
Abstract
Abstract
Objective:
To report the feasibility of laparoscopic resection with intraoperative radiotherapy for local advanced rectal cancer in an Asian man.
Patient and Methods:
A 55-year-old man with adenocarcinoma of the rectum presented at Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China. The tumor, with a size of 5×5 cm, was located 3 cm from the anus and covered a circular area around approximately two-thirds of the bowel. The carcinoembryonic antigen level was 29.86 ng/mL; a nodule was detected, but no distant metastasis was detected. Preoperative staging was T4N1M0. After the patient signed the consent form, laparoscopic resection with intraoperative radiotherapy was performed.
Results:
The operation time was about 180 minutes, intraoperative blood loss was 100 mL, and postoperative hospital stay was 8 days. The patient had no postoperative complications.
Conclusions:
Performance of laparoscopic resection with intraoperative radiotherapy for local advanced rectal cancer is feasible in selected patients.
Introduction
For patients with mid or low rectal cancer, laparoscopic resection leads to a more satisfactory result and better life quality than other techniques. 3 Nowadays, laparoscopic surgery is changing to adopt several multivariate and less invasive ways, such as laparoendoscopic single-site with transanal natural orifice specimen extraction surgery and colorectal natural orifice translumenal endoscopic surgery (NOTES®). 4
Clinically, many patients with local advanced rectal cancer cannot afford the side effects of neoadjuvant therapy and have to wait for 4 more weeks before surgery. Intraoperative radiotherapy (IORT) is a useful and feasible therapeutic method during surgery to control many tumors. Although the IORT technique is a well-described procedure for rectal cancer, with some previous series evaluating the outcome after conservative rectal surgery reconstruction,5–9 only one previous report described the feasibility of the technique for patients subjected to laparoscopic TME. 10 Moreover, no information is available regarding its application in Asian people. Therefore, this study aimed to present the preliminary results of IORT application in an Asian patient undergoing laparoscopic TME. The pre- and intraoperative planning, advantages, limitations, and outcomes are further discussed.
Clinical Case and Methods
Preoperative preparation
A 55-year-old man with symptoms of bloody stools, constipation, and weight loss for 1 year was previously diagnosed with rectal cancer in Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China. His body mass index was 22 kg/m2, and he had no family history of cancer or other systemic diseases. Previous biopsy showed adenocarcinoma by colonoscopy. The tumor, with a size of 5 cm×5 cm, was located 3 cm from the anus and covered a circular area around approximately two-thirds of the bowel. The carcinoembryonic antigen level was 29.86 ng/mL. Pelvic magnetic resonance imaging showed lymph node metastasis, and no distant metastasis was detected by hepatobiliary ultrasound, chest x-ray, and abdomen and pelvis computed tomography scan; thus his preoperative staging was T4N1M0 and circumferential resection margin potential positive (Fig. 1). Laparoscopic rectal resection was planned to be performed on February 15, 2012 without preoperative radiotherapy.
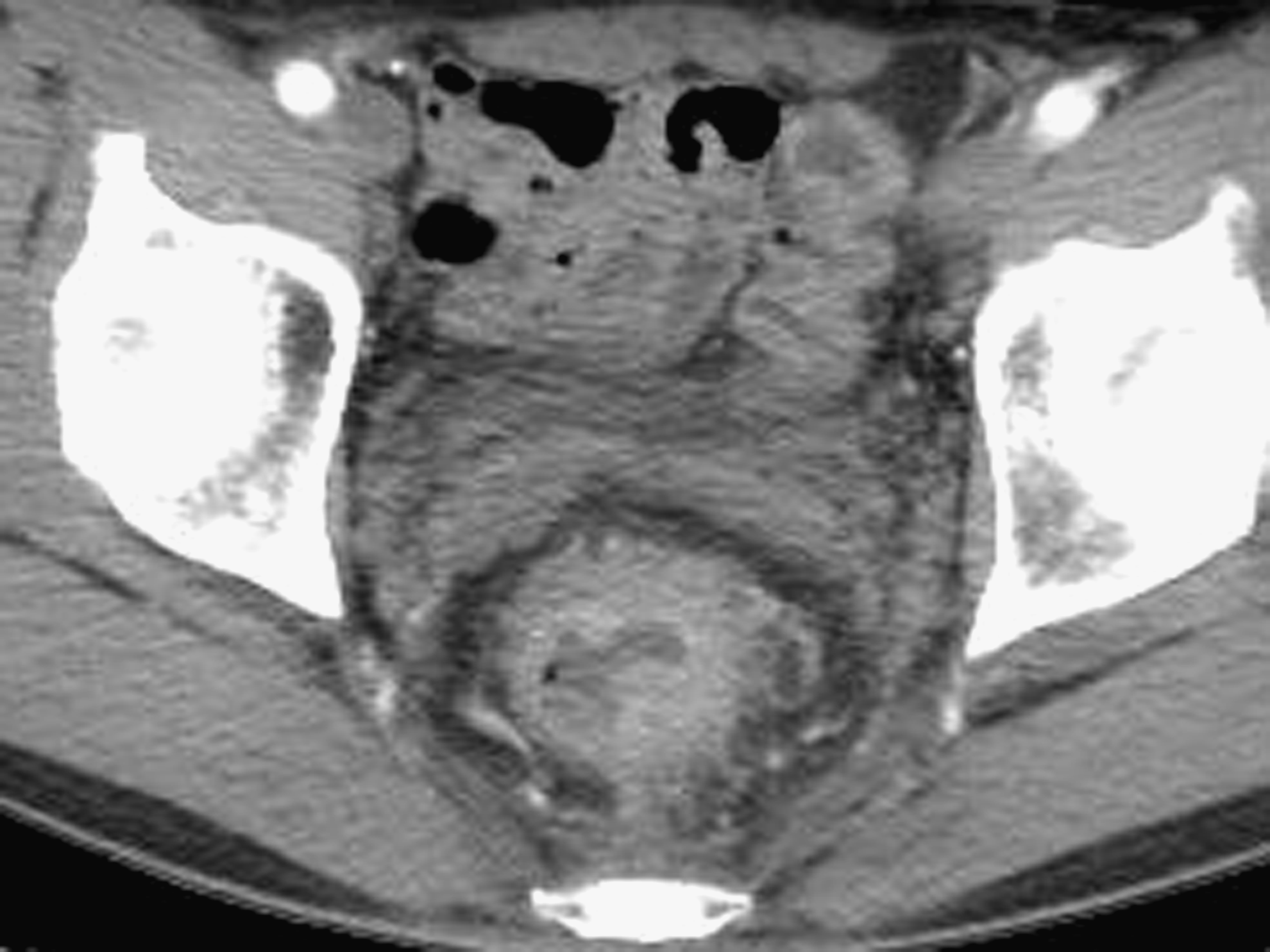
Magnetic resonance imaging showed the tumor occupied a circular area around approximately two-thirds of the bowel and broke the serous membrane with the lymph node observed.
Tumor resection
The patient was placed in the semilithotomy position with hip flexed (Trendelenburg position) for adequate exposure for the perineal approach. After insufflation of carbon dioxide pneumoperitoneum to a pressure of 14 mm Hg, the Veress needle was replaced with a 10-mm trocar for the Stryker 10 mm IDEAL EYES laparoscope in 45 cm length (model 502-457-030, 30° autoclavable laparoscope; Stryker, Kalamazoo, MI) just above the umbilicus. The remaining two 10-mm and two 5-mm trocars were placed under visual guidance. Inferior mesenteric vessel interruptions and detachment of the mesocolon were performed using the Harmonic® Ace system (model GEN300; Ethicon, a Johnson & Johnson Company, Blue Ash, OH). As soon as the dissection of the rectum was completed, the colon was sectioned through an Endo GIA™ (Covidien, Norwalk, CT), and then the in vitro phase began. The suprapubic port site was extended transversely (5 cm) depending on the size of the growth and IORT tube. The specimen was then removed through a protective sheath. The remaining tumor tissue was 1 cm in diameter and located in the left pelvic floor.
IORT technique
Immediately after the tumor resection, the tissue around the remaining tumor bed for about 2 cm was marked with six titanium clips as the radiotherapy area (Fig. 2). The lesion was seen more clearly under laparoscopy for its enlarged image and sharp details. The effective electron energy was subsequently chosen.

The view through the irradiation tube by laparoscopy. The target zone was marked by six titanium clips.
The Mobetron (IntraOp Medical Corp., Sunnyvale, CA), or mobile self-shielded electron linear accelerator unit, consisted of the treatment module, the modulation module, and the control module. The irradiation tube (round shape, 30°, 5 cm in diameter) was positioned directly over the tumor defect previously approximated (target zone) and then connected to the articulated arm of the linear accelerator (Figs. 3 and 4). Care was taken to avoid herniation of the small intestine into the irradiation tube to avert an increase in the dose delivered to the other part of the pelvis. Electron beam radiation was delivered with a dose of 10 Gy in 2 minutes (electron linear energy was 9 MeV, frequency was 1042 MU).

The irradiation tube was positioned with laparoscopic guidance.

The irradiation tube was connected to the articulated arm of the linear accelerator.
Bowel reconstruction
Pneumoperitoneum was reestablished. The bowel reconstruction was accomplished by a 33-mm circular stapler. A drainage tube was placed in the presacral region, and a terminal colostomy was created in the left iliac fossa (Fig. 5). We found a cauliflower-like tumor when the specimen was dissected (Fig. 6).

Trocar position, drainage tube position, and terminal colostomy position.

The tumor specimen has a negative distant resection margin but a positive circumferential resection margin.
Results
The total operative time was about 180 minutes: 90 minutes for laparoscopic TME, 10 minutes for marking the target area, 50 minutes of docking time, 2 minutes of console time, and 30 minutes for bowel reconstruction. The estimate blood loss was 100 mL, and no blood transfusion was required. Bowel function recovery and oral intake occurred in 4 days. The drainage tube and urethral catheter were removed within 7 days. The patient was discharged from the hospital within 8 days after surgery. No intraoperative or postoperative complication was found at 3 months' follow-up time.
Discussion
Despite increasing emphasis on screening and prevention, at least 5% of colorectal patients will present with locally “unresectable disease” and cannot receive laparoscopy resection (i.e., tumors fixed to critical structures or organs not amenable or appropriate for radical resection). 11 In such patients, incomplete resection alone or radiation therapy alone results in few long-term survivors.12,13 The patients who underwent R1 and R2 resections only survived 14 and 12 months after resection, 12 whereas those treated with primary “curative intent,” external beam radiotherapy have poor response rates, high rates of cancer recurrence, and overall 5-year survival rates of only 6%. 13 Given these poor outcomes, a multimodality regimen that includes maximal surgical resection, chemotherapy, and radiotherapy was used in patients with initially unresectable primary rectal cancer. Selected patients with advanced unresectable disease benefit from an aggressive approach. 14
Developed at the end of the 1990s, intraoperative radiation has been indicated for selected patients as an alternative to conventional external radiotherapy. Neoadjuvant administration of external beam radiotherapy has been recommended for patients with mid- or late-stage rectal cancer. 10 However, to eliminate its effects on observations during IORT, external beam radiotherapy was not involved in our multimodality approach. Doses ranging up to 25 Gy can generally be tolerated without significant toxicity. 15 The Mayo Clinic uses a dose of 7.5–10 Gy when the resection margin is negative, 10–12.5 Gy when the resection margin is microscopically positive, 15 Gy when the residual tumor is ≤2 cm, 17.5–20 Gy when the residual tumor is >2 cm, and 45–55 Gy as preoperative or postoperative external radiotherapy. 16 According to these results, we planned 10 Gy and postoperative radiochemotherapy for the patient.
To eliminate the risk of radiation on adjacent normal tissues is quite important during IORT. After tumor resection, the pelvic cavity was big enough to place the collimator. During IORT, the patient was placed in the head-down lithotomy position to push the bowel out of the pelvic cavity. In our study, we used the Richardson retractor to grasp the abdominal wall, and a pseudo-pneumoperitoneum was created. Afterward, to prevent the small bowel from getting into the radiation field, laparoscopic instruments (such as bowel clamp) were used if small bowel obstruction occurred. In addition, by using the mobile self-shielded electron linear accelerator unit, a high dose of radiation could be delivered mechanically to the specific tumor bed region, while the adjacent tissues (such as small bowel) were not affected.
The operative time was shorter than that of Civello et al. 10 Before the introduction of the mobile self-shielded electron linear accelerator unit, most patients were transported from the operating room to the radiation therapy department to receive their IORT treatment. After the treatments, they were then returned to the operating room for the completion of the surgery. The transport between the surgery and radiation departments not only was inefficient, but also increased the time of the operation and the time the patient must be under anesthesia, and it carried a higher risk for infection because the patient with an open wound was transported out of a sterile environment for the IORT treatment. The bowel function recovery time, oral intake time, and discharge time were similar to those in the previous report. 10
Despite the good result observed, some IORT-related complications have been reported, such as anastomotic leakage, delay of cicatrization, and infections. 17 Additionally, because the immediate application of IORT involves rearrangement of pelvic tissue, the technique may jeopardize the postoperative rectal radiation dose delivery. However, these did not occur in our study. Under laparoscopy, we can clearly distinguish the target zone from normal tissue, thus protecting the small bowel and anastomotic bowel from radiation.
The initial data showed that laparoscopic resection with IORT is feasible. The important concern of this technique is the accuracy of tumor resection. The mobile self-shielded electron linear accelerator unit enables a high dose of radiation be delivered mechanically to the specific tumor bed region, while the adjacent tissues (such as small bowel) were not affected. With appropriate patient selection, respecting its indication and limitations, this type of therapy can benefit the management of “unresectable” rectal cancer. Nevertheless, further studies including larger clinical series and longer follow-up periods are still necessary to successfully treat rectal tumors.
Footnotes
Acknowledgments
This report was compiled and written by a multidepartment group. Although the primary contributors are listed, we would like to thank all those who contributed to this case through their input and assistance. Thanks to International Center of Papertrans (![]() ) for the composition and revision for the manuscript.
) for the composition and revision for the manuscript.
Disclosure Statement
No competing financial interests exist.