
Abstract
Abstract
Background:
Surgical resection is the only curative treatment for hilar cholangiocarcinoma. Laparoscopic hepatectomy has been used to treat several types of liver neoplasms. However, technical issues have limited the adoption of laparoscopy for the treatment of hilar cholangiocarcinoma. To date there is only one report of minimally invasive procedure for hilar cholangiocarcinoma in the literature. The present video-assisted procedure shows a laparoscopic resection of hilar cholangiocarcinoma.
Patient and Methods:
A 43-year-old woman with progressive jaundice due to left-sided hilar cholangiocarcinoma was referred for treatment. The decision was to perform a laparoscopic left hepatectomy with lymphadenectomy and resection of extrahepatic bile ducts. Biliary reconstruction was performed using the hybrid method.
Results:
Operative time was 300 minutes with minimum blood loss and no need for blood transfusion. Recovery was uneventful, and the patient was discharged on postoperative Day 7. Pathology revealed a well-differentiated cholangiocarcinoma with negative lymph nodes and clear surgical margins. The patient is well with no signs of the disease 18 months after the procedure.
Conclusions:
Laparoscopic left hepatectomy with lymphadenectomy is safe and feasible in selected patients and when performed by surgeons with expertise in liver surgery and minimally invasive techniques. The use of a hybrid method may be needed for biliary reconstruction, especially in cases where position and size of remnant bile ducts may jeopardize the anastomosis. Further studies are still needed to confirm the benefit of this approach over conventional surgery for hilar cholangiocarcinoma.
Introduction
Patient and Methods
A 43-year-old woman with progressive jaundice due to left-sided hilar cholangiocarcinoma was referred for surgical treatment. Preoperative magnetic resonance imaging disclosed a left-sided Klatskin's tumor with atrophy of the left liver and adequate future liver remnant (Fig. 1a and b). The decision was to perform a left hepatectomy with lymphadenectomy and resection of extrahepatic bile ducts. Preoperative percutaneous biliary drainage was not performed given the excellent performance status of the patient, adequate volume of the future liver remnant, and serum bilirubin level being only slightly elevated.
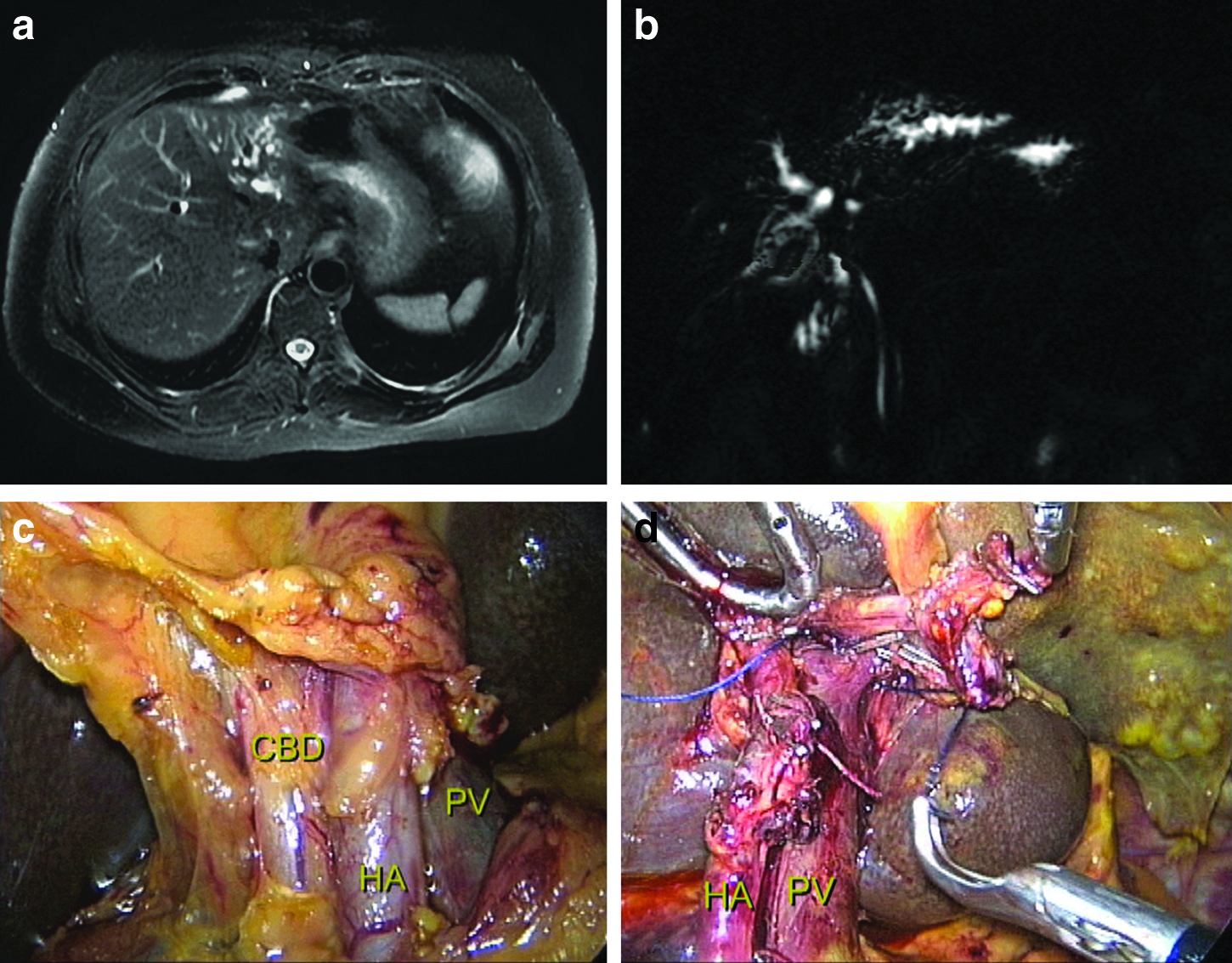
Laparoscopic resection of hilar cholangiocarcinoma.
The patient was placed in a supine position with the surgeon standing between the patient's legs. This technique uses five trocars; the type and location of trocars are described elsewhere. 11 Pneumoperitoneum was established at a pressure of 12 mm Hg.
At laparoscopy, left liver atrophy was evident. The first step was to fully mobilize the left liver. This was accomplished by transecting the round ligament, followed by division of the falciform, coronary, and left triangular ligaments. The left lobe was pulled upward, and the lesser omentum was divided, exposing the Arantius ligament (ligamentum venosum) and the caudate lobe. A laparoscopic 5-mm snake liver retractor was introduced by the epigastric port, and it was used for upward liver retraction and exposure of the hepatic hilum. Extensive hilar lymphadenectomy was performed. Dissection of hepatic hilum was carefully performed, exposing the anterior surface of the common bile duct, common hepatic artery, and portal vein (Fig. 1c).
The hepatic artery was dissected and encircled. The same maneuver was done with the common bile duct. As the dissection progressed, the hepatic artery to segment 4 was encountered and divided. The left hepatic artery was identified and divided. The hepatic hilum was completely skeletonized (Fig. 1d). The common bile duct was then divided. Cholecystectomy was performed, and the gallbladder was removed en bloc with the right-sided lymph nodes. The left portal vein was carefully dissected and ligated. Hepatic pedicle dissection was completed, so that the left liver was now ischemic and ready to be transected. The future line of transection was marked with cautery, along the liver's surface. Liver transection was accomplished with a Harmonic® scalpel (Ethicon Endo-Surgery) and endoscopic stapling device as appropriate. The left liver, including segments 2–4, was removed. Bile ducts from the anterior and posterior right sectors of the liver were identified and measured about 2 mm. Because of the difficult localization and small caliber of the bile ducts we decided to perform a video-assisted bilioenteric reconstruction. 10 A small subcostal incision was performed, and the specimen was extracted. The magnification of the video was useful in safely performing the hepaticojejunostomy. Pneumoperitoneum was re-established, and raw surfaces of the liver were reviewed for bleeding and bile leaks. One round 19-French abdominal drain was left in place.
Results
Operative time was 300 minutes with minimum blood loss and no need for blood transfusion. Recovery was uneventful, and the patient was discharged on postoperative Day 7. The abdominal drain was removed on postoperative Day 10 with no signs of biliary leakage. Histological examination revealed a well-differentiated cholangiocarcinoma with negative lymph nodes and clear surgical margins. The patient is well with no signs of the disease 18 months after the procedure.
Discussion
Several studies have demonstrated the safety and feasibility of laparoscopy for minor and major liver resections, and some have shown that laparoscopy is associated with less bleeding, fewer complications, and a better quality of life than open liver surgery.6–8 However, its use in hilar cholangiocarcinoma has not gained popularity. The main challenges are the extensive hilar dissection and hilar lymphadenectomy, but the most difficult part is the need for a complex biliary reconstruction, especially when remaining bile ducts are of a very small caliber such as the case presented. According to the report of Giulianotti et al. 9 they also used a limited abdominal incision for extraction of the specimen and construction of the Roux-en-Y loop. This strategy was used to speed up the procedure. However, the biliary reconstruction was performed using the robot-assisted technique. In our case there were two separated bile ducts with a maximum diameter of 2 mm, deeply located inside the parenchyma and in a position that would hinder any chance of a perfect anastomosis. The decision was to perform the hepaticojejunostomy using an incision but assisted with the magnification of the 30° laparoscope. Indeed, the anastomosis was satisfactorily performed under this condition, and the patient did not present any biliary leakage or stenosis during the late follow-up.
In conclusion, laparoscopic left hepatectomy with lymphadenectomy is safe and feasible in selected patients and when performed by surgeons with expertise in both liver surgery and minimally invasive techniques. The use of a hybrid method may be needed for biliary reconstruction, especially in cases where the position and size of remnant bile ducts may jeopardize the anastomosis. Further studies are still needed to confirm the benefit of this approach over conventional surgery for hilar cholangiocarcinoma.
Footnotes
Disclosure Statement
No competing financial interests exist.