
Abstract
Abstract
Background:
The technique of totally laparoscopic total gastrectomy (TLTG) has been developed for gastric cancer, but its feasibility and surgical outcomes remain unclear. This is the first study comparing the early surgical outcomes of TLTG with those of conventional open total gastrectomy (OTG) for gastric cancer.
Patients and Methods:
Between January 2011 and December 2011, 139 patients underwent TLTG, and 207 patients underwent OTG for gastric cancer; surgical procedures were selected by means of preoperative diagnostic tests under T3N2M0. Clinicopathologic characteristics and early surgical outcomes in the two groups were compared retrospectively.
Results:
There were no significant difference in preoperative characteristics between the two groups, and the durations of surgery were not significantly different. However, TLTG was superior to OTG in terms of time to first flatus, time to commencement of soft diet, pain score (visual analog scale), need for analgesics, length of hospital stay, and overall postoperative complications (each P<.05). The median number of lymph nodes harvested was significantly higher in the TLTG group (37 versus 34; P=.039). Resection margins were negative in all patients.
Conclusions:
TLTG should be considered as a safe and practicable alternative to OTG for the treatment of gastric cancer. Moreover, it is less invasive and results in faster recovery than OTG.
Introduction
Patients and Methods
Patients
We reviewed the prospectively collected records of 346 consecutive patients who underwent total gastrectomy by TLTG or conventional OTG for gastric cancer between January 2011 and December 2011 at a single institution. The diagnosis was based on preoperative examinations including esophagogastroduodenoscopy, endoscopic ultrasound, and computed tomography scan. Patients with gastric cancer were selected by means of preoperative diagnostic tests under T3N2M0 according to the American Joint Committee on Cancer–International Union for Cancer Control 7th edition. 19 All patients underwent D2 lymphadenectomy. Clinical features and early surgical outcomes were compared in the two groups to assess the effectiveness of TLTG.
Surgical technique of TLTG
Posture and site of insertion of a trocar
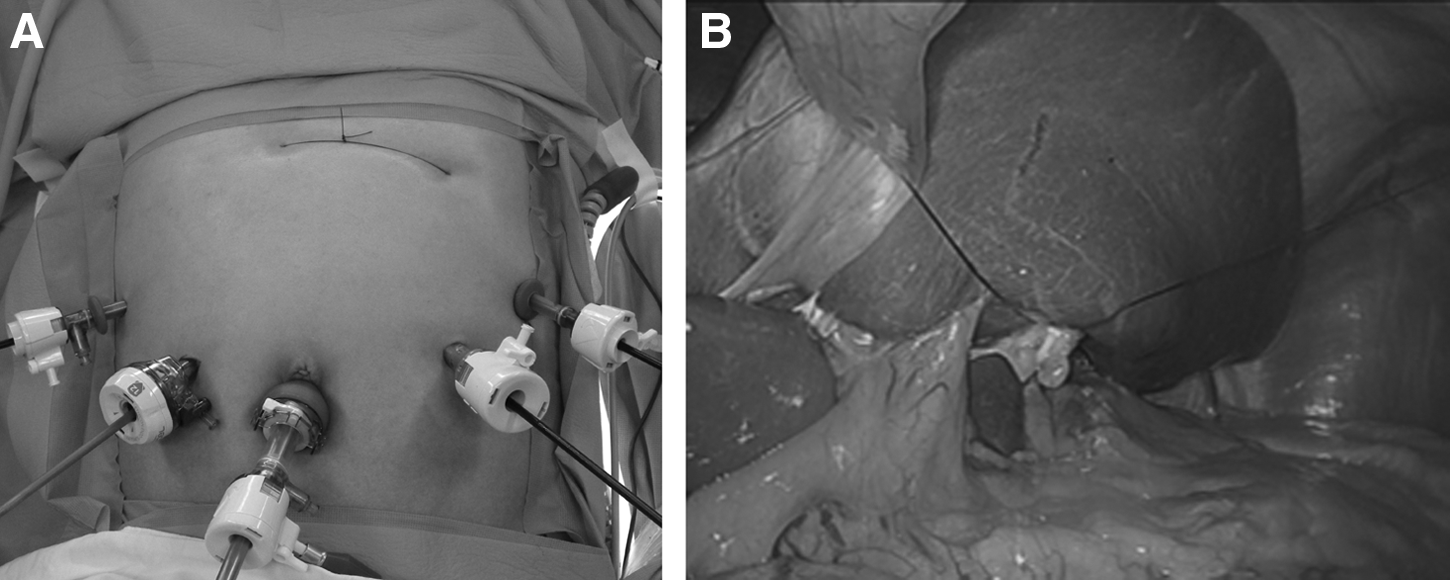
The patient was placed in the reverse Trendelenburg position. A carbon dioxide pneumoperitoneum was formed from the umbilical port, with pressure maintained between 12 and 15 mm Hg. Total gastrectomy was performed using four trocar ports placed in a U-shaped pattern (Fig. 1A). To retract the liver, the attachment site of the lesser omentum to the right diaphragmatic cruse was intracorporeally sutured, and then a thread pulled by a suture-passer was tied onto the skin in the xiphoid process area (Fig. 1B). If the operating field was not adequate, an additional 5-mm trocar was inserted into the epigastric area to retract the liver.
Dissection and removal of specimen
Dissection was begun by dividing the greater omentum from the midportion of the gastroepiploic arcade to the left gastroepiploic vessel. The lymph nodes around the left gastroepiploic and short gastric vessels were dissected, followed by the infrapyloric area. After dissection of the lymph nodes around the suprapyloric area, the duodenum was transected just below the duodenal bulb with an endoscopic linear stapler (Echelon™ Flex™ 60; Ethicon, Blue Ash, OH) with a closed stapler height of 1.5 mm. Subsequently, the lymph nodes around the common hepatic, proximal and distal splenic, celiac, and left gastric arteries were dissected (in that order), followed by dissection of the lymph nodes around the right paracardial and lesser curvature areas.
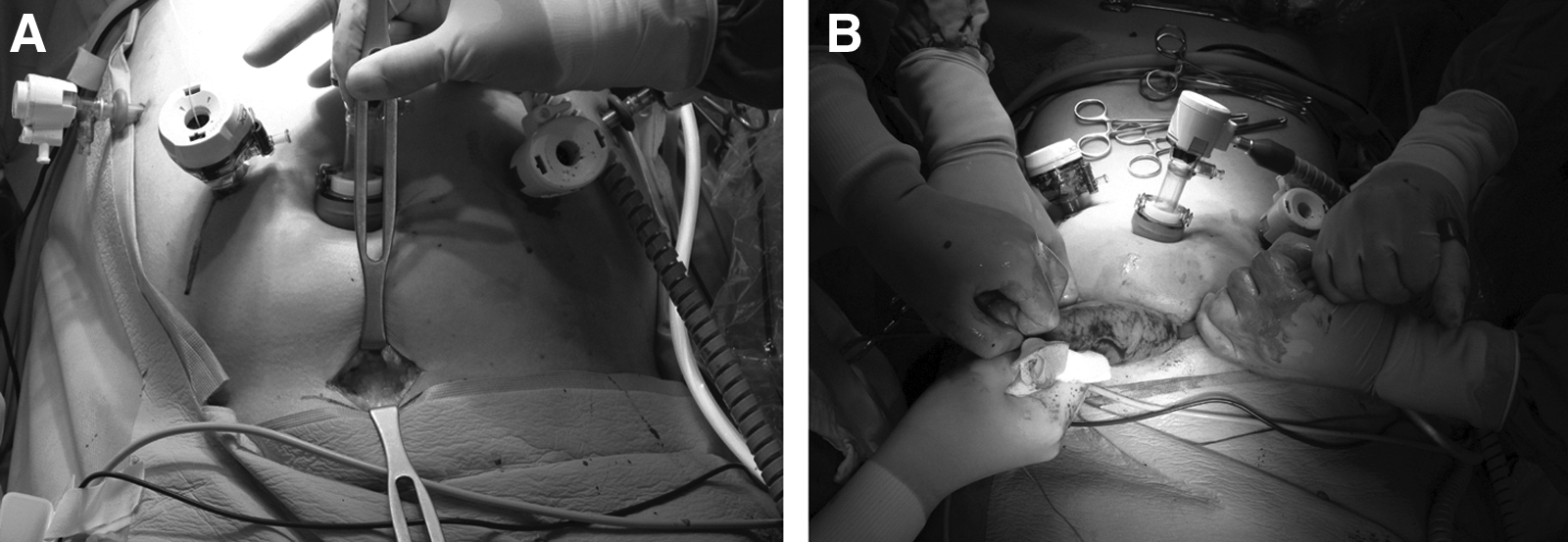
After all the lymph nodes were cleared, nearly two-thirds of the esophagus diameter was transected 2 cm above the gastroesophageal junction using the same type of endoscopic linear stapler (Fig. 2A), and the first intracorporeal suture was placed at the end of the stapled line to retract the esophageal stump (Fig. 2B). This suture was cut 15 cm from the esophageal stump, which was retracted by the first assistant during reconstruction of the EJ. The unstapled esophageal stump was then transected with laparoscopic scissors after the remnant stomach was grasped with a laparoscopic intestinal clamp to avoid cancer cell spillage (Fig. 2C). To make the lumen of the esophagus easier to detect, a second round of intracorporeal sutures was placed in the small esophagostomy of the esophageal stump, and it was pulled out of the abdomen through the right lower trocar; this prevented the esophageal mucosa and submucosa from slipping during reconstruction of the EJ (Fig. 2D). The specimen was subsequently removed through another 3–4-cm incision on the lower abdominal site, 2 cm from the suprapubic area (Fig. 3). After the specimen was removed, this incision site was closed by suturing the peritoneum to reinstate the pneumoperitoneum. The proximal resection margin of the specimen was examined pathologically.
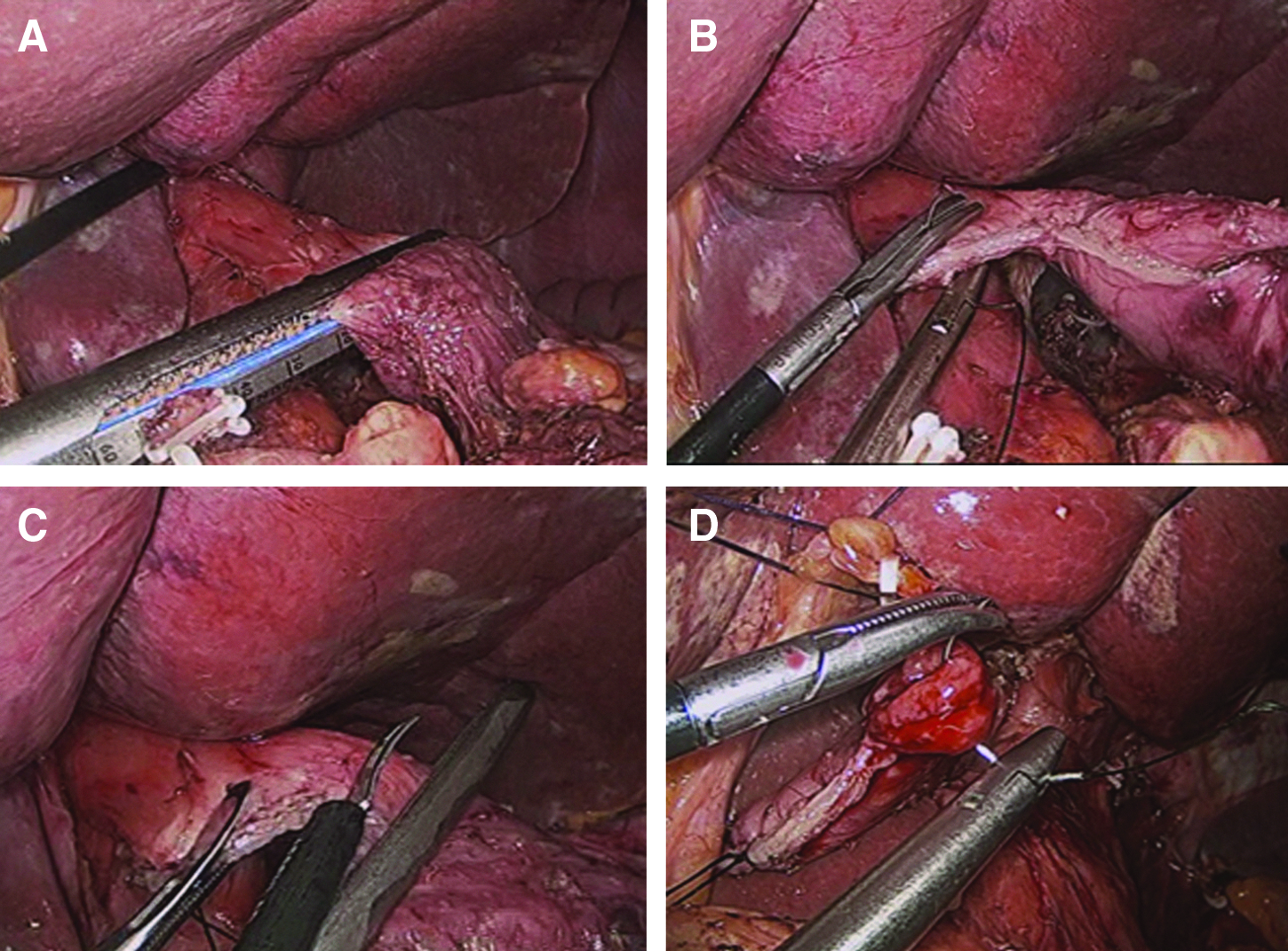
Making an esophageal stump.
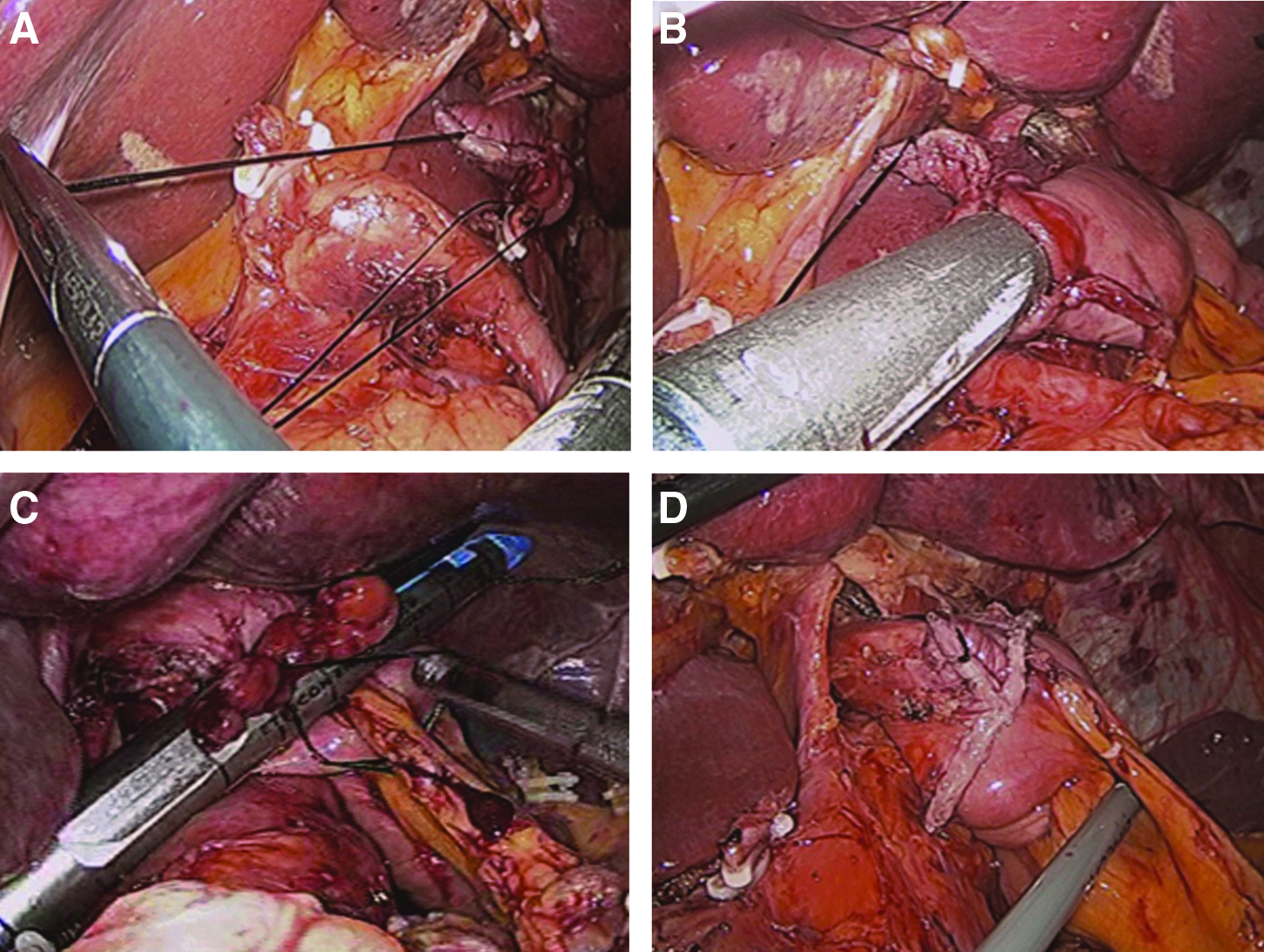
The jejunum was then divided 20 cm below the ligament of Treitz using an endoscopic linear stapler (Echelon Flex 60), and an efferent loop was turned in a counterclockwise direction to reconstruct the EJ. An enterostomy of the jejunum was made on the antimesenteric side of the Roux-en-Y limb using laparoscopic scissors, and an endoscopic linear stapler (ETS Straight™ 45; Ethicon) with a closed staple height of 1.5 mm was inserted into the esophagostomy and enterostomy of the jejunum to form an EJ (Fig. 4B).
Reconstruction of anastomosis
To make an EJ, the two sutures were retracted during the reconstruction. The first assistant retracted the first suture in the direction of the operator inside the abdominal cavity (Fig. 4A), and the second assistant retracted the second suture out of the abdomen through the right lower trocar. This procedure is important for preventing the esophageal stump from slipping into the thoracic cavity; it also guides the introduction of the anvil of the endoscopic linear stapler into the small esophagostomy of the esophageal stump during reconstruction of the EJ. An endoscopic linear stapler (ETS Straight 45) was inserted by the operator between the esophagostomy and enterostomy of the jejunum to form an EJ (Fig. 4B). After that, the entry hole was closed with three sutures for tissue approximation, followed by stapling with a laparoscopic linear stapler (Echelon Flex 60) (Fig. 4C). In some cases, further suturing was necessary to complete the closure. Then, to construct the jejunojejunostomy, two small enterostomies of the jejunum were made: (1) on the antimesenteric side of the jejunum, 40 cm below the EJ, and (2) on the antimesenteric side of the afferent loop. The endoscopic linear stapler (Echelon Flex 60) was inserted into these enterostomies of the jejunum to construct a jejunojejunostomy, and the entry hole was closed with the endoscopic linear stapler (Echelon Flex 60). Finally, the mesenteric and the Peterson defects were sutured, and the operation was finished.
Clinical analysis of surgical outcomes of laparoscopic gastrectomy
The clinical data obtained from medical records comprised patient age, gender, body mass index, American Society of Anesthesiologists score, and any previous abdominal surgery. Early surgical outcomes comprised operation time, postoperative change in hematocrit, time to first flatus, time to commencement of soft diet, pain score (visual analog scale [VAS]), postoperative length of hospital stay, number of analgesics administered, and postoperative complications. Pathologic results that were analyzed included tumor size, number of retrieved lymph nodes, resection margins, and cancer stage according to the Japanese Classification of Gastric Carcinoma, 3rd edition. 19
Preoperative hematocrit was checked before surgery, and postoperative hematocrit was checked at 7:00 a.m. on postoperative day (POD) 1. A postoperative complication was defined as any problem that required conservative or surgical treatment. Severe postoperative complications were defined as those requiring management by an endoscopic or interventional procedure or re-operation without general anesthesia. 20
Postoperative pain control consisted of intravenous, patient-controlled analgesia (fentanyl, 2,500 μg; ketorolac tromethamine, 180 mg; and ondansetron hydrochloride, 16 mg). Postoperative pain was assessed on a VAS. The score on the VAS was checked on POD 1 at 8:00 a.m., POD 3 at 8:00 a.m., and POD 5 at 8:00 a.m. We also calculated numbers of doses of analgesics required up to discharge to evaluate patients' postoperative pain.
Diatrizoate meglumine and diatrizoate sodium solution (Gastrografin®; Bayer Schering Pharma AG, Berlin, Germany) studies were performed on POD 3 to assess leakage in cases involving certain intraoperative events during reconstruction of the EJ. The day a soft diet was started was the day on which the patient felt comfortable enough to eat soft foods. Patients were discharged if they had no problems with such a diet, were generally comfortable, and demonstrated an absence of inflammatory conditions such as leukocytosis, unstable vital signs, and abrupt onsets of abdominal pain.
Statistical analysis
Statistical analyses were performed using SPSS version 20 software (SPSS, Chicago, IL). Patient data were analyzed using the Mann–Whitney U test for continuous variables and Fisher's exact test for categorical variables. A two-sided P value of<.05 was considered statistically significant.
Results
The clinical backgrounds of the 346 patients are shown in Table 1. There was no significant difference in age, gender, body mass index, American Society of Anesthesiologists score, and previous abdominal operation history between the OTG and TLTG group.
ASA, American Society of Anesthesiologists; OTG, open total gastrectomy; TLTG, totally laparoscopic total gastrectomy.
All the TLTG operations were successfully performed using intracorporeal esophagojejunal anastomosis with an endoscopic linear stapler. None of the TLTG group required conversion to open surgery or other laparoscopic anastomosis techniques. The extent of lymph node dissection was similar in the two groups. All the operations were curative.
Table 2 summarizes the early surgical outcomes. We found no differences between the OTG and TLTG groups in operation time or postoperative change in hematocrit. However, times to first flatus and to commencement of a soft diet and the length of postoperative hospital stay were significantly shorter in the TLTG group; in addition, the number of analgesic doses administered was significantly lower, and pain scored on the VAS lasted less time. Table 3 gives details of the postoperative complications in the two groups. There were significant differences in terms of overall and mild postoperative complications. Although the severe postoperative complication rate was similar in the two groups, there was no instance of anastomosis leakage in the TLTG group (Table 3).
Data are median (range) values as indicated.
OTG, open total gastrectomy; POD, postoperative day; TLTG, totally laparoscopic total gastrectomy; VAS, visual analog scale.
OTG, open total gastrectomy; TLTG, totally laparoscopic total gastrectomy.
Postoperative complications developed in 21.7% (45 cases) of the patients who received OTG. The postoperative complication rate for the TLTG group was significantly lower at 10.0% (14 cases). The mild postoperative complications (7 cases, 5.0%) in the TLTG group were partial obstruction of the anastomosis site (n=2), pneumonia (n=2), wound infection (n=1), paralytic ileus (n=1), and ischemia of the left lateral segment of the liver (n=1). Severe postoperative complications (7 cases, 5.0%) in the TLTG group were extraluminal bleeding (n=2), intraluminal bleeding (n=1), duodenal stump leakage (n=1), mechanical ileus (n=2), and transmesenteric herniation (n=1).
One of the instances of extraluminal bleeding in the TLTG group was stopped by laparoscopic suturing around the suprapancreatic area; the other patient had a large hematoma and was managed by inserting a pig-tail catheter with antibiotics and transfusion. The patient with duodenal stump leakage was managed by a combination of laparoscopic tube duodenostomy and conservative therapy, whereas the two cases with mechanical ileus were managed by laparoscopic adhesiolysis. Finally, the patient with internal herniation was managed by laparoscopic hernia reduction. There were no operative deaths in either group during the first 30 postoperative days.
Table 4 presents the pathology findings for the two groups. The groups did not differ significantly in terms of distal resection margin (P=.577), distribution of tumor depths (P=.059), or presence of lymph node metastasis (P=.056). However, there were significant differences in tumor size (P=.011), number of retrieved lymph nodes (P=.039), and proximal resection margin (P=.005).
Data are median (range) values as indicated.
AJCC/UICC, American Joint Committee on Cancer–International Union for Cancer Control; OTG, open total gastrectomy; TLTG, totally laparoscopic total gastrectomy.
Fluorography revealed smooth passage of contrast medium through the anastomoses in the TLTG group without leakage or stenosis (Fig. 5). Postoperative endoscopy demonstrated larger anastomoses in the TLTG group than in the OTG group 6 months after operation (Fig. 6).

Fluorography reveals smooth passage of contrast medium through the anastomosis without leakage or stenosis.
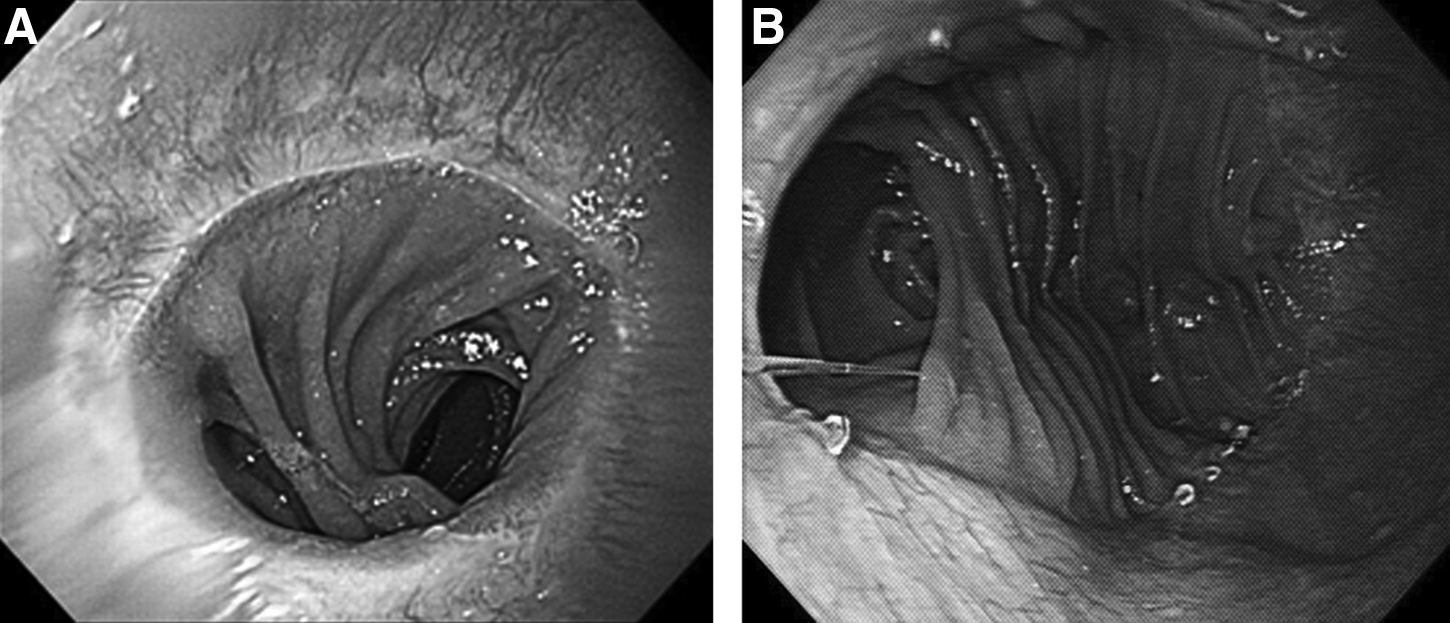
Postoperative endoscopy.
Discussion
Since the first report of laparoscopy-assisted distal gastrectomy in 1994, 3 the procedure has been widely adopted for gastric cancer.4,21,22 Recently, many workers have described totally laparoscopic distal gastrectomy using intracorporeal reconstruction. More recently, it has been shown to have several advantages over laparoscopy-assisted distal gastrectomy, including smaller wounds, less invasiveness, and greater security.9,10,23,24 The laparoscopic distal gastrectomy technique is fully established, and many patients have undergone laparoscopic distal gastrectomy for gastric cancer.9–13,23 In contrast, the number of laparoscopic total gastrectomies has been limited by the small number of expert surgeons who perform the procedure because of its technical challenges and lack of knowledge of long-term outcomes.14–18,25 Reconstruction of the EJ is technically one of the most difficulty aspects of the TLTG method. However, several investigators have reported on its safety and feasibility.14–18 Previously, we performed extracorporeal EJ and reported that laparoscopy-assisted total gastrectomy was superior to conventional OTG as it was associated with earlier bowel movements, less pain, and shorter hospital stays. 26 However, it is sometimes difficult to complete anastomoses by minilaparotomy in narrow and deep operating fields. In our experience, one difficulty is the process of clamping the distal esophagus through a small incision. Another is inserting a straight needle into the purse-string clamp and extracting it. A final difficulty is anvil insertion into the esophagus. This procedure tends to be affected by the size of the patient, and in obese patients we had to enlarge the incision. 26 Therefore, beginning in October 2008 we started performing intracorporeal EJ after laparoscopic total gastrectomy using an endoscopic linear stapler to exploit the advantage of laparoscopy-assisted total gastrectomy. We believe that we had reached a plateau in the learning curve with our 71st patient by January 2011, in terms of early surgical outcomes such as operation time, bowel movement, and postoperative complications. We had performed over 1500 laparoscopic gastrectomies before this study commenced and believe we are justified in claiming that we were well up the learning curve for performing TLTG. The purpose of this study was to establish a TLTG procedure using an endoscopic linear stapler and to compare it with the conventional procedure in gastric cancer.
Reconstruction of the intracorporeal EJ after laparoscopic gastrectomy is technically the most difficult aspect of TLTG. In our intracorporeal EJ method, we create two intracorporeal sutures to prevent slipping of the esophageal stump during reconstruction of the EJ: one at the end of the staple line and one at the small esophagostomy of the esophageal stump. The first assistant pulls the first suture toward the operator in the abdominal cavity, while the second assistant pulls the second suture thread toward the operator's side from outside the abdominal cavity. This retraction prevents the anastomosis from falling into the thoracic cavity while simultaneously making it safe. Furthermore, the operator is able to insert an endoscopic linear stapler without great difficulty between the esophagostomy and enterostomy of the jejunum to make an EJ. As a result, we are able to minimize the size of the remnant entry hole of the EJ and successfully complete the EJ (Fig. 4D).
Our study showed that TLTG using an endoscopic linear stapler could be performed safely with the intended benefit of less invasive surgery and favorable early surgical outcomes as assessed by more rapid postoperative recovery. In our series, the time required for TLTG did not differ from that for conventional OTG (137 versus 144 minutes, P=.381). When performed by a skilled and experienced surgeon, laparoscopic gastrectomy does not require any more time than open gastrectomy. 27
In our study, TLTG was indeed safe. The postoperative complication rate was lower than in the OTG group. Although there was no significant difference in severe postoperative complications between the two groups, there was no leakage of anastomosis in the TLTG group. However, in TLTG, one needs to create a wide operating view in order to construct the EJ safely. In our approach to TLTG, we are able to widen the operation field by retracting the liver. In addition, in our method we reconstruct the EJ with endoscopic staplers and three staggered rows of staples, whereas in OTG it is created by only two rows of staples; the three staggered rows of staples provide better staple line security than the two rows of staples. In addition, in terms of the lumen size for the esophagojejunal anastomosis, the lumen is larger in the TLTG (Fig. 6B) than with the double stapling method using a circular stapler (Fig. 6A). Among our patients there were 2 cases of mild anastomotic stricture of the EJ, and these cases were managed by conservative therapy. Clearly the TLTG technique provides acceptable surgical outcomes not only in terms of mild postoperative complications but also anastomosis-related complications.
At present, surgical resection is the treatment of choice for gastric cancer, but the extents of resection and lymphadenectomy during gastrectomy remain controversial. However, a recent randomized trial confirmed the survival benefit of D2 lymph node dissection while controlling for the morbidity of lymph node dissection.28–30 Therefore, we intend to continue performing D2 lymphadenectomy for gastric cancer. In this study, although the number of lymph nodes harvested was significantly lower in the TLTG group, the average number of lymph nodes harvested was over 30 in both groups; hence there was no clinical difference in this respect between the OTG and TLTG groups.
There are very few definite guidelines that cite literature sources and make recommendations regarding the desirable distance between tumor and resection margin. In a search of Medline we found only a few articles that made such recommendations.31–33 Bozzetti et al. 32 evaluated 343 patients with gastric cancer, including advanced cancer, with special reference to the outlines of the tumor, assessed grossly, together with other macroscopic or microscopic features of the tumor. They reported that neither proximal nor distal infiltration occurred at a distance >3 cm in lesions confined to the mucosa, submucosa, and muscularis. Jang et al. 33 reported that middle-third advanced gastric cancers that were treated by curative resection were not affected by the length of the proximal resection margin and the extent of gastric resection. In our procedure, the gross margin was free, and frozen-sections of the proximal resection line were examined to ensure that R0 resections had been performed.
In the present study, early surgical outcomes after TLTG were good, with reduced pain, rapid recovery of bowel movement, shorter hospital stay, fewer mild postoperative complications, and fewer anastomosis-related complications. We acknowledge that selection bias affecting the study populations in this retrospective study may have influenced the comparison of early surgical outcomes of OTG and TLTG. However, in this study, although TLTG aimed to cure via more radical lymphadenectomy, the oncologic safety of TLTG has not yet been established. Therefore, a large, randomized, and prospective study is needed to evaluate the effectiveness of TLTG for gastric cancer.
In conclusion, our TLTG method is safe and reliable. We believe that it should be preferred to OTG as a surgical treatment for gastric cancer. However, long-term follow-up is needed to evaluate any oncologic effects.
Footnotes
Disclosure Statement
No competing financial interests exist. H.S.K. drafted the manuscript. H.S.K., Beom S. Kim, I.S.L., and S.L. collected the data and performed the statistical analyses. H.S.K. followed up on the patients. J.H.Y. and Byung S. Kim designed the study and helped with the manuscript. All the authors read and approved the final manuscript.