating the need for a skin incision. This technique allows access to the abdominal cavity via transgastric, transvesical, transcolonic, or transvaginal approaches. However, it is still under development, and the safety and efficacy of the technique have yet to be established. NOTES requires several important considerations, including whether the endoscopist or the surgeon should undertake the procedure, whether the operation can be performed without peritoneal contamination, and whether there is a likelihood of a realistic benefit in patient recovery and perioperative morbidity compared with conventional multiport laparoscopic techniques. 5 Currently, these limitations complicate the widespread clinical implementation of NOTES. In contrast, SILS is a new technique that involves a transabdominal approach similar to conventional laparoscopic surgery but with fewer incisions. Since the first single-incision laparoscopic tubal ligation was performed by Wheeless 15 in 1969, SILS had been limited to some gynecologic operations. However, as laparoscopic surgery has become more common since the mid-2000s, SILS has been used for various abdominal operations, such as appendectomy, cholecystectomy, hysterectomy, ovarian cystectomy, and other surgeries. 8
At present, laparoscopic appendectomy is the standard procedure in patients with acute appendicitis with or without perforation. Laparoscopic appendectomy confers several advantages over open appendectomy, including a shorter hospital stay, less postoperative pain, earlier postoperative recovery, and a lower complication rate. 3 Since Pelosi and Pelosi 16 reported on a transumbilical single-puncture laparoscopic appendectomy in 1992, many surgeons have taken a profound interest in the SILA procedure. Recently, many reports have compared clinical outcomes and complication rates between SILA and conventional multiport laparoscopic appendectomy.17–21 Although these reports were almost retrospective or preliminary reports, they demonstrated that SILA was a safe and effective technique and a feasible surgical alternative to CTLA. Previously, many surgeons performed the SILA procedure only in cases of acute appendicitis without perforation or abscess because SILS causes a loss in triangulation, which may lead to poor visualization and handling within the abdominal cavity. 22 This will limit the surgeon's ability to thoroughly irrigate the peritoneum. Recently, a large prospective randomized trial involving 360 patients excluded patients with perforated appendicitis at the time of laparoscopic appendectomy. 23 Although the authors did not report why cases of perforated appendicitis were excluded, we speculated that the difficulty of cleansing the contaminated abdomen was the reason. Some suggested that adding an additional port could alleviate this difficulty. 24 However, the development of instruments for SILS and the increasing familiarity of surgeons with the procedure have led to solutions to this problem. In this study, we did not exclude the 16 patients with perforated appendicitis. In the SILA group, except for 1 conversion case, the contaminated abdomen was cleaned well without the need for an additional port. During the SILA procedure, we performed a saline irrigation via the single-incision site and cleaned the inflammatory exudate from the peritoneal cavity with a piece of gauze, which was achieved adequately via the single-incision site. The cleansing was repeated several times. However, this may be problematic during the CTLA procedure because the trocar only permits the passage of a small piece of gauze. 14 As a result, our data suggest that the SILA procedure for perforated appendicitis took slightly less time intraoperatively (however, the difference was not significant) and led to significantly earlier postoperative recovery (Table 4). This finding suggests that the SILA procedure can be performed feasibly and safely, even in perforated appendicitis with peritoneal contamination.
Most previous reports showed that the operative time in the CTLA group was shorter than that in the SILA group.14,23,24 One randomized controlled study reported that the operative time in the SILA group was 35.2 minutes compared with 29.8 minutes in the CTLA group. 23 In the present study, in contrast, the operative time was not significantly different between the SILA and CTLA groups (37.00±15.46 versus 38.45±15.26 minutes, P=.635). The difference in mean operative time does not translate to an individual appendectomy, which can be performed as quickly using the SILA procedure in the presence of straightforward anatomy. However, when the operation is difficult, such as in cases with a retrocecal appendix or severe adhesions due to significant inflammation, the CTLA procedure allows the dissection and mobilization to be performed more expeditiously without compromising significant operative time. Similarly, the shorter duration in the SILA group could be caused by reducing the time for port insert and wound closure and omitting wrapping the specimen in the disposal bag. Based on this result, we think that SILA may not be a difficult procedure for experienced and skillful surgeons.
In the field of minimally invasive surgery, some studies have shown less pain with less incisions.25,26 SILA is less traumatic than CTLA because no trocar in inserted into the abdomen through the abdominal muscles. We assessed wound pain with the VAS pain score system on POD 1 and 2. In our study, wound pain using the VAS system in the SILA group was significantly less than that in the CTLA group on POD 1 (3.22±1.22 versus 3.90±1.46, P=.012). However, this difference was not present on POD 2. In contrast, a pilot trial with 40 patients showed significantly greater pain scores in the initial 24 hours after SILA than after CTLA. 27 The authors hypothesized that the increased pain with SILA was due to a longer fascia incision and greater wound irritation in the SILA group. However, they reported that this difference in wound pain between the two groups disappeared by 48 hours after the operation. Our data differ from these results. We believe that the differences between the two study outcomes might result from the careful avoidance of wound irritation by the experienced surgeon performing SILA in our study. However, there was a commonality between the two studies in that a considerable portion of postoperative wound pain was reduced by POD 2 in both the SILA and CTLA groups. Based on this result, wound pain on POD 1 can be reduced by the careful handling of laparoscopic instruments during insertion through the umbilical wound in SILA. This may also facilitate an earlier recovery.
In this study, several parameters for the evaluation of postoperative recovery were compared between the two groups. There was significantly faster recovery to daily life in the SILA group than in the CTLA group (3.22±1.04 versus 3.94±1.43 days, P=.005). We think that the lower pain score on POD 1 may have contributed to this result because the absence of pain may contribute to a faster return to an oral diet and usual physical activity.
Many studies have reported that the most common postoperative complication is wound infection.14,17,23,27 Some authors reported that the SILA procedure caused more wound infections.28,29 One study reported a 3.3% postoperative wound infection rate in the SILA group compared with 1.7% in the CTLA group (P=.50). 23 In contrast, others have reported that wound infections are not more common in SILA than in CTLA.14,17,27 In our study, there were no wound infections in the SILA group, and 1 patient in the CTLA group developed a wound infection. We used a double-ringed wound retractor, and it might contribute to wound protection. In one study performed by a method similar to ours, there was only one wound infection in the SILA group. 27 The double-ringed wound retractor may be helpful for avoiding wound irritation during handling of laparoscopic instruments and may protect the wound from inflammation.
With respect to SILS, some authors have suggested that long-term complications, such as umbilical hernia, may result because the umbilical incision in SILS is larger than that in conventional multiport laparoscopic surgery. 23 Although we do not show the data here, none of the patients developed incisional hernias after about 2 years. We did not compare the patients' satisfaction regarding their wound between the two groups. The patients in the SILA group did not have the chance to compare their wounds with those developed from the other approach. To overcome this limitation, a larger sample study should be performed, and an appropriate method should be found to determine patients' satisfaction. However, SILA allows for scarless surgery.
In conclusion, the SILA procedure was technically feasible and safe, even in perforated appendicitis, and had some advantages over CTLA with respect to postoperative recovery. Overall SILA results in slightly less pain in the first 24 hours and a return to full activity ¾ of a day quicker when compared with CTLA. In addition, for perforated appendicitis, SILA seems to have a more pronounced advantage over CTLA with an almost 2 day shorter hospital stay and 3 day quicker return to full activity. To capitalize on these advantages, surgeons should continuously accumulate experience with laparoscopic surgery and perform the SILA procedure while carefully handling the laparoscopic instruments. We hope that the SILA procedure will become the good surgical option, as it is convenient for surgeons and satisfies patients' demands for earlier recovery and cosmesis.
Footnotes
Acknowledgments
Statistical analyses were supported by the Department of Statistics, School of Medicine, The Catholic University of Korea, Seoul, Korea.
Disclosure Statement
The manuscript is an original work and has not been submitted nor is it under consideration for publication in another journal. The study complies with current ethical considerations. We also confirm that all the listed authors have participated actively in the study and have read and approved the submitted manuscript. None of the authors have any possible conflicts of interest.