
Abstract
Abstract
Background:
Despite the popularity of laparoscopic-assisted distal gastrectomy (LADG), studies have reported a high incidence of postoperative complications in patients who have had LADG. The present study explores the preoperative risk factors for complications from LADG.
Patients and Methods:
This study involves 1257 patients who underwent standardized LADG in a single institution between January 2006 and June 2011. The risk factors for postoperative complications of LADG were evaluated by univariate and multivariate analyses.
Results:
In univariate analysis of overall postoperative complications, there were significant effects of age (above 65 years), obesity (a body mass index above 25 kg/m2), comorbidity, cerebrovascular disease, heart disease, hypertension, diabetes mellitus, and combined comorbidities (three or more). Multivariate analysis of these risk factors showed that old age (P=.006), obesity (P<.001), and heart disease (P=.014) were independent risk factors for postoperative complications. Univariate analysis showed that obesity also had a significant effect on severe postoperative complications.
Conclusions:
Older age, obesity, and heart disease are risk factors for postoperative complications after LADG. Greater caution or more limited surgery is required to reduce the high rate of complications in patients with these risk factors.
Introduction
Few reports have evaluated the preoperative predictive factors for postoperative complications after LADG.11,12 It is important to predict these factors because increasing numbers of gastric cancer patients with various comorbidities undergo LADG. These risk factors may also be used in the preoperative assessment of patients with comorbidities, which in turn may help to reduce postoperative complications.
This study evaluates the impact of predictive risk factors on the surgical outcomes of LADG.
Patients and Methods
Patients
We reviewed prospectively collected data from the electronic medical record of 1364 consecutive patients who underwent LADG for EGC between January 2004 and June 2011 at the Asan Medical Center (Seoul, Korea). We did not include the 107 patients who underwent unstandardized LADG from 2004 to 2005 because the standardized LADG developed in our institution has been used since 2006 and has led to shorter postoperative length of hospital stay, fewer surgical complications, and decreased operation times (Fig. 1). Of the 1364 patients in the study, 1257 were analyzed for risk factors for postoperative complications of LADG. All these patients had been diagnosed with EGC in the lower third of the stomach, with no lymph node metastasis detected preoperatively or intraoperatively. The diagnoses were based on preoperative examinations, including esophagogastroduodenoscopy, endoscopic ultrasound, and computed tomography scans. All patients underwent D1+β lymph node or D2 dissections, according to the Japanese classification of gastric carcinoma. 15
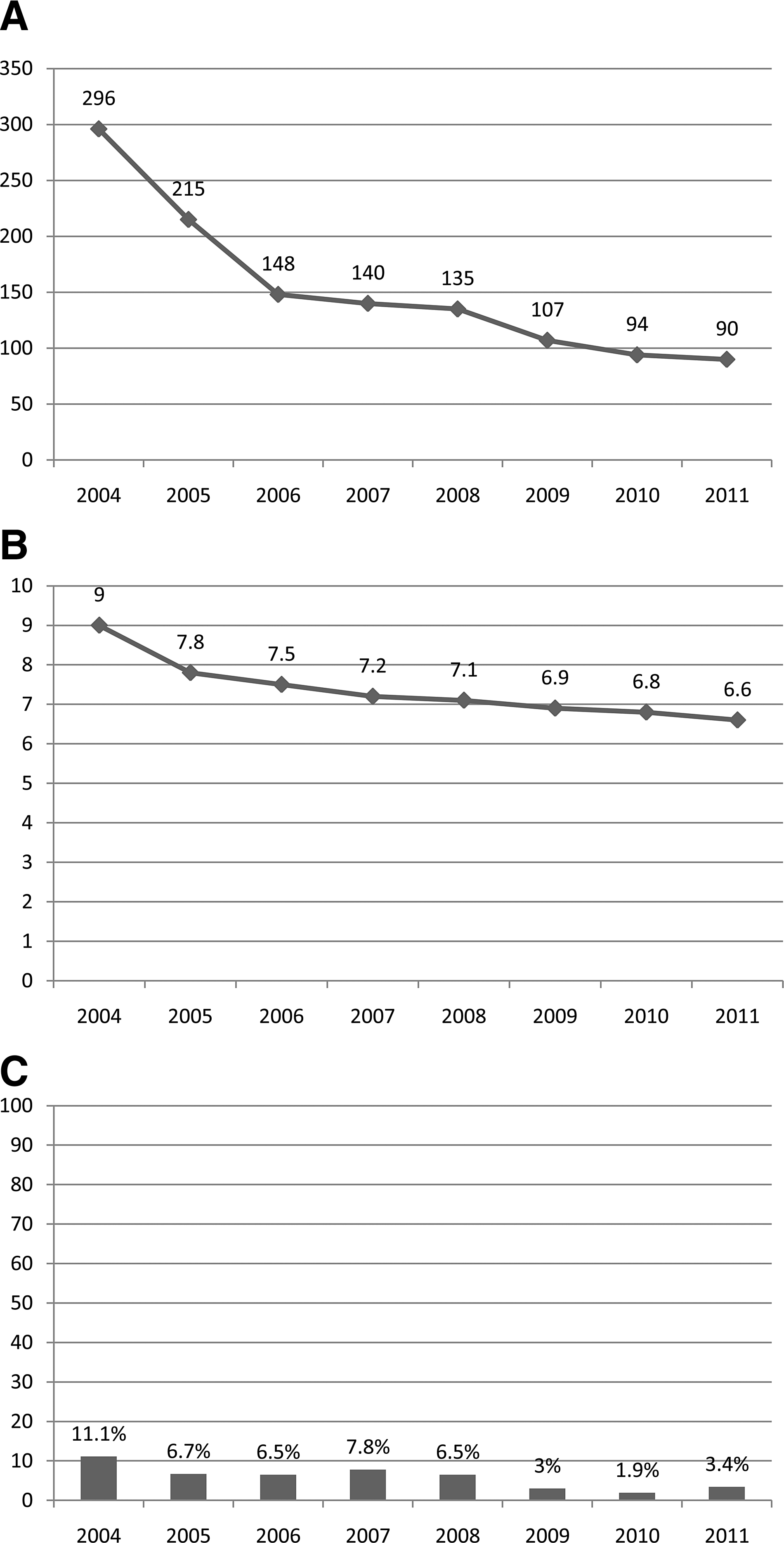
Annual trends of
Preoperative risk factors for postoperative complications
In the present study, we evaluated the gender, age, obesity, history of previous abdominal surgery and preoperative comorbidities of patients to explore the risk factors for postoperative complications. Postoperative complications were defined as any that required conservative or surgical treatment according to the Accordion classification. 16
The World Health Organization Asia-Pacific obesity classification is as follows: normal weight (body mass index [BMI], 18.5–24.9 kg/m2), overweight (BMI, 25.0–29.9 kg/m2), and obese (BMI, ≥30 kg/m2 ).17,18 In our study, obese patients were defined as having BMI ≥25 kg/m2 (301 patients), and underweight patients were defined as having BMI <18.5 kg/m2 (22 patients).
Cerebrovascular diseases such as stroke and hemorrhage were defined as conditions that develop as a result of problems with blood vessels in the brain. Heart disease was defined as any disorder that affects the heart, such as angina, arrhythmia, congenital heart disease, heart attack, heart failure, and cardiomyopathy. Pulmonary disease was defined as any disease or disorder that occurs in the lungs or that causes the lung to work inefficiently, such as asthma, chronic obstructive pulmonary disease, emphysema, and tuberculosis. Liver disease referred to any disorder of the liver, such as cirrhosis and inflammation (hepatitis B, hepatitis C). Diabetes mellitus and hypertension were defined as conditions requiring medication to control blood sugar level and blood pressure, respectively.
Surgical techniques
Each patient was placed in the reverse Trendelenburg position under general anesthetic. A camera port (12 mm) was introduced into the subumbilical region. A carbon dioxide pneumoperitoneum was generated at the umbilical port and maintained at a pressure of 12–15 mm Hg. Four trocars were placed on the abdomen in a U shape: on the right lower quadrant (12 mm), right upper quadrant (5 mm), left lower quadrant (5 mm), and left upper quadrant (5 mm) (Fig. 2). The falciform ligament was fixed to the anterior wall of the peritoneum to retract the liver using an Endo Close™ (Covidien, Norwalk, CT). If the operating field was not sufficient, an additional 5-mm trocar was inserted into the epigastric area to retract the liver.
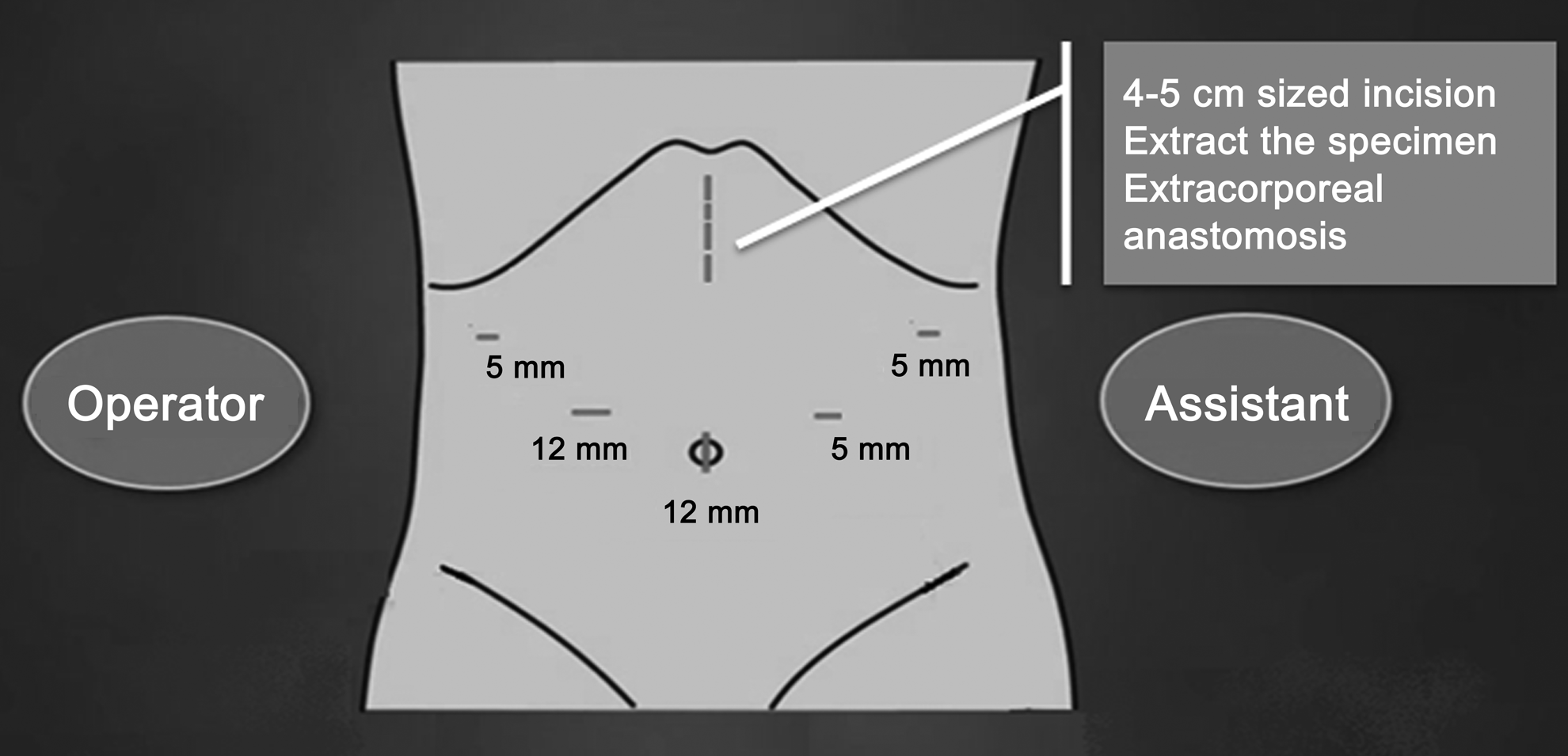
Placement of trocars for laparoscopic-assisted distal gastrectomy.
The greater omentum was divided from the midportion of the gastroepiploic arcade to the left gastroepiploic vessel using an ultrasonic cutting and coagulation system (Harmonic ACE™ curved shears; Ethicon Endo-Surgery, Inc., Somerville, NJ) with clips. The lymph nodes around the left gastroepiploic and short gastric vessels were then dissected. Thereafter the lymph nodes around the right gastroepiploic area were dissected, followed by dissection of the infrapyloric area. Then the nodes around the suprapyloric area were dissected, together with the hepatoduodenal ligament (along the hepatic artery), the common hepatic, proximal, and distal splenic, celiac, and left gastric arteries, and the right pericardial artery, in that order. Next, the lesser omentum was dissected from the proximal side toward the distal side. The lymph node dissection was performed intracorporeally.
After the lymph nodes were cleated, a 4–5-cm midline incision was made from the epigastric trocar site to reconstruct a gastroduodenostomy (Billroth-I) (Fig. 2). After a wound protector was applied, the stomach was pulled out extracorporeally. We carried out essentially the same procedure as that used to reconstruct a gastroduodenostomy by the conventional open method. A 28-mm circular stapler (Proximate® ILS; DST Series™ EEA™; Ethicon) was used to make the gastroduodenostomy.
Postoperative management
Diatrizoate meglumine and diatrizoate sodium solution (Gastrografin®; Bracco Diagnostics, Milan, Italy) was used to evaluate leakage on postoperative Day 5 in patients who had had an intraoperative event during reconstruction of the gastroduodenostomy. A soft diet was begun when the patient felt comfortable enough to eat soft foods. Patients were discharged if they had no problems eating a soft diet, were generally comfortable, and had no symptoms indicating inflammation, such as leukocytosis, unstable vital signs, and the abrupt onset of abdominal pain.
Statistical analysis
Statistical analysis was performed using SPSS version 17.0 software for Windows (SPSS, Inc., Chicago, IL). All clinical parameters considered to be potential risk factors for surgical outcomes were investigated by univariate and multivariate analyses. The χ2 test was used for univariate analysis. Values of P<.05 were considered statistically significant. Multivariate analysis was performed with the variables that were significant in the univariate analysis using binary logistic multiple regression tests with backwards elimination.
Results
Patient characteristics
The clinical characteristics of the 1257 patients are presented in Table 1. Of the patients, 375 were classified as elderly, and 301 were overweight or obese according to the World Health Organization Asia-Pacific classification.17,18 Of the patients, 480 had at least one comorbidity.
AGC, advanced gastric cancer; BMI, body mass index; EGC, early gastric cancer; LADG, laparoscopic-assisted distal gastrectomy; SD, standard deviation.
Analysis of risk factors for postoperative complications
Table 2 shows the results of univariate analysis of risk factors for postoperative complications. Age had a significant effect (above 65 years old versus below 65 years old, 8.5% versus 4.5%, P=.005), as did obesity (BMI above 25 kg/m2 versus below 25 kg/m2, 10.3% versus 4.3%, P<.001), comorbidity (presence versus absence, 7.9% versus 4.4%, P=.009), cerebrovascular disease (17.4% versus 5.5%, P=.038), heart disease (18.8% versus 5.4%, P=.008), hypertension (9.2% versus 4.7%, P=.004), and combined comorbidities (three or more comorbidities versus fewer than three comorbidities, 19.2% versus 5.4%, P=.014). Obesity had a significant effect on severe postoperative complications (BMI above 25 kg/m2 versus below 25 kg/m2, 3.7% versus 1.3%, P=.007). Table 3 presents the results of multivariate analysis for these predictive risk factors. Significant factors were obesity (P<.001; odds ratio 2.543, 95% confidence interval 1.555–4.156), old age (P=.006; odds ratio 1.970, 95% confidence interval 1.209–3.210), and heart disease (P=.014; odds ratio 3.257, confidence interval 1.275–8.318). Table 4 provides details of the postoperative complications in patients with these risk factors.
AGC, advanced gastric cancer; EGC, early gastric cancer.
BMI, body mass index; CI, confidence interval; OR, odds ratio.
The procedure was performed successfully on all patients. No patients required conversion to open surgery or other laparoscopic anastomosis techniques. The gross resection margin and the frozen section were negative in all cases.
Discussion
Gastric cancer is one of the most common malignancies in Korea and Japan and a leading cause of cancer-related deaths,11,12 although its incidence worldwide has been gradually declining. 19 Nevertheless, increasing numbers of elderly patients with comorbidities are suffering from gastric cancer because of improvements in surgical techniques, early detection, and higher life expectancy. 11
LADG has been shown to result in less pain, earlier recovery, and good cosmetic effects for patients with EGC, and surgeons choose this procedure for these reasons.20,21 Some studies have identified risk factors for postoperative complications following LADG, but these included many patients who underwent unstandardized LADGs.11,12,18 Surgical outcomes such as morbidity rate and operation time were poor before LADG procedures were standardized. The outcomes of unstandardized LADGs performed during a learning period are qualitatively different from those of standardized LADGs once the procedure has been mastered.
In the present study we enrolled only those patients who underwent a standardized form of LADG, in order to reduce the importance of the surgeon's experience as a risk factor. The development of a standardized LADG enables surgeons to become experienced in that procedure. After 2006, the mean operating time decreased sharply, and the length of postoperative hospital stay decreased slowly (Fig. 1).
Univariate analysis showed that old age (above 65 years), obesity (BMI above 25 kg/m2), and the presence of comorbidity, cerebrovascular disease, heart disease, hypertension, and combined (three or more) comorbidities were risk factors for postoperative complications of LADG. Multivariate analysis showed that only old age, obesity, and heart disease were associated with increased postoperative complication rates. Obesity had a significant impact on the rate of severe postoperative complications in the univariate analysis.
Recently, we reported that obesity is an important risk factor for postoperative complications after LADG. After we standardized our totally laparoscopic distal gastrectomy with gastroduodenostomy using endoscopic linear staplers without minilaparotomies, the surgical outcome in obese patients improved.22,23 Totally laparoscopic distal gastrectomy with gastroduodenostomy is now our preferred procedure for laparoscopic gastrectomy in obese patients, and in our hospital LADG is mainly performed on patients of normal weight. As a result, early surgical outcomes of LADG are constantly improving (Fig. 1).
Some surgeons have suggested that laparoscopy-assisted gastrectomy may be appropriate for elderly patients8,23 because, although there were more comorbidities in elderly patients, the surgical outcomes for elderly and younger patients were statistically similar. In our study, however, there was a clear difference between the overall postoperative complication rates of LADG for elderly and younger patients. Hence, although laparoscopy-assisted gastrectomy was more beneficial than open gastrectomy, old age appears to be a risk factor for postoperative complications of LADG.
Patients with heart disease had the highest rate of postoperative complications. This reflects the severity of the effects of comorbidities, as patients with heart disease had a large number of combined comorbidities (Table 4).
In conclusion, the present study shows that old age, obesity, and heart disease are risk factors for overall postoperative complications of LADG, and obesity is a risk factor for severe postoperative complications. We suggest that greater caution, or the use of less invasive surgical methods, is required to improve surgical outcomes in patients with these predictive risk factors.
Author Contributions
H.S.K. drafted the manuscript. H.S.K., M.G.K., K.B.S., I.S.L., and S.L. collected the data and performed the statistical analysis. H.S.K. and M.G.K. tracked the patients. J.H.Y. and B.S.K. designed the study and helped with the manuscript. All authors read and approved the final manuscript.
Disclosure Statement
No competing financial interests exist.