
Abstract
Abstract
Background:
In this article we report our initial clinical experience about umbilical single-incision laparoscopic surgery (SILS) radical gastrectomy with D2 lymph node dissection for early gastric cancer with conventional laparoscopic instruments.
Subjects and Methods:
Preliminary experiences with umbilical SILS radical gastrectomy in 4 patients with early gastric cancer were described.
Results:
Umbilical SILS radical gastrectomy with D2 lymph node dissection was performed successfully with conventional laparoscopic instruments in these 4 patients. Average operative time was 280 minutes, and average blood loss was 162 mL. No intraoperative or postoperative complications, such as secondary hemorrhage, anastomotic leakage, or obstruction, were recorded. The patients recovered fully, and the single umbilical scar was well healed.
Conclusions:
Our initial experience showed that transumbilical SILS radical gastrectomy with D2 lymph node dissection for early gastric cancer is feasible and safe when performed by experienced laparoscopic surgeons.
Introduction
Patients and Methods
Patients
Four patients (three women and one man) underwent single-incision laparoscopic distal gastrectomy with D2 lymph node dissection from February 2010 to September 2011 at our center, with a mean age of 56 years (range, 47–68 years). The diagnosis was confirmed by gastroscopy and pathology, and the extent of disease was estimated by ultrasonic endoscopy and enhanced computed tomography preoperatively. The lesions were limited within the submucosum and lower third of the stomach; there was no metastasis of carcinoma in these patients. Informed consent was obtained preoperatively, and its associated risks were explained to the patient and the responsible next of kin.
Technique
After induction of general endotracheal anesthesia, the patient was placed in a supine posture with legs apart. The laparoscopic equipment and the monitor were placed above the patient's left shoulder. The surgeon stood between the patient's legs, while the first assistant stood on the patient's right side. A superficial incision 2–3 cm long was made vertically within the patient's umbilical fold into which a 10-mm trocar was inserted at the 6 o'clock position for the 10-mm videolaparoscope, a 12-mm trocar on the 2 o'clock position for the right-handed instruments and the Endo GIA™ stapler (Covidien), and a 5-mm trocar at the 10 o'clock position, so that the three trocars formed an inverted equilateral triangle about 10 mm apart on each side.
The procedure for lymph node dissection is similar to that for conventional laparoscopic gastrectomy. The liver needs to be suspended from the diaphragm by the adhesion of tissue glue sprayed on the diaphragmatic surface of the liver instead of standard laparoscopic forceps operated by an assistant or other retractors puncturing the abdominal wall
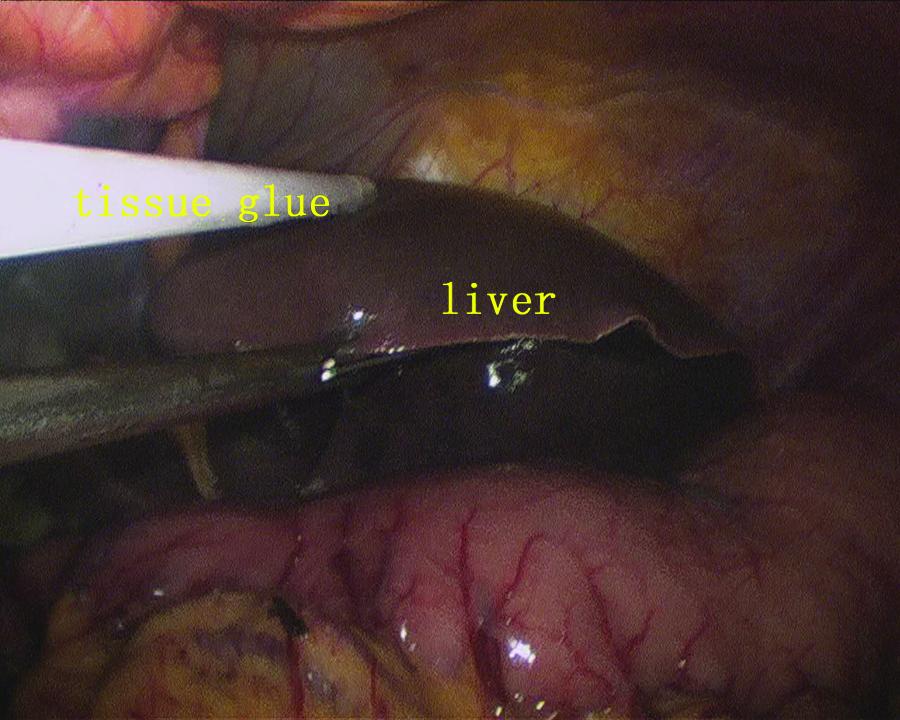
The liver was suspended from the diaphragm by the adhesion of tissue glue sprayed on the diaphragmatic surface of the liver.

The right gastroepiploic vein was divided at the base to allow dissection of lymph node 6.
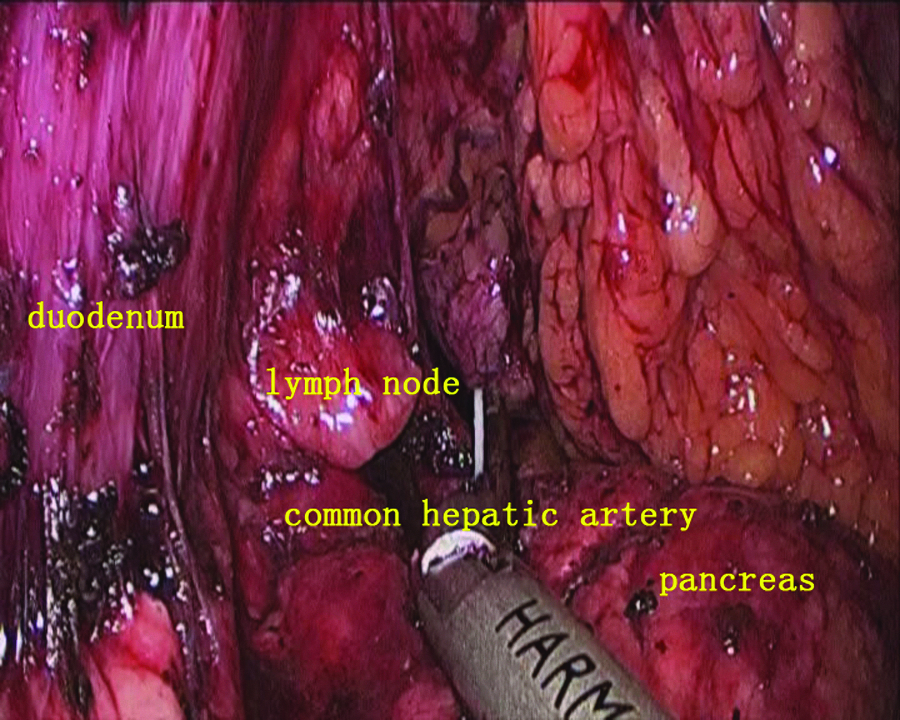
With the stomach lifted posteriorly by the atraumatic grasper in the left hand, dissection was continued along the gastroduodenal artery, and the common hepatic artery was exposed.
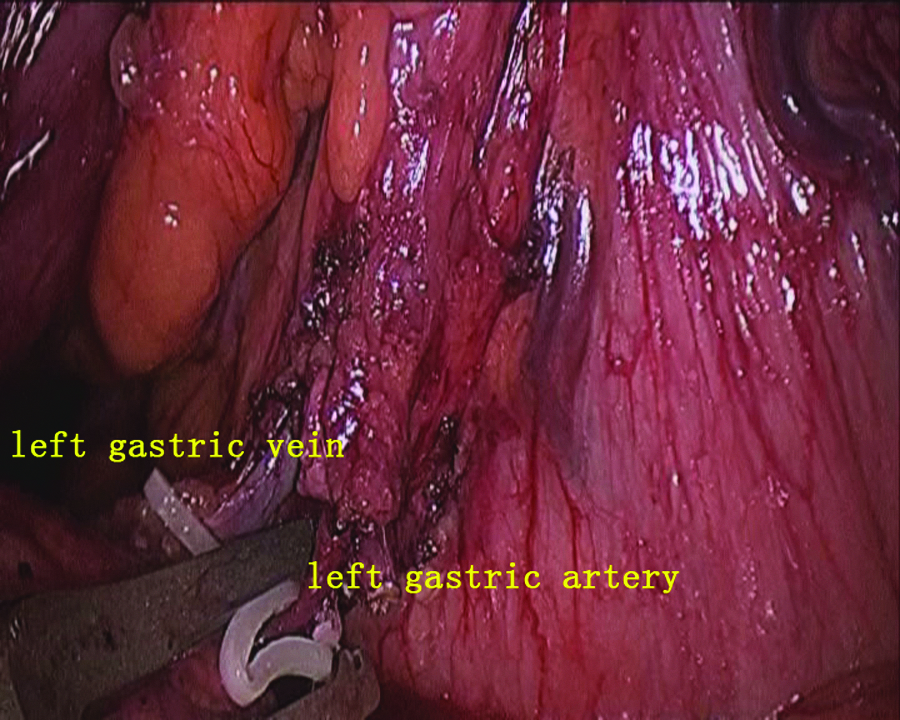
The left gastric artery and vein were saved at their origin.
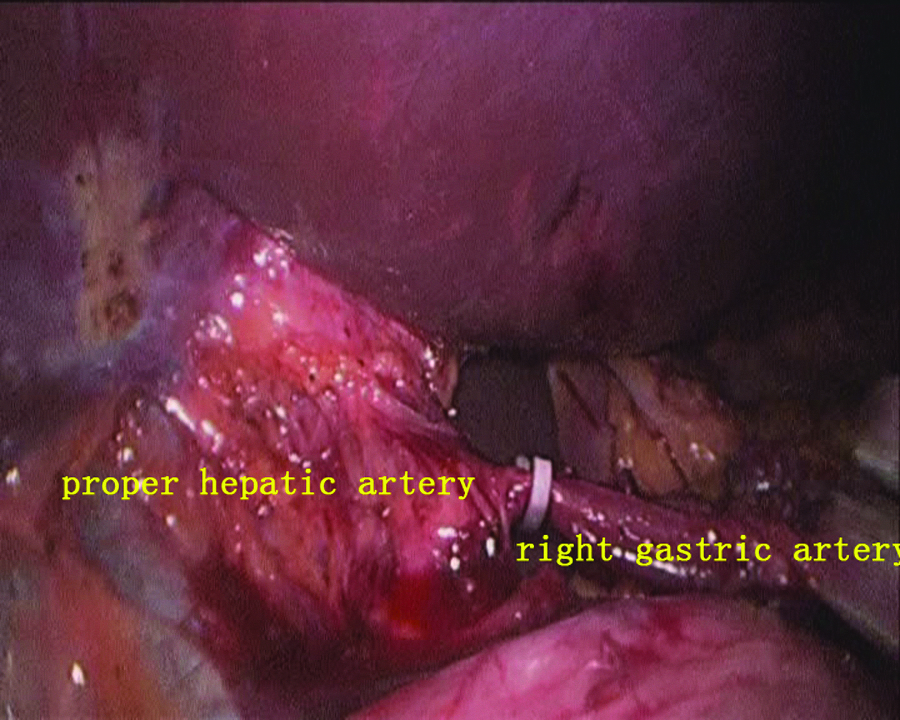
The proper hepatic artery and the right gastric vessels were identified for lymph nodes 12a and 5 dissected in front of the stomach, and the right gastric artery was divided at the root.
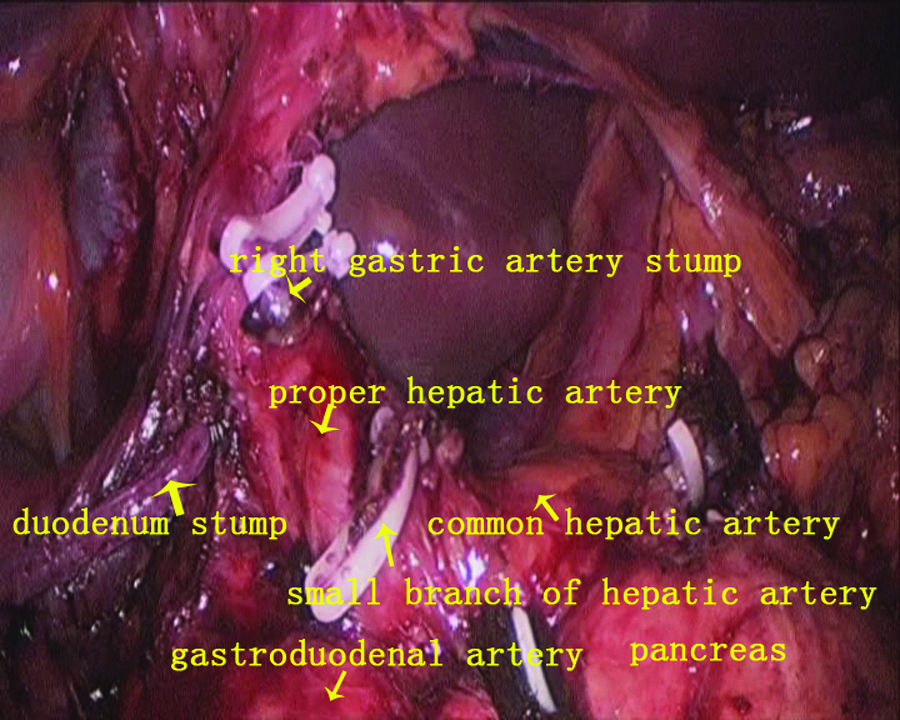
The procedure for lymph node dissection was completed.
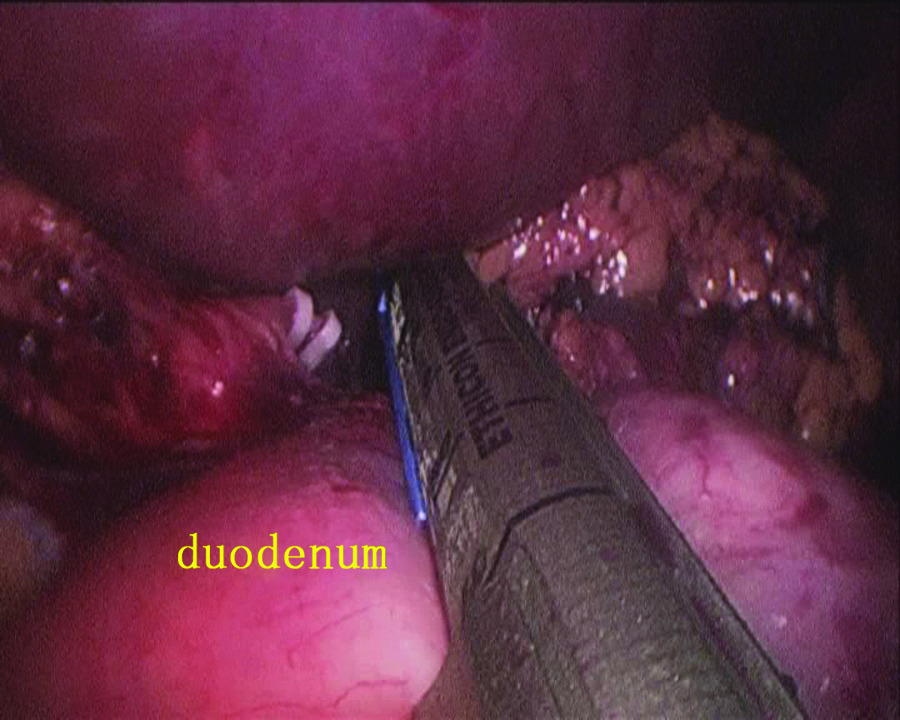
The duodenum was transected just distal to the pyloric ring by using linear staplers.
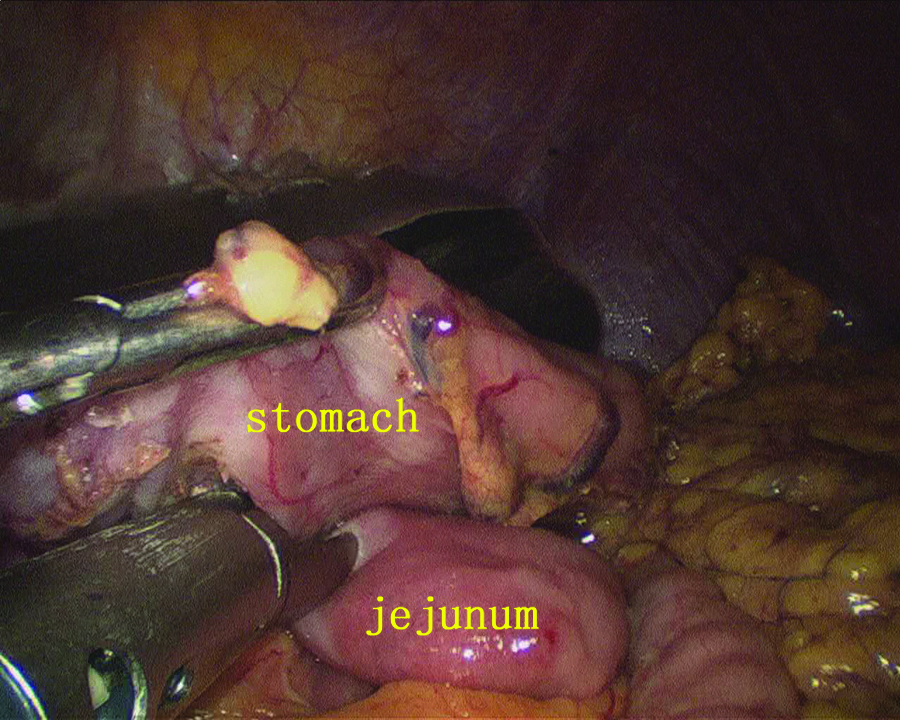
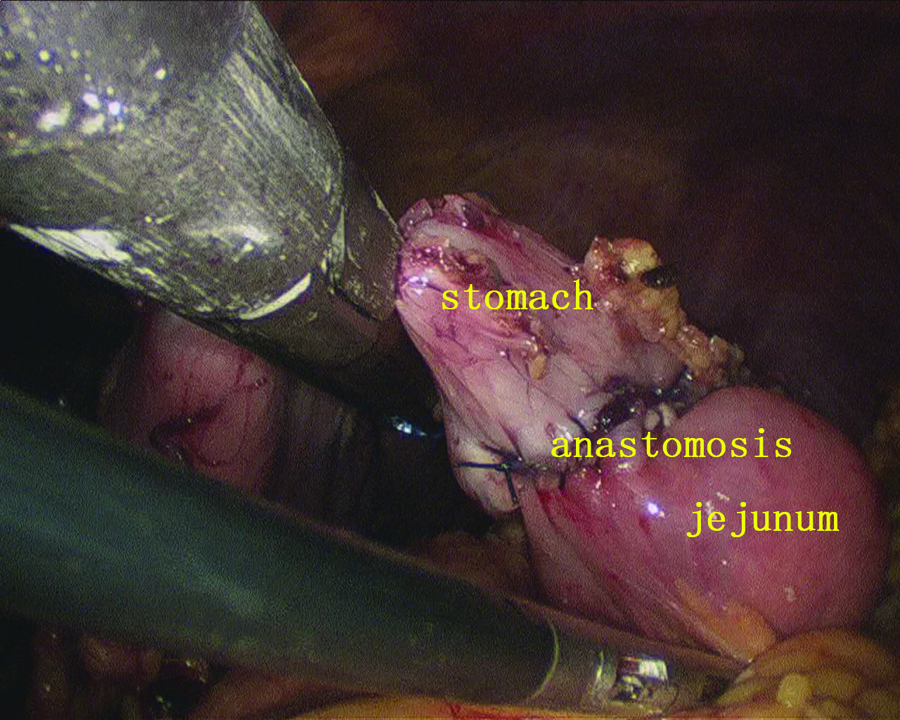
After step-by-step insertion of the linear stapler forks, the posterior wall of the stomach and the antimesenteric side of the jejunum were put together, and an anastomosis was made with the linear stapler.
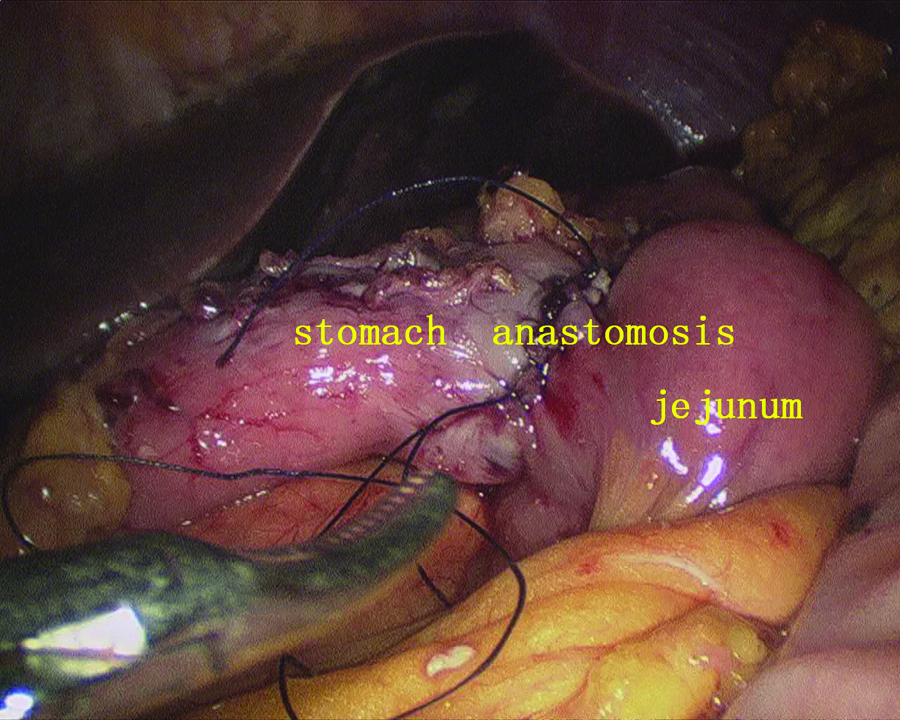
The common incision was closed by a running suture with 3-0 absorbable suture.
The stomach was transected at least 5 cm distal from the lesion by using linear staplers.
Results
Single-incision laparoscopic distal gastrectomy with D2 lymph node dissection has been performed successfully in 4 patients with early gastric cancer. No serious intraoperative and postoperative complications were observed. The median operative time was 280 minutes (range, 250–310 minutes). The median estimated blood loss was 162 mL (range, 100–200 mL). The postoperative pathology confirmed a tumor located in the mucosa in 1 case and in the submucosa in 3 cases. The sizes of the tumor were 1, 2, 4.5, and 1.0 cm, respectively. The margin was negative for tumor cells. The median number of retrieved lymph nodes was 16 (range, 12–21); only 1 of them was metastasized, whereas the others had no lymphatic metastasis.
All the patients recovered quickly after the surgery. They were allowed to consume liquids with the intestinal peristalsis recovery. No major complications such as anastomotic leakage, stenosis, or bleeding were observed. The mean postoperative hospital stay was 13 days. These 4 patients have been followed up for 6–24 months. There has been no tumor recurrence or distant metastasis, and the umbilical wounds were healing well.
Discussion
Since 1999, when Uyama et al. 2 first reported laparoscopic D2 radical gastrectomy for advanced gastric cancer, laparoscopic radical gastrectomy for gastric cancer has been accepted worldwide by surgeons. Although the radical nature and safety of laparoscopic tumor resection are controversial, some retrospective studies have confirmed that laparoscopic operation can achieve the same effect as open operation.3–5 Even in the matter of postoperative hospital stay, infection of the incision, and postoperative complications, laparoscopic operation is superior to the traditional operation.6–9
With the popularization and development of laparoscopic technology, the application of transumbilical single-port laparoscopic operation has become the current clinical research hot topic. The postoperative cosmesis is excellent because the umbilical wound can be hidden inside the umbilicus in SILS, and it meets the needs of patients for cosmesis. Its first application in gastric operation was reported in 2003 by Lee et al., 10 who completed the endoscopic staging of gastric cancer by using the single-port laparoscopic technique. This was followed by some reports about gastrostomy, gastric reduction, and partial gastrectomy for gastric stromal tumor.11–16 In 2011 Omori et al. 17 first reported their initial clinical experience with single-incision laparoscopic gastrectomy with lymphadenectomy for early gastric cancer without the use of additional trocars or conversion to laparotomy. Their experience showed that single-incision laparoscopic distal gastrectomy is a feasible and safe procedure for early gastric cancer and gives a favorable cosmetic result. Lee et al. 18 compared the perioperative outcomes of single-incision laparoscopic distal gastrectomy and conventional laparoscopic distal gastrectomy by using a porcine model with gastric cancer. The model pigs were subjected to the same distal gastrectomy with D1+b lymph node dissection. The single-incision laparoscopic group was associated with a significantly longer operation time, but it had a similar mean number of resected lymph nodes. Their animal study showed that the single-incision laparoscopic group can be applicable for treating gastric cancer with similar inflammatory reaction and complication rates compared with the conventional laparoscopic procedure. A recent meta-analysis demonstrated that single-incision laparoscopic cholecystectomy is a safe procedure for the treatment of uncomplicated gallstone disease, with postoperative outcome similar to that of standard multiport laparoscopic cholecystectomy. 19 The operative time and hospital stay are a little bit longer because this procedure is still in its initial stage. According to our experience with single-port laparoscopic surgery in other fields, these data will improve after the learning curve is set up.
Up to now we have completed transumbilical single-port laparoscopic radical gastrectomy with D2 lymph node for early gastric cancer in 4 patients. No serious perioperative complications occurred, and no mortalities were observed in this case series. The median operative time was longer owing to the difficult operation with the transumbilical single port. The following limitations were observed. First, insertion of the laparoscope and instruments through the same single incision resulted in a conflict of instruments. Second, only one auxiliary operating channel meant there was a lack of operative field exposure with assistance. Third, the surgery was achieved with the surgeon's independent operation; retraction with one hand made it difficult to achieve the tension between the tissues and affected the anatomy speed of the ultrasonic scalpel. Fourth, insertion of the instruments through the single incision decreased the range of motion, resulting in significant difficulty in suturing and knotting. Fifth, adequate lymph node dissection is a complex and highly difficult operation in radical gastrectomy with gastric cancer.
In order to overcome these difficulties, we adopted the following measures: First, the patient was fixed well on the table during the operation, and gravity helped the exposure of the operation field through adjustment of the patient's position. Second, the liver needs to be suspended from the diaphragm by the adhesion of tissue glue sprayed on the diaphragmatic surface of the liver to expose the fundus and lesser curvature. Third, endoscopic linear staplers were used to complete the gastrointestinal disarticulation and reconstruction and to minimize the manual suture as much as possible. Also, Hem-o-lok® clips (Teleflex) are very useful for treating large vessels securely and conveniently. Fourth, when suturing must be done, such as in gastrointestinal residual anastomosis, continuous suturing with an absorbable 3-0 suture with a needle and single-handed knotting was helpful. When the single hand knotting technique was performed, we made a ring with one end of the line by one instrument and then used the same instrument to catch the other end of the line through the ring to complete the knot. Fifth, the accumulation of experience with conventional laparoscopic radical gastrectomy for gastric cancer and the familiarity with the anatomy were useful. Sixth, large numbers of transumbilical single-port laparoscopic cholecystectomy and other SILS operations were conducive to strengthen the cooperation between the surgeon and the assistant holding the mirror.
In conclusion, our initial experience with single-incision laparoscopic radical gastrectomy with D2 lymph node dissection for early gastric cancer is feasible and safe when performed by experienced laparoscopic surgeons. As a result of the small number of cases and the short observation time in this group, further expansion of the number of the case and extension of the follow-up time to determine the benefits of this new minimally invasive technique are still needed.
Footnotes
Disclosure Statement
No competing financial interests exist.