
Abstract
Abstract
Background:
Several investigators have suggested methods for performing totally laparoscopic total gastrectomy (TLTG). However, even surgeons experienced in laparoscopic gastrectomy find it very hard to perform TLTG safely because it is a complex procedure. The aim of the present study was to evaluate the safety and efficacy of our TLTG method for the surgical treatment of early gastric cancer (EGC) located near the gastroesophageal junction (GEJ).
Subjects and Methods:
Between January 2010 and June 2011, 113 patients at a single institution underwent TLTG (n=90) or laparoscopic-assisted total gastrectomy (LATG) (n=23). Early surgical outcomes of the two techniques were compared to assess the effectiveness of TLTG for treating EGC near the GEJ.
Results:
The TLTG group included patients with higher body mass indexes (23.2 versus 22.2 kg/m2, P=.037) and more overweight patients (22.2% versus 4.0%, P=.041) than the LATG group. Despite this, the two groups had similar early surgical outcomes, such as mean operation time, intraoperative events, postoperative complications, time to first flatus, time to starting a soft diet, pain scores, analgesic requirements, and lengths of hospital stay.
Conclusions:
The results of TLTG were favorable even though a high proportion of the subjects were overweight. TLTG for EGC near the GEJ could be the best way to improve early surgical outcomes of EGC in overweight patients provided it is performed by surgeons who are experienced in laparoscopic gastrectomy.
Introduction
More recently, various types of intracorporeal esophagojejunostomy (EJ) using linear or circular staplers have been reported,12–16 but the best method has not been established. However, totally laparoscopic total gastrectomy (TLTG) procedures involve complex methods, especially the EJ and reconstruction without cancer cell spillage, that can be difficult to perform in patients whose gastric cancer is near the gastroesophageal junction (GEJ).
In the present study, we evaluated a novel method of TLTG using endoscopic linear staplers and demonstrated its clinical utility in the surgical management of EGC located near the GEJ.
Subjects and Methods
Patients
We reviewed the prospectively collected data on 113 consecutive patients who underwent laparoscopic total gastrectomy, including TLTG and laparoscopic-assisted total gastrectomy (LATG), for EGC located near the GEJ between January 2010 and June 2011 at Asan Medical Center (Seoul, Korea). A gastric cancer near the GEJ was defined as one for which the upper margin of the tumor was located within 3 cm of the GEJ on postoperative pathologic examination. All patients underwent D1+β or D2 lymph node dissections following the Japanese classification of gastric carcinoma. 17 Obesity was defined according to the World Health Organization Asia-Pacific Obesity classification, with patients classified as normal weight (body mass index [BMI] 18.5–24.9 kg/m2), overweight (BMI 25.0–29.9 kg/m2), and obese (BMI ≥30 kg/m2).18,19
Surgical technique
Position and insertion site of the trocar
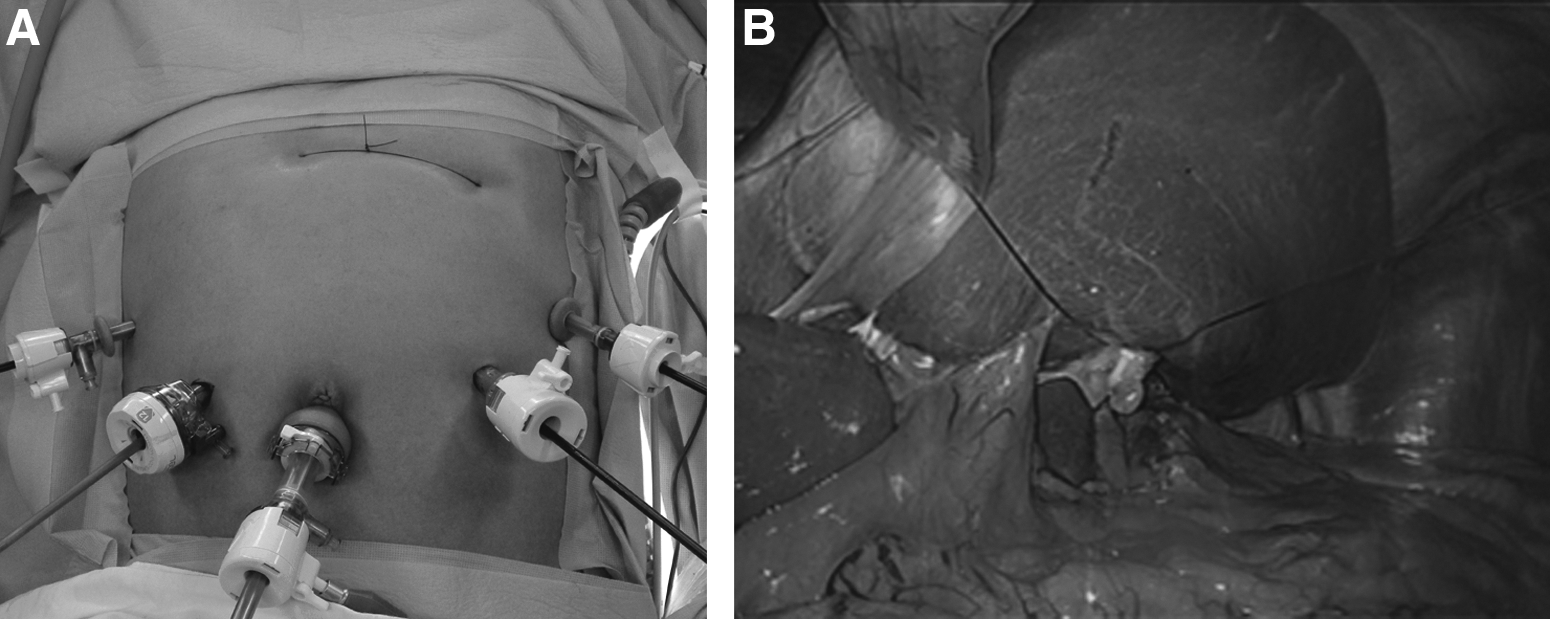
The patient was placed in the reverse Trendelenburg position. A carbon dioxide pneumoperitoneum was created through the umbilical port, with pressure maintained at 12–15 mm Hg. Total gastrectomy was performed using four trocar ports placed in a U shape (Fig. 1A). To retract the liver, the attachment site of the lesser omentum to the right diaphragmatic cruse was intracorporeally sutured, and then a thread pulled by a suture-passer was tied over the skin in the xiphoid process area (Fig. 1B). If the operating field was not sufficiently wide, another 5-mm trocar was inserted into the epigastric area to retract the liver further.
Dissection and removal of the specimen
Dissection was begun by dividing the greater omentum from the midportion of the gastroepiploic arcade to the left gastroepiploic vessel. The lymph nodes around the left gastroepiploic and short gastric vessels were dissected, and then the infrapyloric area was dissected. After lymph node dissection around the suprapyloric area, the duodenum was transected just below the duodenal bulb using an endoscopic linear stapler (Echelon™ Flex™ 60; Ethicon Endo-Surgery, a Johnson & Johnson Company, Landover, MD) with a closed stapler height of 1.5 mm. Subsequently, the lymph nodes around the common hepatic, proximal or distal splenic, celiac, and left gastric arteries were dissected (in that order), followed by dissection of the lymph nodes around the right paracardial and lesser curvature areas.
After all the lymph nodes had been cleared, nearly two-thirds of the esophagus diameter was transected 2 cm above the GEJ using an endoscopic linear stapler (Echelon Flex 60) (Fig. 2A), and the first intracorporeal suture was placed at the end of the stapled line to retract the esophageal stump (Fig. 2B). This suture was cut 15 cm from the esophageal stump, which was retracted by the first assistant during reconstruction of the EJ. The unstapled esophageal stump was then transected with laparoscopic scissors after the remnant stomach was grasped with a laparoscopic intestinal clamp to avoid cancer cell spillage (Fig. 2C). To make it easier to detect the lumen of the esophagus, a second round of intracorporeal sutures was placed at the small esophagostomy of the esophageal stump. This was retracted from outside the abdomen through the right lower trocar, to avoid the esophageal mucosa and submucosa slipping during reconstruction of the EJ (Fig. 2D). The specimen was subsequently removed through the umbilical port site by extending the incision into an I shape approximately 3–4 cm long. After the specimen was removed, the umbilical trocar was reintroduced, and three or four interrupted sutures were tied at the umbilical incision to reinstate the pneumoperitoneum. The proximal resection margin of the specimen was examined pathologically.
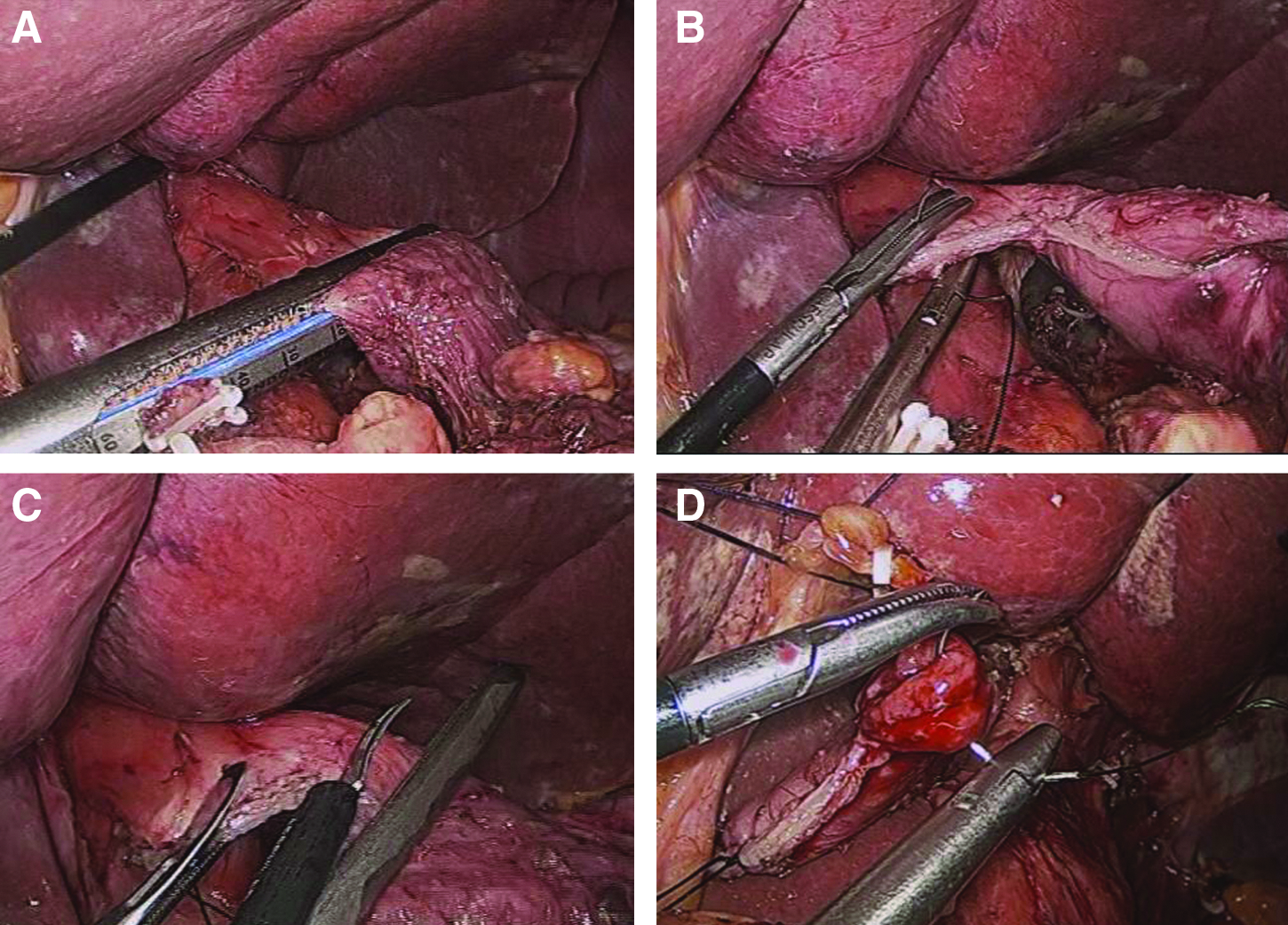
How to make an esophageal stump in totally laparoscopic total gastrectomy.
The jejunum was then divided 20 cm below the ligament of Treitz using an endoscopic linear stapler (Echelon Flex 60), and an efferent loop was turned in a counterclockwise direction to reconstruct the EJ. An enterostomy of the jejunum was made in the antimesenteric side of the Roux-en-Y limb using laparoscopic scissors, and an endoscopic linear stapler (ETS Straight™ 45; Ethicon Endo-Surgery) with a closed staple height of 1.5 mm was inserted into the esophagostomy and enterostomy of the jejunum to form an EJ (Fig. 3B).
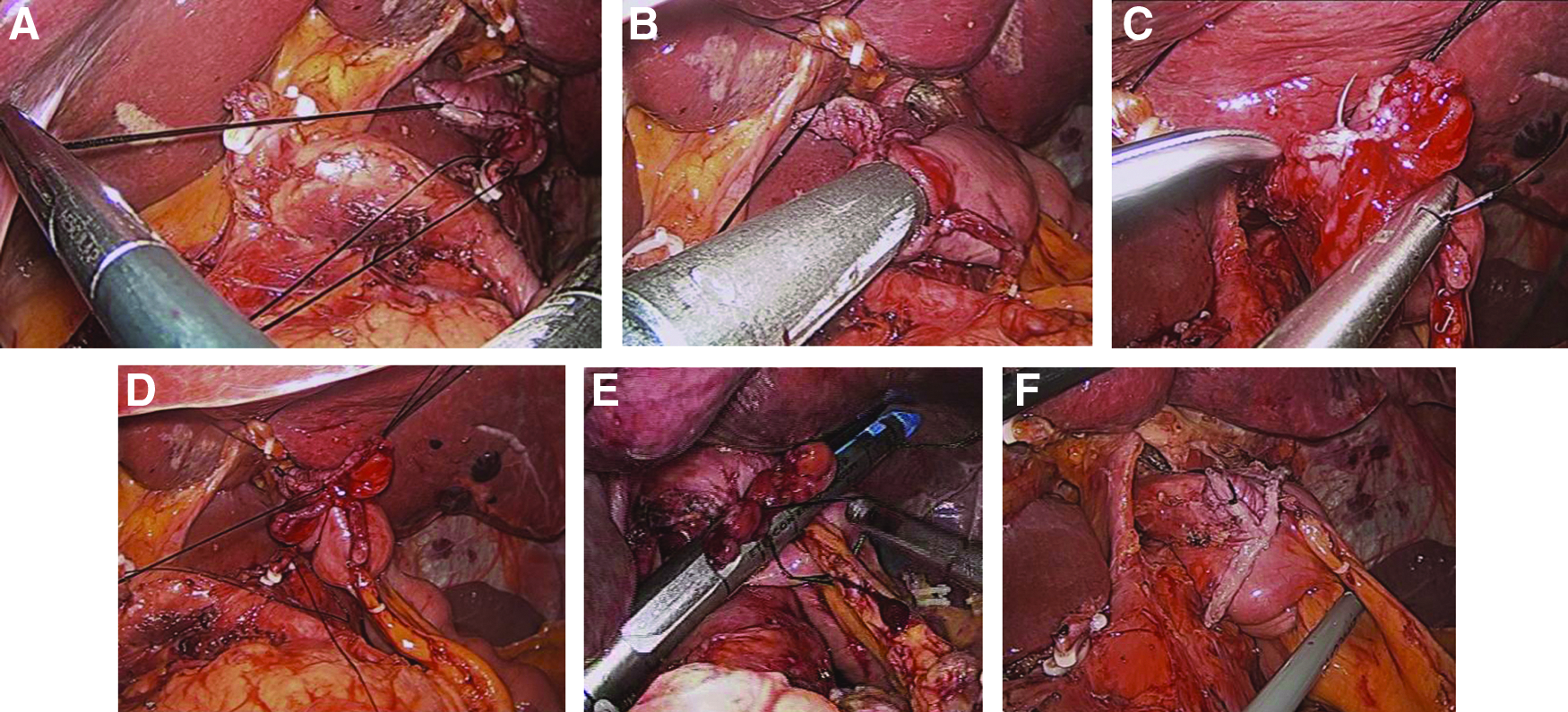
How to make an esophagojejunostomy in totally laparoscopic total gastrectomy.
Reconstruction of the anastomosis in TLTG
To make an EJ, two sutures were retracted during the reconstruction. The first assistant retracted the first suture in the direction of the operator inside the abdominal cavity (Fig. 3A), and the second assistant retracted the second suture through the right lower trocar from outside the abdomen. This procedure is important to prevent the esophageal stump slipping into the thoracic cavity; it also helps guide the anvil of the endoscopic linear stapler into the small esophagostomy of the esophageal stump during the reconstruction of the EJ. The operator inserted an endoscopic linear stapler between the esophagostomy and enterostomy of the jejunum to make an EJ (Fig. 3B). At this time, it is difficult but important to avoid inserting the endoscopic linear stapler into a “pseudo” lumen between the submucosal and muscular layers. After construction of an EJ, the entry hole was closed with three sutures for tissue approximation (Fig. 3C and D) and was then closed using a laparoscopic linear stapler (Echelon Flex 60) (Fig. 3E). In some cases, further suturing was needed to complete the closure. Then two small enterostomies of the jejunum were made: one on the antimesenteric side of the jejunum, 40 cm below the EJ, and the other on the antimesenteric side of the afferent loop. An endoscopic linear stapler (Echelon Flex 60) was inserted into the enterostomies of the jejunum to construct a jejunojejunostomy, and the stapler was also used to close the entry hole.
Reconstruction of anastomosis in the LATG
After the lymph nodes were removed, a mini-laparotomy incision 4–5 cm long was made in the epigastric area, and a wound protector was applied, as in laparoscopic-assisted distal gastrectomy. Essentially the same method was used to reconstruct the EJ as during conventional open surgery. It was reconstructed using a circular stapler (DST EEA™ 2535 [25-mm single-use stapler with 3.5-mm staples], blue; Covidien, Mansfield, MA) with a closed staple height of 1.5 mm. A side-to-side jejunojejunostomy was then performed extracoporeally via a hand-sewn anastomosis.
Finally, the mesenteric and Peterson defects were sutured, and the operation was completed.
Clinical analysis of surgical outcomes of laparoscopic gastrectomy
Clinical data obtained from medical records included patient age, gender, BMI, and American Society of Anesthesiologists score. Early surgical outcomes included operation time, intraoperative events, overall postoperative complications, severe postoperative complications, time to first flatus, time to starting a soft diet, pain score (visual analog scale), administration of analgesics, and postoperative length of hospital stay. Pathologic results that were analyzed included tumor size, number of retrieved lymph nodes, resection margins, and cancer stage according to the American Joint Committee on Cancer/International Union for Cancer Control, 7th edition. 17
A postoperative complication was defined as any condition that required conservative or surgical treatment. Severe postoperative complications were defined as conditions that required an endoscopic or interventional procedure or a re-operation with general anesthesia. 20
Postoperative pain control consisted of intravenous, patient-controlled analgesia (fentanyl, 2,500 μg; ketorolac tromethamine, 180 mg; and ondansetron hydrochloride, 16 mg). The degree of postoperative pain was assessed using a visual analog scale and by the number of additional doses of analgesics required until discharge from the hospital.
Gastrografin® (Bayer Schering Pharma AG, Berlin, Germany) was used on postoperative Day 3 to assess leakage and stenosis in patients who had an intraoperative event during reconstruction of the EJ. The time to starting a soft diet was given by the day on which the patient felt comfortable enough to eat soft foods. Patients were discharged when they had no problems eating a soft diet, were generally comfortable, and had no symptoms indicating inflammation, such as leukocytosis, unstable vital signs, and the abrupt onset of abdominal pain. The final decision about discharge was made by each patient.
Statistical analysis
Statistical analyses were performed using SPSS version 17.0 for Windows (SPSS, Inc., Chicago, IL). Data are expressed as mean±standard deviation values. Categorical variables were analyzed with the chi-squared test and Fisher's exact test, and continuous variables were analyzed with Student's t test. A P value of <.05 was considered statistically significant.
Results
Patient characteristics
The clinical characteristics of the 113 patients are presented in Table 1. Patients in the TLTG group had higher BMIs than those in the LATG group (23.2 versus 22.2 kg/m2, P=.037). This group also had more overweight and obese patients (22.2% versus 4.0%, P=.041). There were 3 obese patients (BMI ≥30 kg/m2) in the TLTG group but none in the LATG group.
Data are number of patients (%) unless indicated otherwise.
ASA, American Society of Anesthesiologists; BMI, body mass index; LATG, laparoscopic-assisted total gastrectomy; TLTG, totally laparoscopic total gastrectomy.
Early surgical outcomes
Table 2 shows early surgical outcomes in patients who underwent TLTG and LATG. None required conversion to open surgery, and none died within 30 days of the procedure. There were no significant differences in early outcomes between the two groups.
Data are mean±SD values or number (%).
LATG, laparoscopic-assisted total gastrectomy; POD, postoperative day; TLTG, totally laparoscopic total gastrectomy; VAS, visual analog scale.
Table 3 summarizes the postoperative complications. Severe postoperative complications occurred in 4 patients (4.4%) in the TLTG group: 2 had extraluminal bleeding, 1 had duodenal stump leakage, and 1 had an anastomotic stricture. Details of the management of these complications are given in Table 3.
LATG, laparoscopic-assisted total gastrectomy; TLTG, totally laparoscopic total gastrectomy.
Table 4 presents the pathology results for the patients who underwent TLTG and LATG. There were no significant differences between the two groups regarding tumors, number of retrieved lymph nodes, proximal resection margin, distal resection margin, distribution of tumor depth, and lymph node metastasis.
Data are mean±SD values unless indicated otherwise or number (%).
AJCC/UICC, American Joint Committee on Cancer/International Union for Cancer Control; LATG, laparoscopic-assisted total gastrectomy; TLTG, totally laparoscopic total gastrectomy.
Discussion
Gastric cancer is one of the most common malignancies in Korea, and laparoscopic gastrectomy is widely used for treating early gastric cancer. Several types of totally laparoscopic gastrectomy using intracorporeal reconstruction have recently been introduced, and we have previously reported the benefits of totally laparoscopic distal gastrectomy with gastroduodenostomy using endoscopic linear staplers. Although several articles have described TLTG using intracorporeal reconstruction, few evaluated the early surgical outcomes.12,21,22 In practice, TLTG is rarely performed because it is difficult to carry out when the EGC is near the GEJ, and laparoscopic esophagojejunal reconstruction is particularly difficult. There are no reports comparing the early surgical outcomes of TLTG and LATG. We have described above our method of performing TLTG safely, while reducing the possibility of cancer cell spillage.
The results of our study revealed no statistical differences in early surgical outcomes between TLTG and LATG, even though the TLTG group had a higher mean BMI and contained more patients with a BMI above 25 kg/m2 than the LATG group. This is significant because being overweight can be a risk factor for poor surgical outcomes, such as postoperative complications, delayed bowel movement, increased postoperative pain, and prolonged hospital stay, as we have suggested in previous reports of laparoscopic distal gastrectomy. Therefore, we believe that our method of TLTG achieves good results. In line with our previous findings for totally laparoscopic distal gastrectomy, we believe that avoiding laparoscopy and manipulation improves early surgical outcomes.
The practical procedures of TLTG and LATG differ in many respects. First, intracorporeal reconstruction using endoscopic linear staplers can enable a tension-free anastomosis and thus avoid damage to the surrounding structures. Second, although neither procedure involves manipulation of the operating field, TLTG requires a smaller incision (a 3–4-cm extension of the umbilical port) to remove the specimen by an endobag than LATG, and smaller incisions are less traumatic and less invasive.
However, even with direct sight of the surgical area, EJ can still be difficult to perform, especially in obese patients with thick abdominal walls,23,24 and the operating view needs to be widened. A wide operating field is also needed to ensure that the anastomosis is carried out safely because the resected esophageal stump can easily move into the thoracic cavity during TLTG. In our study, to create an adequate view for the esophagojejunal anastomosis, we performed the suturing at the attachment site of the lesser omentum to the right diaphragmatic cruse, and then a thread pulled by the suture-passer was tied over the skin in the xiphoid process area (Fig. 1B). By retracting the liver in this way, the operating field was widened, and the EJ could be reconstructed safely. To prevent the esophageal stump from slipping and to perform the anastomosis in the abdominal cavity, two intracorporeal sutures were made: one at the end of the staple line and one at the small esophagostomy of the esophageal stump. The first suture was placed at the end of the stapled esophageal stump, which was retracted by the first assistant during the reconstruction of the EJ. The second suture was made at the small esophagostomy of the esophageal stump, which was retracted from the abdomen through the right lower trocar. To widen the operating field and prevent esophageal slippage during the reconstruction of the EJ, the first assistant pulled the first suture thread toward the operator in the abdominal cavity, whereas the second assistant pulled the second suture thread toward the operator from outside the abdominal cavity. This retraction was to prevent the anastomosis from falling into the thoracic cavity while also keeping it safe. Furthermore, the operator was able to insert an endoscopic linear stapler without great difficulty between the esophagostomy and enterostomy of the jejunum to create an EJ. As a result, we were able to minimize the size of the remnant entry hole of the EJ on completing the EJ. This also enabled us to confirm the safety of both the posterior and anterior sides of the anastomosis (Fig. 3F). Using our TLTG method, we could obtain a wider operating field and effective retraction of the esophageal stump. Therefore we could safely insert an endoscopic linear stapler into the true lumen of the esophagus and reconstruct the intracorporeal EJ safely.
Postoperative morbidity after LATG is in the range of 17%–27%.25–30 In this study, the postoperative morbidity rate after TLTG was 11.1%. Reports suggest that leakage of the esophagogastric anastomosis causes complications in 5%–25% of cases.31–33 Clinically obscure ischemia of the anastomosed stomach and errors in surgical technique are major reasons for this.34,35 Anastomosis leaks during EJ generally cause more deaths than other gastrointestinal anastomotic leaks because they can easily lead to suppurative mediastinitis and subsequent septicemia and multiple organ failure.31,33 Although there was no significant difference in severe postoperative complications in the two groups, there was no leakage of anastomoses in the TLTG group, whereas two patients in the LATG group suffered leakage. In LATG, it is sometimes difficult to complete anastomoses by mini-laparotomy in narrow operating fields, whereas TLTG has a wide operating view with direct sight. In our experience, one difficulty with LATG is clamping the distal esophagus through a small incision. Another is inserting a straight needle into the purse-string clamp and extracting it. A third is inserting the anvil into the esophagus. Together with the limited view, these difficulties make it hard to carry out safe reconstruction of the EJ. Moreover, LATG tends to be affected by the size of the patient, and the incision has to be enlarged in obese patients. 36
However, in TLTG, a wide operating view is needed to construct the EJ safely. In our study, we widened the operating field by retracting the liver. In addition, we reconstructed the EJ with endoscopic staplers and three staggered rows of staples, which are more secure than the two rows of staples used in LATG.
Many operative events and postoperative complications arose during the learning curve for TLTG. In early 2010, extraluminal bleeding occurred because of insufficient hemostasis by the laparoscopic coagulation scissors; hemostasis is now adequate. Initially, operative events such as tearing of the esophageal mucosa occurred during reconstruction, and further suturing was necessary to complete the closure. There were also 4 cases of stricture of the EJ. However, with experience, our surgical outcomes have improved, and there are now fewer complications.
In conclusion, the present study suggests that the TLTG method for surgical treatment of EGC near the GEJ is feasible and safe. TLTG could be the best way to improve early surgical outcomes, particularly for overweight patients. However, a well-designed randomized controlled trial is needed to compare the short-term and long-term outcomes of TLTG and LATG in a larger number of patients.
Footnotes
Disclosure Statement
No competing financial interests exist.