
Abstract
Abstract
Background:
Pancreatoduodenectomy is an established procedure for the treatment of benign and malignant diseases located at the pancreatic head and periampullary region. In order to decrease morbidity and mortality, we devised a unique technique using two different jejunal loops to avoid activation of pancreatic juice by biliary secretion and therefore reduce the severity of pancreatic fistula. This technique has been used for open pancreatoduodenectomy worldwide but to date has never been described for laparoscopic pancreatoduodenectomy. This article reports the technique of laparoscopic pylorus-preserving pancreatoduodenectomy with two jejunal loops for reconstruction of the alimentary tract.
Materials and Methods:
After pancreatic head resection, retrocolic end-to-side pancreaticojejunostomy with duct-to-mucosa anastomosis is performed. The jejunal loop is divided with a stapler, and side-to-side jejunojejunostomy is performed with the stapler, leaving a 40-cm jejunal loop for retrocolic hepaticojejunostomy. Finally, end-to-side duodenojejunostomy is performed in an antecolic fashion.
Results:
This technique has been successfully used in 3 consecutive patients with pancreatic head tumors: 2 patients underwent hand-assisted laparoscopic pylorus-preserving pancreatoduodenectomy, and 1 patient underwent totally laparoscopic pylorus-preserving pancreatoduodenectomy. One patient presented a Grade A pancreatic fistula that was managed conservatively. One patient received blood transfusion. Mean operative time was 9 hours. Mean hospital stay was 7 days. No postoperative mortality was observed.
Conclusions:
Laparoscopic pylorus-preserving pancreatoduodenectomy with double jejunal loop reconstruction is feasible and may be useful to decrease morbidity and mortality after pancreatoduodenectomy. This operation is challenging and may be reserved for highly skilled laparoscopic surgeons.
Introduction
In order to decrease morbidity and mortality rates after PD, we devised a unique technique using two different jejunal loops for hepatico- and pancreaticojejunostomy. 4 Indeed, the adoption of this technique in our surgical service significantly decreased the complication rates in our patients. These findings were subsequently confirmed by several authors.5–8 In recent years, some modifications of the original technique, using an isolated jejunal loop for pancreatojejunostomy, have been published and also showed a reduced rate of pancreatic fistulas.9–11 The sole prospective trial published so far favored double jejunal loop reconstruction. 5 In the last 5 years, 287 of our patients underwent open pylorus-preserving PD with 17.8% developing a pancreatic fistula and no mortality (authors' unpublished data). Most pancreatic fistulas were Grade A.
Since the publication of the original technique in 1976, several modifications of PD have been published, such as pylorus-preserving PD, portal vein resection, and minimally invasive techniques for PD. This aim of this article is to report our technique of laparoscopic pylorus-preserving PD with emphasis on the use of two jejunal loops for reconstruction of the alimentary tract.
Operative Technique
The patient is placed in a supine position with the surgeon standing between the patient's legs. Using an open technique, a 10-mm trocar is placed above the umbilicus; through this port, a 10-mm 30° angled laparoscope is introduced. Pneumoperitoneum is established at a pressure of 12 mm Hg. Once examination of the abdominal cavity confirms the absence of peritoneal metastases, four additional trocars are inserted. One 12-mm trocar is placed on the left midclavicular line about 5 cm above the umbilicus for the surgeon's right hand. A 5-mm port is placed in the subxiphoid position and is used for retraction, another 5-mm trocar is inserted on the right midclavicular line, and finally one 5-mm trocar is placed on the right flank. Two cases were performed using hand assistance. In those cases, the two right-sided trocars are replaced by a 7-cm transversal incision made in the right upper quadrant and used for the hand port (surgeon's left hand) with GelPort® (Applied Medical, Rancho Santa Margarita, CA).
Pylorus-preserving PD
The operation begins with the opening of the retrocavity and exposure of the body of the pancreas. The Kocher maneuver is performed with upper traction of the duodenum. After division of the gastroepiploic vessels, the duodenum is transected 2–4 cm below the pylorus using an endoscopic linear stapler. The stomach is then moved to the left upper quadrant. The next step is to perform hepatic hilum dissection. Cholecystectomy is performed, and the common bile duct is dissected and divided. The proximal bile duct is maintained closed with a detachable vascular clamp. The hepatoduodenal ligament is then skeletonized. The gastroduodenal artery is safely divided, and the portal vein is exposed. A tunnel is carefully created behind the neck of the pancreas at the level of the superior mesenteric and portal vein using a right-angle instrument and blunt dissection. The pancreas is then divided with an endoscopic vascular stapler. The jejunum is divided with the stapler 20 cm distal to the ligament of Treitz. Finally, the uncinate process is carefully dissected from the superior mesenteric vein and artery. PD is completed.
Reconstruction of the alimentary tract with a double jejunal loop
Reconstruction of the alimentary tract is performed using the double jejunal loop technique 4 (Fig. 1). First, a double-layered retrocolic end-to-side pancreaticojejunostomy is performed with duct-to-mucosa anastomosis using interrupted nonabsorbable monofilament sutures and a second layer between the jejunal seromuscular and pancreatic tissue to reinforce the anastomosis (Fig. 2a and b). Second, the jejunal loop is divided with the stapler, and a side-to-side jejunojejunostomy is performed with the stapler, leaving a 40-cm jejunal loop for the hepaticojejunostomy. Next, the detachable vascular clamp is removed, and an end-to-side retrocolic hepaticojejunostomy is performed with a running absorbable suture, using a previously published technique. 12 A posterior running suture is performed without opening of the jejunum. The jejunum is then opened, and the posterior layer is completed with a reversal running suture (Fig. 2c and d). Finally, an end-to-side duodenojejunal anastomosis is performed using the standard double-layer technique in an antecolic fashion. Two drains—one for pancreaticojejunostomy and other for hepaticojejunostomy—are left in place and exteriorized on the left and right flank, respectively.
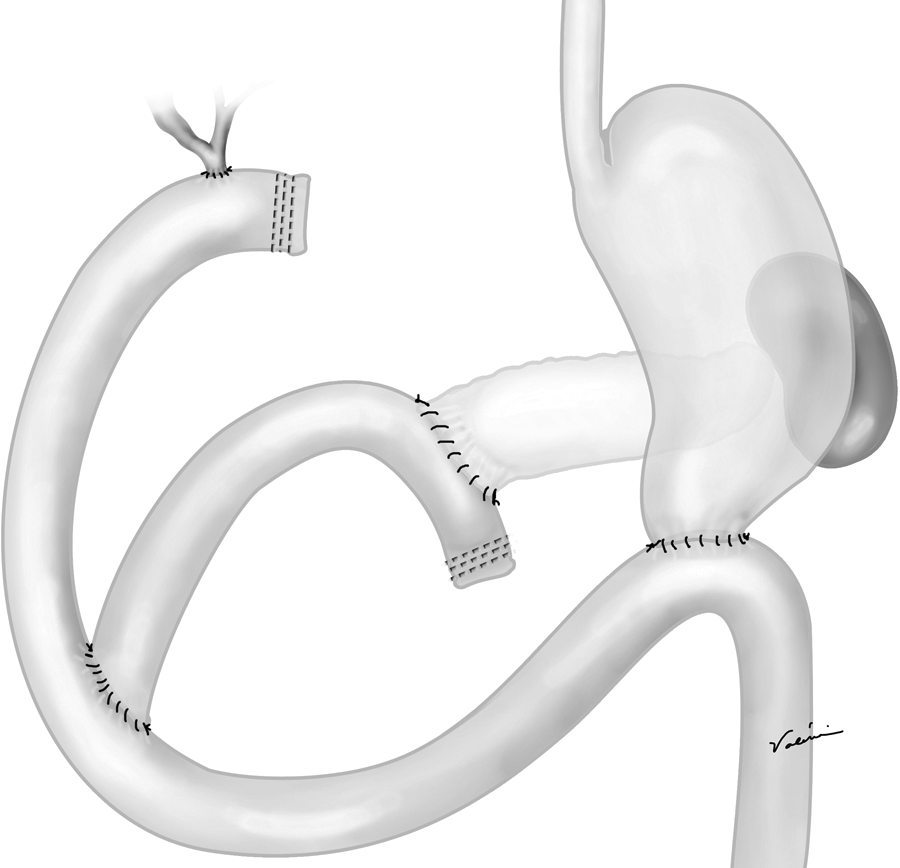
Schematic drawing of the double jejunal loop technique for reconstruction of the alimentary tract after laparoscopic pylorus-preserving pancreatoduodenectomy.
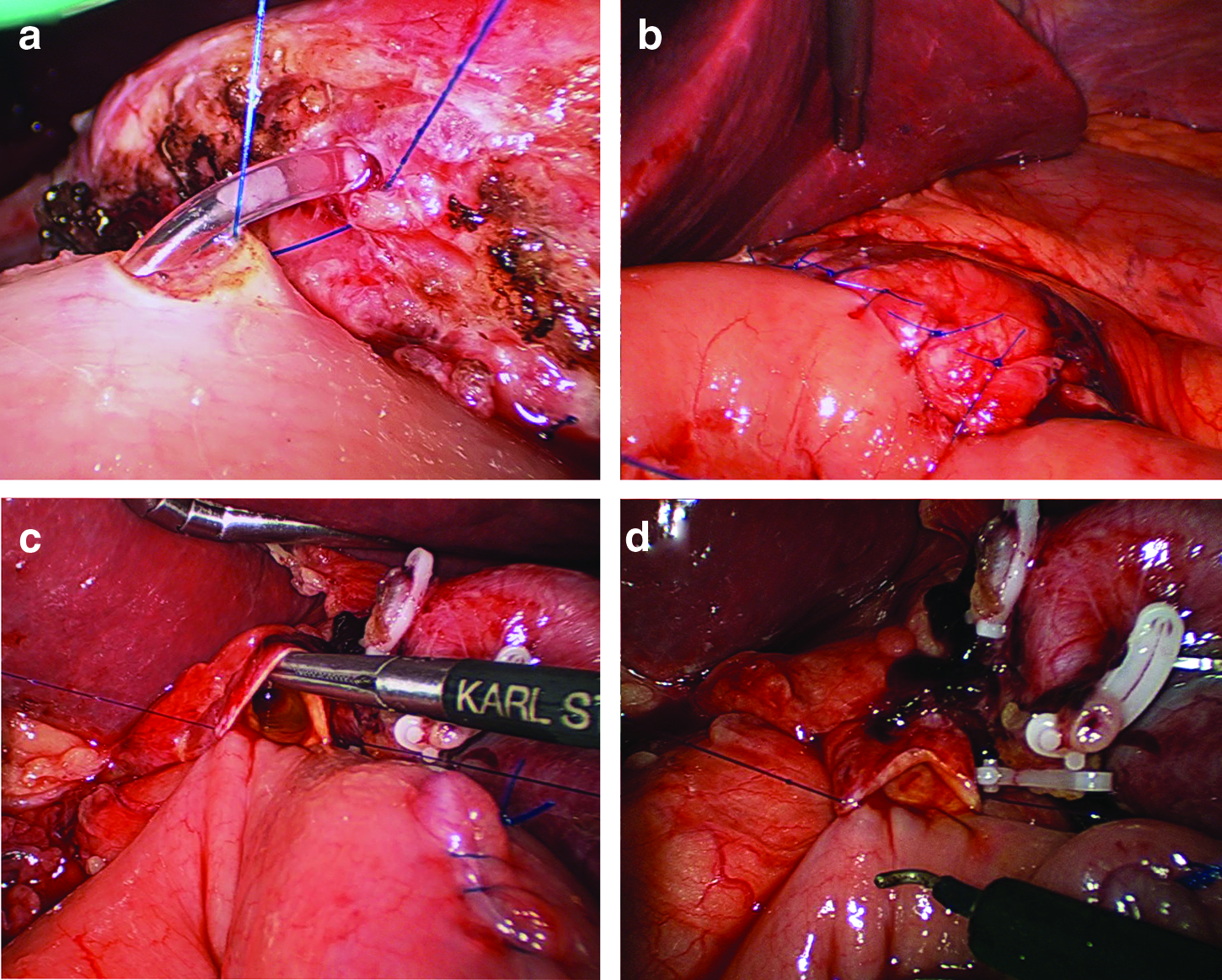
Reconstruction after laparoscopic pancreatoduodenectomy.
The surgical specimen was removed by an extended umbilical incision in 1 case and through the hand port in 2 cases.
Results
This technique has been successfully used in 3 consecutive patients with pancreatic head tumors. A 75-year-old man with adenocarcinoma of the pancreas and a 58-year-old woman with intraductal papillary-mucinous neoplasm underwent hand-assisted laparoscopic pylorus-preserving PD with the double jejunal loop technique. A 63-year-old woman with a neuroendocrine tumor underwent totally laparoscopic pylorus-preserving PD with the double jejunal loop technique. The pathologic surgical margins were free in all cases. Operative time for the hand-assisted operation was 9 and 8 hours, and hospital stay was 10 and 6 days, respectively. The totally laparoscopic operation took 10 hours, and the patient was discharged on postoperative Day 5. Blood loss was minimal in 2 cases with no need for transfusion. One patient (the hand-assisted case) had blood loss of 800 mL and needed a transfusion (2 units). The first patient developed a Grade A pancreatic fistula that was managed conservatively. No postoperative mortality was observed. All patients are well in a mean follow-up of 4 months. One patient with adenocarcinoma is currently receiving systemic chemotherapy.
Discussion
The first laparoscopic PD was performed in 1992 and published in 1994 by Gagner and Pomp. 13 Since then, given the difficulty level of the procedure, relatively few laparoscopic PDs have been performed. However, there is a growing interest in this type of surgery, and the number of procedures is rapidly increasing. In a recent review of all published cases, 285 cases were found. 14 According to this review, overall mortality was 2%, and the morbidity rate was 48%.
Pancreatic fistulas from pancreatic anastomosis are the most common factor responsible for the high morbidity and mortality after both open and laparoscopic PD.14–17 To reduce the incidence and complications of these anastomosis, several techniques such as pancreatogastrostomy, duct-to-mucosa anastomosis, or binding pancreaticojejunostomy or use of octreotide have been studied; however, no advantages have been shown in any of these technique.17–23
Most of the reports related to pancreatic fistula are dealing with a technique aimed to decrease the incidence and not the severity of this complication. Pancreatic juice is secreted in an inactivated state, being activated into the bowel lumen mainly by biliary secretion. In patients with combined biliary and pancreatic fistulas, mortality was virtually 100%. 3 Using a single jejunal loop for the reconstruction of pancreatic and biliary tracts may predispose to the leakage of pancreatic anastomosis by activation of proteolytic enzymes and consequent tissue damage. Separation of the biliary and pancreatic conduits may decrease the incidence and the severity of pancreatic fistulas, therefore reducing the morbidity and mortality of PD.4–8 An additional advantage of this type of alimentary reconstruction is related to the need of reoperation due to stenosis of biliary or pancreatic anastomosis. Reoperation is much easier and safer when separate loops have been used for biliary and pancreatic anastomosis. Another potential advantage of the particular reconstruction described herein is the reduction of marginal ulceration. Having bile and pancreatic juice in the jejunum where the duodenojejunostomy is performed may reduce the incidence of marginal ulceration. One similar technique puts both the pancreatic and biliary anastomoses on one jejunal loop and the duodenal anastomosis on a separated Roux, which may cause marginal ulceration. 9
With our increasing experience with advanced laparoscopic surgery, more complex pancreatic resections, such as PD, have been included in our armamentarium. However, our results with open PD were excellent, and we did not see much room for improving. Our current technique includes pylorus-preserving PD with duct-to-mucosa double-layer pancreaticojejunostomy and double jejunal loop reconstruction. The worldwide initial experience with laparoscopic PD showed a great variety of techniques for easier resections and reconstructions to the detriment of pylorus-preserving and duct-to-mucosa pancreaticojejunostomy.14,16 These modifications were mainly due to technical difficulties rather than choice. Our choice was not to change our technique but to improve skills and perform surgery with the same technique used for open PD. With greater experience several laparoscopic pancreatic surgeons have improved their technique. However, the use of double jejunal loops for laparoscopic PD has not been described so far.
With the increased use of minimally invasive techniques in resection of the pancreatic head, we will expect the use of different methods for reconstruction of the alimentary tract. Our extensive experience with double jejunal loop reconstruction after open PD stimulated us to use the same technique with the laparoscopic approach. The construction of two different loops for each pancreatic and biliary reconstruction may seem tedious and time-consuming. However, the advantage of the technique, especially in small pancreatic duct and soft gland, justifies its use. Moreover, with the availability of staplers in laparoscopic surgery, the construction of two different loops did not significantly increased the operation time in our preliminary experience (6 cases).
In conclusion, laparoscopic pylorus-preserving PD with double jejunal loop reconstruction is feasible and may be useful to decrease severity of postoperative pancreatic fistulas. This operation remains technically demanding and challenging and may be reserved for highly skilled laparoscopic surgeons.
Footnotes
Disclosure Statement
No competing financial interests exist.