
Abstract
Abstract
Background:
Many reconstructive procedures have been developed in an effort to resolve complications after total gastrectomy (TG). However, anatomical disruption of the esophagogastric junction, especially the low esophageal sphincter, still occurs so that postoperative complications continue to arise. In this study, we developed a procedure for intracorporeal laparoscopic Roux-en-Y gastrojejunostomy (RYGJ) after 95% (near-total) gastrectomy, to reduce postoperative complications in early gastric cancer (EGC) of the upper third of the stomach.
Patients and Methods:
Laparoscopic RYGJ after 95% gastrectomy was performed on 21 patients with EGC in the upper third of the stomach between May 2011 and April 2012 in Asan Medical Center, Seoul, Korea. The resection line of the stomach was marked using metallic preoperative endoscopic clips and intraoperative laparascopic vessel clips together with a portable abdominal radiograph. Approximately 95% of the stomach was transected using an endoscopic linear stapler, and an antecolic side-to-side gastrojejunal anastomosis was created between the posterior side of the gastric remnant and the antimesenteric side of the jejunal limb, also using an endoscopic linear stapler. The entry hole was first closed in approximate fashion with three sutures, and closure was completed with an endoscopic linear stapler.
Results:
Intracorporeal laparoscopic RYGJ after 95% gastrectomy was successfully performed in all patients. No patients required conversion to open surgery or other laparoscopic anastomosis techniques. No postoperative complications occurred. All patients had tumor-free resection margins, and there was no mortality.
Conclusions:
Intracorporeal laparoscopic RYGJ after 95% gastrectomy can be performed easily and safely. We recommend this method over laparoscopic TG or open TG for treatment of EGC in the upper third of the stomach.
Introduction
Since laparoscopy-assisted distal gastrectomy was performed for the first time by Kitano et al., 3 this minimally invasive surgery has been widely accepted as a viable option for treatment of gastric cancer rather than open gastrectomy, because of many advantages such as reduced surgical invasiveness, less postoperative pain, better cosmesis, early postoperative recovery, and excellent long-term survival.3,4 As diverse laparoscopic surgical techniques have been developed in addition to laparoscopy-assisted distal gastrectomy, laparoscopic procedures have been introduced and adapted for treatment of EGC.1,2 However, although several investigators have reported that laparoscopic total gastrectomy (TG) is feasible and safe,6–8 alimentary tract reconstruction, which is critical to the success of the operation, is technically difficult after this procedure, especially after laparoscopic esophagojejunostomy following TG.9–11
Open TG, on the other hand, is reported to be associated with a higher operative mortality rate (up to 30%), a significant portion of which is attributable to leakage of the esophagoenteral anastomosis.12,13 In addition, anatomical disruption of the esophagogastric junction can lead to several problems as the lower esophageal sphincter (LES) serves as a mechanical barrier to gastroesophageal reflux.14–16 These functional disturbances induce a variety of postgastrectomy symptoms that adversely affect QoL, such as heartburn, early satiety, and swallowing difficulty. Surgical procedures for EGC that allow functional preservation have been developed to reduce these complications, but these are limited in their effectiveness.
The aim of this study was to find an effective method to reduce postoperative complications caused by a disturbed LES and thus might enhance the QoL of patients after gastrectomy. To achieve this aim, we developed the procedure of intracorporeal laparoscopic Roux-en-Y gastrojejunostomy (RYGJ) after 95% gastrectomy for EGC in the upper third of the stomach. With this technique we have attempted to achieve the radicality of TG without the postoperative complications that are often caused by esophagojejunal anastomosis.
Patients and Methods
Patients
Between April 2011 and April 2012, 21 patients (12 men, 9 women) with EGC underwent intracorporeal laparoscopic RYGJ after 95% gastrectomy, performed by the same surgeon, in Asan Medical Center, Seoul, Korea. All these patients had been diagnosed with EGC in the upper third of the stomach, or EGC with lesions that had spread to the upper and middle gastric regions, with no lymph node metastasis detected preoperatively or intraoperatively. The diagnoses were based on preoperative examinations including esophagogastroduodenoscopy, endoscopic ultrasound, and computed tomography scans. Gastric cancer near the gastroesophageal junction was defined as that in which the upper margin of the tumor was located within 3 cm of the gastroesophageal junction or in which a fundus lesion was present, as indicated by postoperative pathologic results. These cases were excluded because it is usually sufficient to resect these EGCs with a 2-cm margin. Radical lymph node dissection was defined as D1+β or above D2 dissection following the Japanese classification of gastric carcinoma. 17
Surgical techniques
Gastrectomy
The resection line for the 95% gastrectomy was determined as described in previous reports.1,5,18,19 As part of this process, patients underwent a preoperative endoscopy in the week before surgery, in which two or three endoscopic metallic clips (model HX-600-090L; Olympus, Tokyo, Japan) were applied at sites just proximal to the lesion, 1–2 cm orally from the most proximal margin of the tumor (Fig. 1).
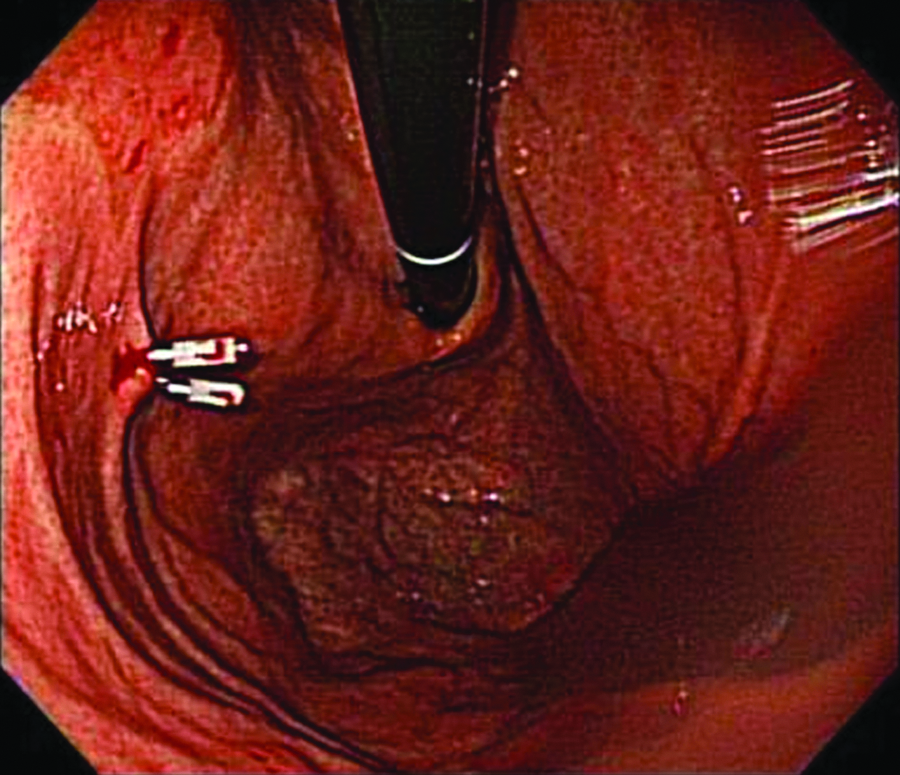
Endoscopic clipping for determining the resection line.
For the operation, patients were placed in the reverse Trendelenburg position. A carbon dioxide pneumoperitoneum was formed from the umbilical port, with pressure maintained between 12 and 15 mm Hg. Four trocars were used, placed in a U-shaped pattern (Fig. 2). To retract the liver, the intracorporeal suturing was performed at the attachment site of the lesser omentum from the right diaphragmatic cruse, and then a thread pulled by a suture-passer was tied on the skin in the xiphoid process area (Fig. 3). If the operating field was insufficient, an additional 5-mm trocar was inserted into the epigastric area to retract the liver.
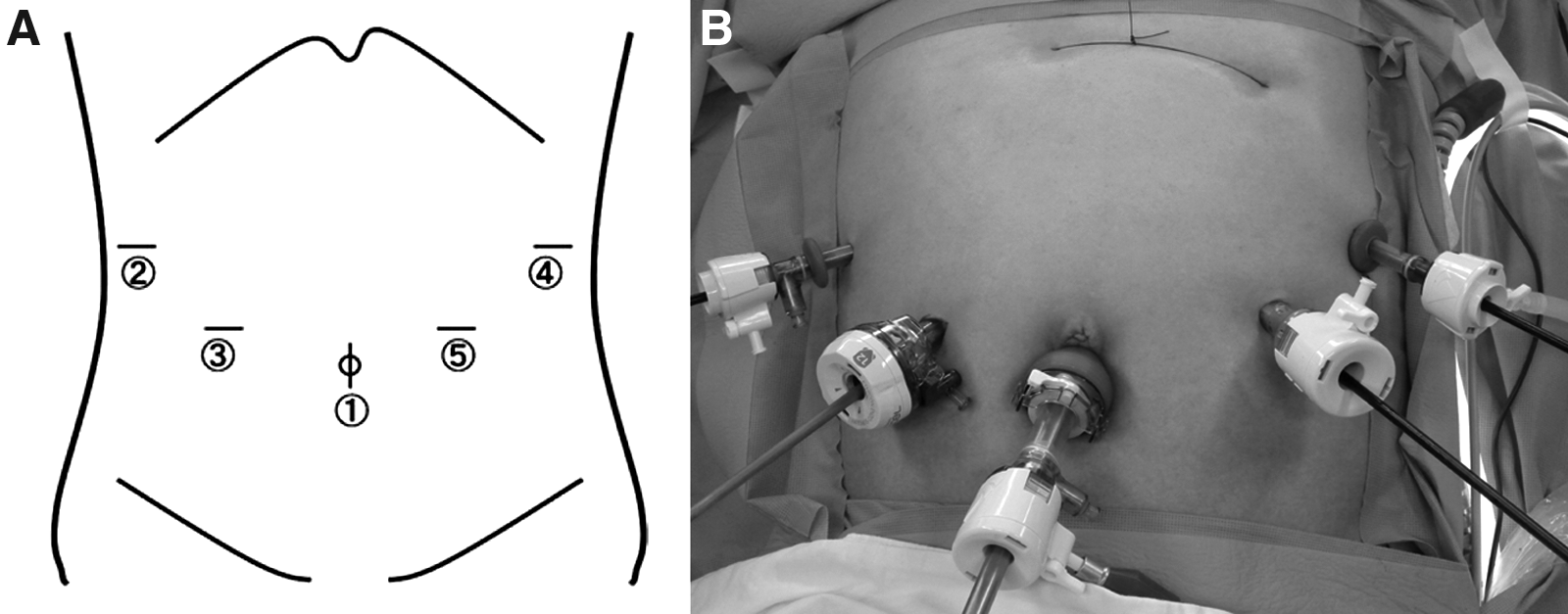
Placement of trocars.
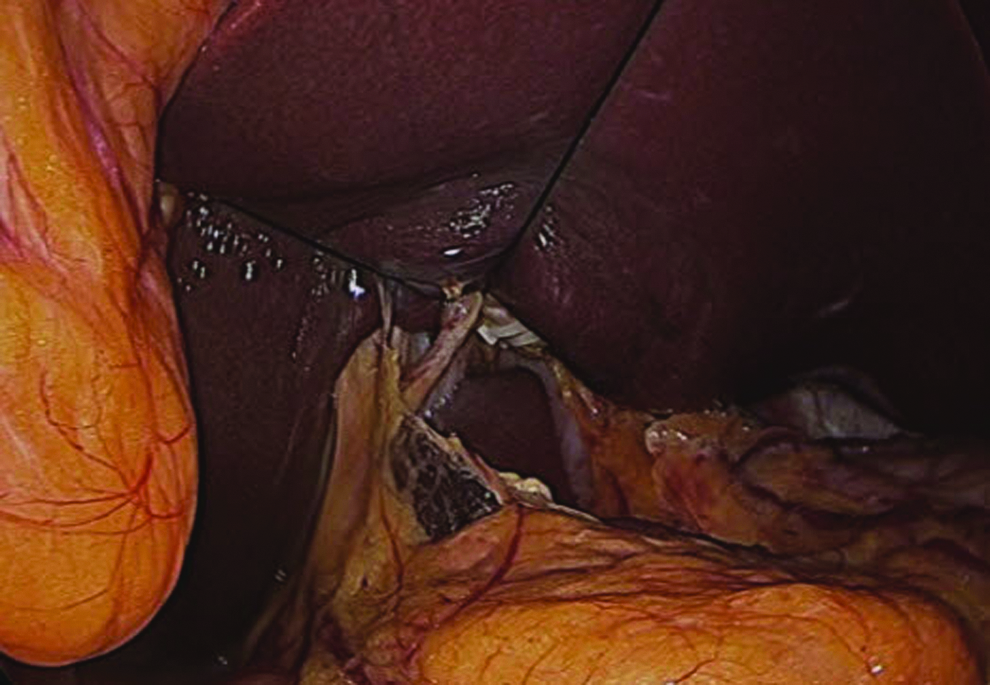
Retraction of the liver during laparoscopic gastrectomy.
Dissection was begun by dividing the greater omentum from the midportion of the gastroepiploic arcade to the left gastroepiploic vessel. After this, the lymph nodes around the left gastroepiploic and short gastric vessels were dissected, with care taken to preserve at least two short gastric vessels. The infrapyloric area was then dissected. After lymph node dissection around the suprapyloric area, the duodenum was transected just below the duodenal bulb using an endoscopic linear stapler (Echelon™ Flex™ 60; Ethicon, Blue Ash, OH) with a closed stapler height of 1.5 mm. Subsequently, the lymph nodes around the common hepatic, proximal or distal splenic, celiac, and left gastric arteries were dissected (in that order), followed by dissection of the lymph nodes approximately 4 cm below the gastroesophageal junction at the lesser curvature. When the root of the left artery was divided, care was taken to try to ensure that the celiac branch of the vagus nerve was preserved, to maintain the patient's gastrointestinal motility following surgery (Fig. 4). 20
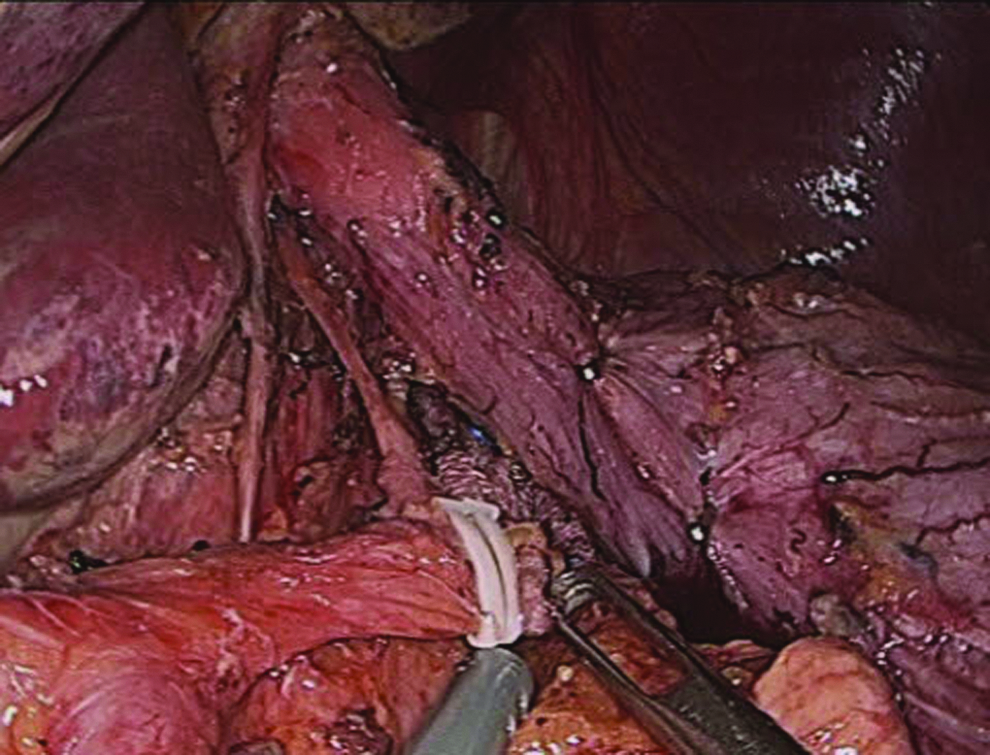
Preservation of the celiac branch of the vagus nerve.
After dissection of all lymph nodes, the resection line of the stomach was determined using the method of intraoperative portable abdominal radiography for localization of the tumor.3,5,19 We applied metallic intraoperative laparoscopic vessel clips along the greater and lesser curvatures of the external surface of the stomach, according to the information acquired from the preoperative endoscopy (Fig. 5A). Intraoperative portable abdominal radiographs were then taken to identify the location of these clips relative to the previously applied endoscopic clips (Fig. 5B). 18 The line connecting the external laparoscopic vessel clips on the greater and lesser curvatures was taken to be the resection line. A minimum proximal resection margin of 2 cm from the endoscopic clips was ensured.
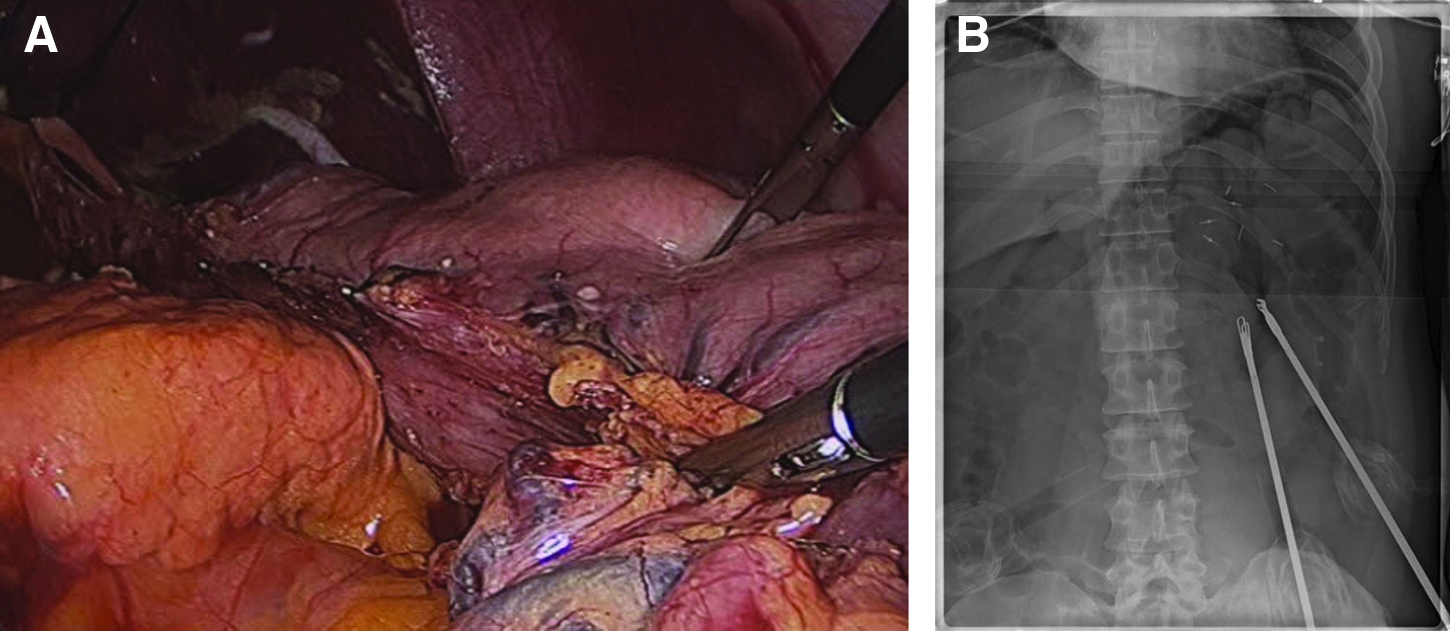
Intraoperative portable abdominal radiography for tumor localization.
The proximal stomach was transected just below the esophagogastric junction using an endoscopic linear stapler (Echelon Flex 60) with a closed stapler height of 1.5 mm with full articulation at 45° along the resection line. Transection of the stomach was then continued, with the direction turned along the imaginary resection line (Fig. 6A). Approximately 95% of the stomach was transected, leaving only a 2–3-cm proximal gastric remnant (Fig. 6B and C).
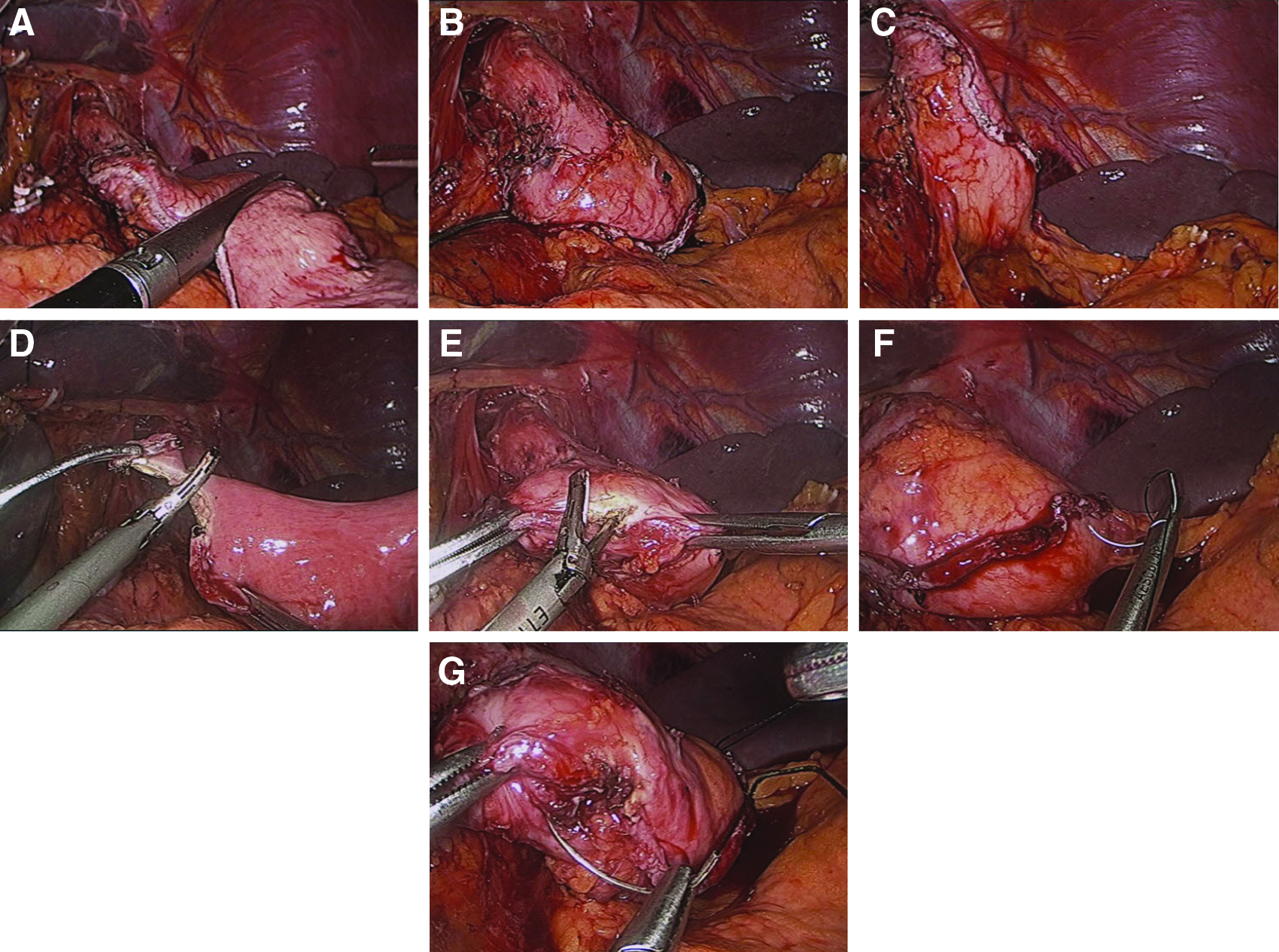
Gastrostomy and jejunostomy construction.
The resected specimen was subsequently removed through the umbilical port by extending the incision to an I-shaped one of approximately 3 cm in length. After removal of the specimen, the location of the tumor was determined, and the 2-cm gross negative margin was confirmed. The proximal resection margin of the specimen was examined pathologically after freezing.
Intracorporeal laparoscopic RYGJ
After completion of the gastrectomy, the umbilical trocar was reintroduced, and the three or four interrupted sutures were tied at the umbilical incision to reinstate the pneumoperitoneum. To identify the ligament of Treitz, the transverse colon and remaining greater omentum were brought toward the upper abdomen. The proximal jejunum was then divided 20 cm distally to the ligament of Treitz using an endoscopic linear stapler (Echelon Flex 60), and the efferent loop was turned in a counterclockwise direction to construct the gastrojejunostomy (GJ). An enterostomy of the jejunum was created in the antimesenteric side of the Roux-en-Y limb using an ultrasonic cutting and coagulation system (Harmonic ACE™ curved shears; Ethicon) (Fig. 6D), and a gastrostomy was created in the right end of the transected stapling line of the 2–3-cm gastric remnant, using the same system (Fig. 6E). For easy construction of the intracorporeal GJ, two sets of intracorporeal sutures were performed at the stapled line of the gastric remnant: the first set was placed at the right side of the gastrostomy (Fig. 6F), and the second set was placed at the left end of the stapled line of the gastric remnant (Fig. 6G). These sutures were used to retract the gastric remnant during insertion of the anvil of the endoscopic linear stapler into the gastrostomy for construction of the GJ.
The Roux limb was brought up close to the gastric remnant in an antecolic way, and then the gastrojejunal anastomosis was constructed between the posterior wall of the gastric remnant and the antimesenteric side of the afferent jejunal loop, which were positioned to face each other (Fig. 7A). An endoscopic linear stapler (Echelon Flex 60) with a closed staple height of 1.5 mm was inserted into the enterostomy of the jejunum and the gastrostomy. The stapler was then fired to establish the GJ at the posterior wall of the gastric remnant. The GJ was then constructed along the posterior side of the gastric remnant in a side-to-side horizontal fashion.
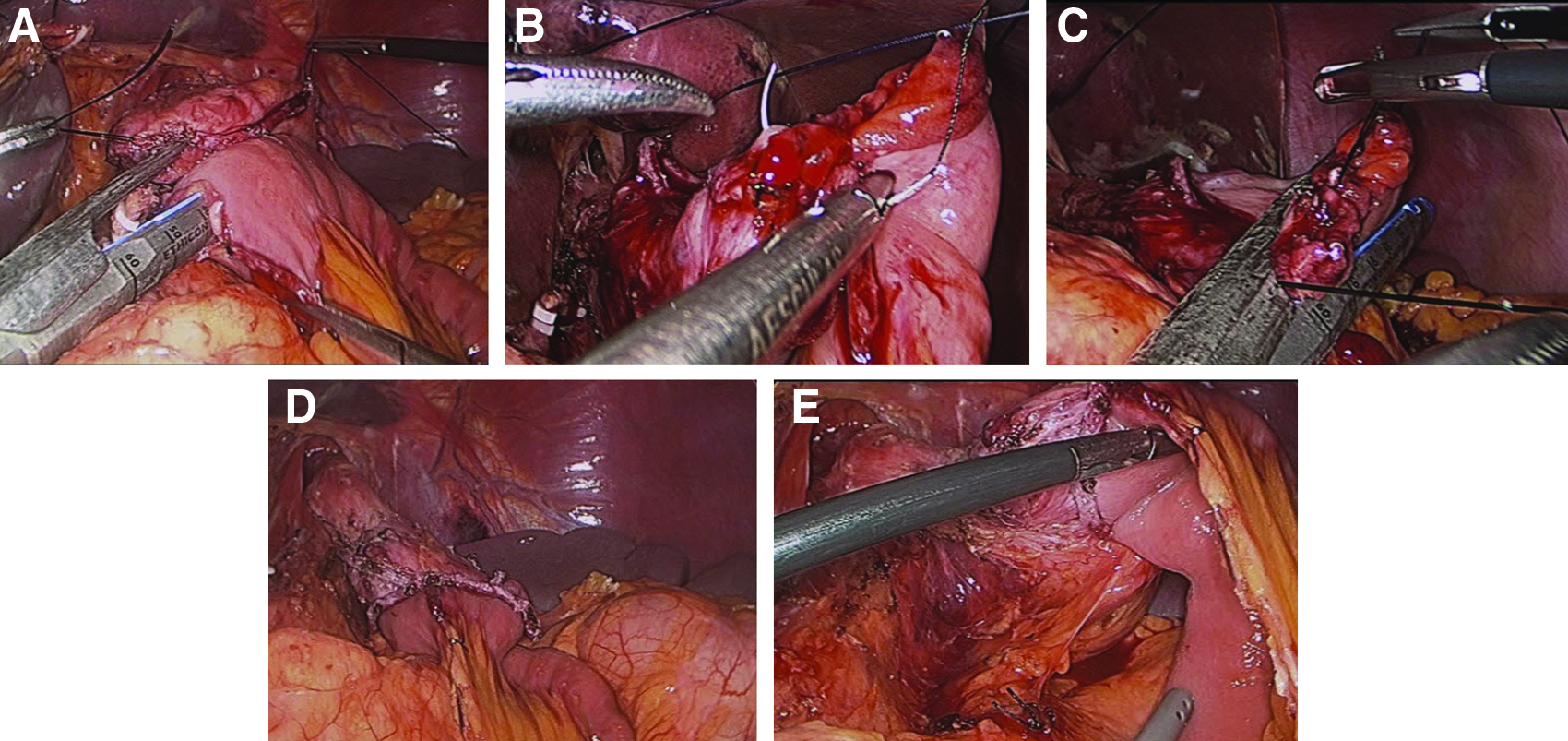
Gastrojejunostomy construction.
After construction of the GJ, the entry hole was closed with three sutures for tissue approximation, and closure was then completed using an endoscopic linear stapler (Echelon Flex 60) (Fig. 7B). In some cases further suturing was necessary to complete the closure. Upon completion of the GJ we confirmed that both the posterior and anterior sides of the anastomosis were secure (Fig. 7D and E). The GJ was then examined for any evidence of leakage by injecting methylene blue dye through a Levin tube during the operation.
A side-to-side linear mechanical jejunojejunostomy was then constructed. To achieve this two enterostomies were created: one on the antimesenteric side of the jejunum, 40 cm below the GJ (Fig. 8A), and the other on the antimesenteric side of the afferent loop (Fig. 8B). An endoscopic linear stapler (Echelon Flex 60) was inserted into these enterostomies to construct the jejunojejunostomy (Fig. 8C). The remnant entry hole was closed with three sutures for tissue approximation, and closure was completed using an endoscopic linear stapler (Echelon Flex 60) (Fig. 8D and E). Finally, the mesenteric defects were sutured, and the operation was completed.
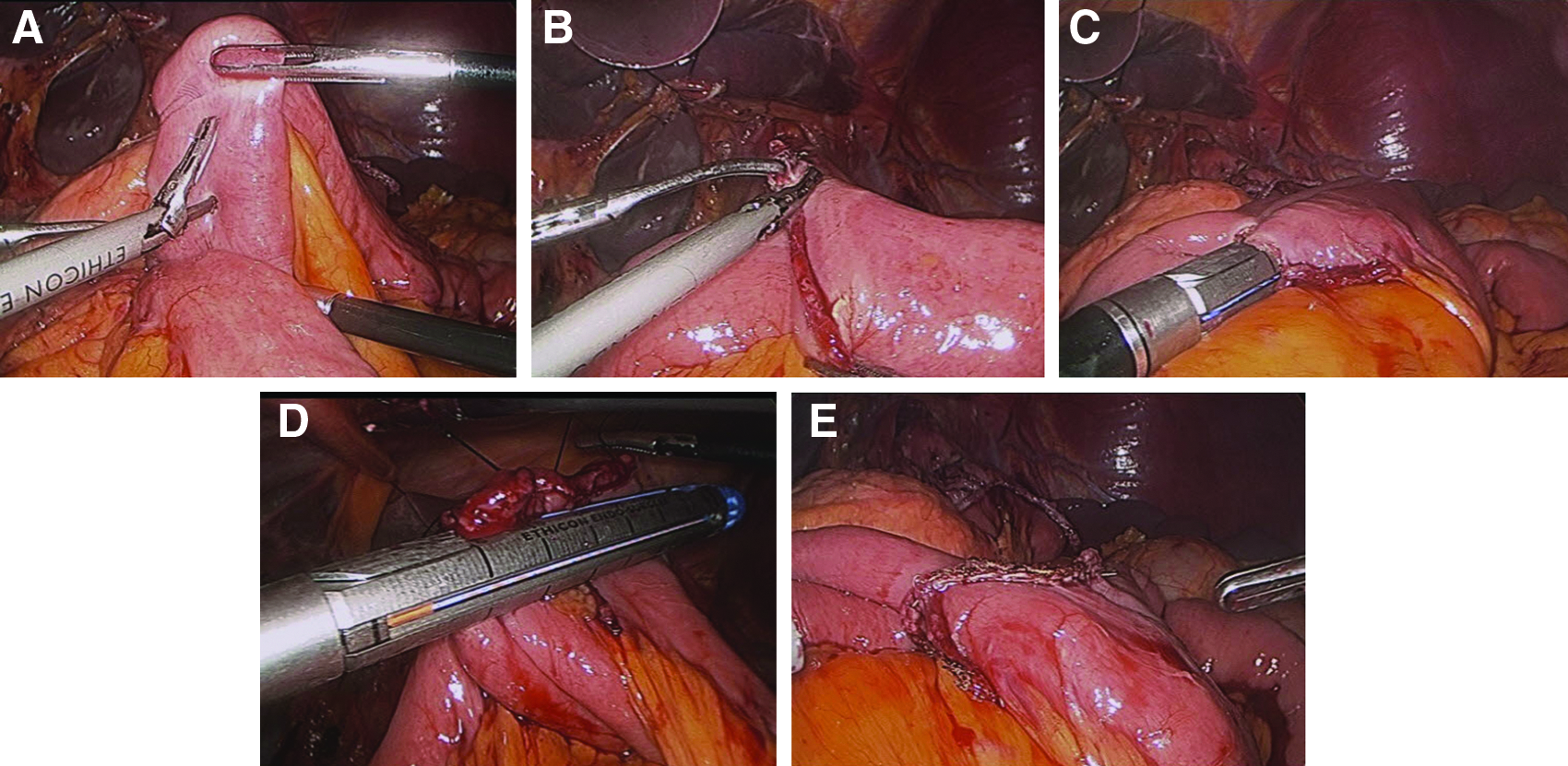
Jejunojejunostomy construction. Two enterostomies were created using the ultrasonic cutting and coagulation system:
Postoperative management
The gastrojejunal anastomoses were examined 3 days after the operations using diatrizoate meglumine and diatrizoate sodium solution (Gastrografin®; Bayer Schering Pharma AG, Berlin, Germany) to check for anastomotic leaks (Fig. 9). A soft diet was commenced when the patient felt sufficiently comfortable to eat soft foods. Patients were discharged when they had no problems eating a soft diet, were generally comfortable, and demonstrated an absence of inflammatory symptoms, including leukocytosis, unstable vital signs, and abrupt onset of abdominal pain. The final decision regarding discharge was made by the patient.

Gastrografin study. Fluorography demonstrated the smooth passage of contrast medium through the anastomosis without leakage or stenosis.
Clinical analysis of surgical outcomes
The following clinical data were obtained from medical records: patient age, gender, body mass index, and American Society of Anesthesiologists (ASA) score. Obesity was defined according to the World Health Organization Asia-Pacific Obesity classification, in which a body mass index above 25 kg/m2 was considered overweight.21,22 The following early surgical outcomes were recorded: operation time, intraoperative events, overall postoperative complications, time to first flatus, time to commencement of soft diet, and length of postoperative hospital stay. The following pathology results were recorded: number of retrieved lymph nodes, resection margins, and cancer stage according to the Japanese Classification of Gastric Carcinoma, 3rd edition. 17 A postoperative complication was defined as any condition that required conservative or surgical treatment. Severe postoperative complications were defined as conditions requiring management by an endoscopic or interventional procedure or reoperation without general anesthesia. 23 Data were collected prospectively and maintained in a computerized database. They are reported as mean±standard deviation values.
Results
We investigated 12 male (57.1%) and 9 female (42.9%) EGC patients with a mean age of 53.3 years (range, 33–78 years). The mean body mass index of the patients was 25.5 kg/m2 (range, 19.0–30.4 kg/m2). According to the ASA classification, 14 patients (66.7%) were ASA 1, 5 (23.8%) were ASA 2, and 2 (9.5%) were ASA 3. Eight patients (38.1%) had undergone previous abdominal surgery.
There were no adverse intraoperative events during gastrojejunal anastomosis construction. The procedure was performed successfully on all patients using an endoscopic linear stapler. No patients required conversion to open surgery or other laparoscopic anastomosis techniques. The gross resection margin and the frozen section were negative in all cases. All operations were curative, and no postoperative complications occurred; of particular importance is that there were no symptoms due to disruption of the LES. There were no patients on proton pump inhibitors preoperatively and postoperatively for reflux symptom.
The mean operation time was 171.9±37.5 minutes. The time to first flatus was 2.9±0.6 days, and the time to commencement of a soft diet for patients with no morbidity was 3.7±0.6 days. The mean length of postoperative hospital stay for patients with no morbidity was 6.3±0.8 days.
Upon pathologic examination, the location of the tumor was determined to be the upper body in 14 patients and the mid-body in 7 patients. Pathologic analysis of tumor characteristics revealed that 17 patients (81.0%) had T1 tumors and 4 patients (19.0%) had T2 tumors. Two patients (9.5%) were found to have lymph node metastasis. Two patients were T2N1, and they only had chemotherapy (TS-1) after operation. The mean proximal resection margin was 2.0±1.6 cm, and the mean number of retrieved lymph nodes was 36.6±11.6. There was no involvement of the proximal resection margin in any patient.
Fluorography demonstrated the smooth passage of contrast media through the anastomoses without leakage or stenoses in all patients (Fig. 9).
Postoperative esophagogastroduodenoscopy was examined 6 months after operation in all patients. There were no patients who had any specific abnormality in the esophagus, remnant stomach, anastomotic ring, A-loop, and E-loop.
Discussion
Gastric cancer has traditionally been treated primarily by gastrectomy and radical lymph node dissection.1,2 Recently, because of the increasing rate of EGC detection in the upper third of the stomach, treatment considerations, such as gastrectomy type, extent of resection, reconstruction methods, surgical curability, and prognosis, have been important issues. 24 Because the prognosis for EGC is excellent, interest has been directed particularly at improving QoL for EGC patients after treatment and on the use of minimally invasive surgery. Therefore knowledge of postoperative QoL should be taken into consideration when making clinical decisions regarding therapy.
Since 1994, when the first laparoscopic gastrectomy for gastric cancer was reported by Kitano et al, 3 additional minimally invasive approaches to gastric cancer have been developed. Laparoscopic distal gastrectomy has gradually become accepted for the treatment of EGC, at least with regard to its oncologic aspects and postoperative QoL, and recently several types of laparoscopic TG have been introduced. However, with regard to technical aspects, laparoscopic reconstruction, especially construction of an esophagojejunal anastomosis after laparoscopic TG, is a difficult and complex procedure that most surgeons are unable to perform. In addition, laparoscopic TG can only be performed after accumulation of a significant amount of experience in laparoscopic surgery.
Furthermore, TG may result in postoperative complications such as heartburn, dysphagia, bitter taste, and regurgitation, which suggest the presence of reflux esophagitis due to disruption of the esophagojejunal junction.15,25 Mechanical disruption of the LES allows components of the refluxate such as duodenal secretions, pancreatic secretions, and bile to cause tissue destruction.9,24 This allows the development of structure and Barrett's esophagus.9,23 Several investigators have reported that a high incidence of esophagitis and reflux esophagitis complications, such as benign stenosis and Barrett's esophagus, was still evident a relatively long time after TG.15,26 Thus the QoL of patients after TG can be significantly decreased by these complications. Many reconstructive procedures have been developed in an effort to resolve such complications and to improve the nutritional condition of patients after TG.24,25 However, the optimal digestive tract reconstruction procedure after TG is still a matter of debate.
The operative mortality of TG has been reported to be between 6% and 30%,12,13,27 and even in more recent studies, it is at least 8%–10%.12,13,18,24,27 In contrast, Salo et al. 27 reported that the hospital mortality rate for 95% (subtotal) gastrectomy was 5%, lower than the rate for TG. They also reported that the incidence of anastomosis leakage for 95% gastrectomy was 1.7%, which is very low compared with the incidence for TG, where leakage of the esophagojejunostomy anastomosis is up to 21%, with a mortality rate of about 50%. 12 The security of the anastomosis between the minute gastric remnant and the jejunum in 95% subtotal gastrectomy is of utmost importance. The reason why an anastomosis between the 2–3-cm gastric remnant and the jejunum heals better than an anastomosis between the esophagus and the jejunum is unclear. 27
In this study, we developed the technique of intracorporeal laparoscopic RYGJ after 95% gastrectomy, in which importance is placed on preservation of the anatomy of the esophagogastric junction: the LES, crural diaphragm, phrenoesophageal ligament, acute angle of His, intra-abdominal segment, and mucosal rosette. This, along with the minimally invasive nature of the surgery, reduces postoperative complications.
There are some important points to note regarding this surgical method. First, when the lymph nodes around the short gastric vessels were dissected, as many as possible and at least two of the short gastric vessels were preserved. The reason for this was that insufficient blood supply to the gastric remnant could lead to failure of the gastrojejunal anastomosis. A second point to note regarding this surgical method is that the gastrojejunal anastomosis was constructed between the posterior wall of the gastric remnant and the antimesenteric side of the efferent jejunal loop. There was initially insufficient space to insert an endoscopic linear stapler during construction of the gastrojejunal anastomosis in a way that would not lead to injury upon firing because the gastric remnant was so small and adjacent to the short gastric vessels. Therefore, when the gastrojejunal anastomosis was constructed, retraction of the stomach was required to allow a sufficient line for the anastomosis. For this reason, two intracorporeal sutures were performed at the stapled line of the gastric remnant, and these sutures were retracted during the construction of the gastrojejunal anastomosis. By retracting these sutures, it was possible to insert an endoscopic linear stapler without great difficulty between the gastrostomy and the enterostomy of the jejunum in order to construct the GJ.
There are very few definite guidelines that cite the clinical literature and provide recommendations for the distance between tumor and resection margin. In a search of Medline we found only two articles that provide such recommendations.25,26 Bozzetti et al. 28 evaluated 343 patients with gastric cancer, including advanced cancer, with special reference to the outlines of the tumor, assessed grossly, together with other macroscopic or microscopic features of the tumor. They reported that neither proximal nor distal infiltration occurred at a distance >3 cm in lesions confined to the mucosa, submucosa, and muscularis. However, this study was conducted 30 years ago. In the Japanese gastric cancer treatment guidelines 2010 (version 3), 29 a gross resection margin of 2 cm is recommended for T1 tumors. In our procedure, the gross free margin was at least 2 cm, and frozen-section examination of the proximal resection line was conducted to ensure that an R0 resection had been performed.
By using intracorporeal laparoscopic RYGJ after 95% gastrectomy, we have attempted to achieve the radicalism of TG without the esophagojejunal anastomoses that often lead to postoperative complications. Although the facts that all the procedures were performed by the same surgeon and the lack of comparative data for TG are limitations of this study, satisfactory results were obtained. The procedures were completed uneventfully, and conversion to open procedures or other laparoscopic anastomosis techniques was not required in any instance.
In conclusion, our technique of laparoscopic intracorporeal RYGJ after 95% gastrectomy yields acceptable surgical outcomes in terms of anastomosis-related complications and early postoperative course. Thus this technique should be effective in allowing functional preservation of the LES and stomach of EGC patients. However, the number of patients in this study was very small, and patients who failed to complete a long-term follow-up survey were included. It will be necessary to confirm these results in a larger number of patients to demonstrate the validity of our conclusions, but based on these preliminary results we believe that intracorporeal laparoscopic RYGJ after 95% gastrectomy is preferable to TG for treatment of EGC in the upper third of the stomach.
Footnotes
Disclosure Statement
No competing financial interests exist.