
Abstract
Abstract
Background:
After promising results were obtained from studies in large animals, a technique using indocyanine green (ICG) is being introduced for sentinel lymph node (SLN) biopsy in colon cancer patients.
Subjects and Methods:
Colon cancer patients without clinical signs of metastatic disease, presenting at the VU University Medical Center (Amsterdam, The Netherlands) or Kennemer Gasthuis (Haarlem, The Netherlands), were asked to participate in the study. During laparoscopy, a subserosal injection of 2.5 mg of ICG diluted in 1 mL of 0.9% NaCl plus 2% human albumin was performed using a percutaneously inserted long rigid or flexible needle. After injection, a near-infrared laparoscope (Olympus Corp., Tokyo, Japan) was used for lymph flow and SLN visualization. The SLNs were laparoscopically harvested and analyzed by a senior pathologist using multisectioning and immunohistochemistry.
Results:
Fourteen patients were included (six women, eight men), with a median age of 75.5 (interquartile range [IQR], 67.8–81.0) years and a median body mass index of 25.1 (IQR, 22.7–26.0) kg/m2. Median tumor diameter was 4.5 (IQR, 3.4–7.0) cm. At least one SLN was identified in all patients, with a median number of 2.0 (IQR, 2.0–3.3) SLNs. The median time between injection and identification of the SLN was 15.0 (IQR, 13.3–29.3) minutes. Positioning of the needle tip into the subserosal layer was found to be more effective using the flexible needle. When this flexible needle was used, less spill of dye was observed. All SLNs were negative. We observed four false-negative nodes, all after using a rigid needle. None of the patients showed an adverse reaction to the ICG injection.
Conclusions:
Preliminary results of laparoscopic sentinel node identification using a near-infrared dye show this procedure is safe and feasible. It was possible to detect lymph nodes in all patients. Large tumor size, drainage to adjacent lymphatic vessels, and the use of a rigid needle might contribute to false-negative nodes.
Introduction
The gold standard for colon cancer treatment today is a segmental resection including resection of all regional lymph nodes. For tumor staging, lymph nodes are harvested manually by the pathologist and are assessed using single-section examination followed by hematoxylin and eosin (H&E) staining. The outcome of this histopathological examination is the most important indication for adjuvant chemotherapy. Following this current strategy for colon cancer management, up to 30% of Stage I and II patients (by definition, node negative) will eventually develop metastases and die from colon cancer. 4 This might be caused by a suboptimal pathological examination of the lymph nodes. Using the conventional single-section H&E staining, only a limited part of the lymph node is investigated, and therefore (micro)metastases can be easily missed. Identification of the SLN, subsequent serial section, and the use of immunohistochemistry, as used in other forms of cancer, might be of value in upstaging node-negative colon cancer patients. Until now, tracers currently used for SLN identification in colon cancer patients have shown limitations such as poor tissue penetration of blue dye in the case of a fatty mesentery and signal interference if the SLN is located near the tumor when using radioactive tracers.5,6 Here we describe a new minimally invasive technique for SLN mapping in patients with colon carcinoma.
Subjects and Methods
The study protocol was approved by the ethical committee of the VU University Medical Center, Amsterdam, The Netherlands, and by the local ethical committee of the Kennemer Gasthuis, Haarlem, The Netherlands (registration number NL2461302908). Patients at least 18 years old, who gave oral and written informed consent, were included in this validation study. Right after the SLN procedure, each patient received standard surgery. Exclusion criteria were pre- and perioperatively gross lymph node involvement, distant metastases, advanced disease with invasion of adjacent structures, prior colorectal surgery, metastatic or T4 disease discovered during intraoperative staging, contraindications to laparoscopy, rectal cancer, and allergy to iodine. Main study end points were identification rate of SLNs, number of false-negative SLNs, number of patients who are upstaged by ultrastaging techniques, number and status of aberrant lymph nodes, and accuracy and conformity of the SLN status.
Surgical procedure
Patients meeting the inclusion criteria were prepped, draped, and placed under general anesthesia. Laparoscopic access was obtained in the traditional fashion, and abdominal exploration was performed to rule out intra-abdominal metastases. Injection of the dye was performed by the same surgeon (W.J.H.J.M.) in all cases. In the first 7 patients a rigid spinal needle was used for injection. During the final 7 patients two different kinds of flexible endoscopic needles were used for transcutanous injection (sclerosering and Wang needle). During two of the seven procedures a sclerosering needle (FH Medical BV, Veenendaal, The Netherlands) with a tube length of 230 cm, tube diameter of 2.35 mm, and needle projection of 5 mm was used. In 5 patients a Wang transbronchial cytology needle (ConMed Corp., Utica, NY) with a tube length of 130 cm, tube diameter of 1.9 mm, and needle projection of 13 mm was used. The short tube length and small diameter of the Wang transbronchial cytology needle, allowed for a more controlled way of injecting tracer material. Alternatively, using a longer flexible needle makes it easier to place the needle tip in the subserosal layer of the colon and keep it positioned during tracer administration. The use of indocyanine green (ICG)/albumin solution was based on previous results obtained from animal studies. 6 First, 1.0 mL of saline was injected into the colon wall to ensure correct placement of the needle (confirmed by a raising bleb), followed by the injection of ICG (ICG-Pulsion; Pulsion Medical Systems AG, München, Germany) solution. The ICG solution consisted of 25 mg of ICG diluted in 1.0 mL of human albumin (20%) and 9 mL of NaCl (0.9%). One to three peritumoral injections were performed depending on tumor size. The maximum injected volume contained 1.0 mL of ICG solution (<2.5 mg). For lymph vessel and SLN identification, a newly developed, CE-approved, near-infrared (NIR) laparoscope (Olympus Corp., Tokyo, Japan) was used. The system consisted of a Visera laparoscopic system equipped with a xenon light source for excitation of ICG and filter sets for optimal wavelength selection. The optic device used has adjusted coated lenses to allow for optimal infrared transparency. A more detailed description of this laparoscope was previously published. 6
The first one to four lymph nodes, accumulating tracer material and presenting as bright fluorescent dots using the NIR modes, were defined as SLN(s). After identification, the SLN or SLNs were being harvested laparoscopically. After SLN harvesting, conventional laparoscopic medial to lateral oncologic resection was conducted.
Pathological assessment
A senior pathologist manually searched the fresh resection specimen for lymph nodes. Lymph nodes found were bisected along the longest axis and embedded in paraffin. All lymph nodes were stained with H&E. If the SLNs were tumor negative after routine H&E staining, the SLNs were sectioned (3–4 μm thick) at 150-μm intervals and examined at three levels with H&E as well as using immunohistochemistry with the epithelial marker CAM 5.2. Metastases between 0.2 mm and 2.0 mm were referred to as micrometastases. Metastases smaller than 0.2 mm were described as isolated tumor cells.
Results
Fourteen patients were included: six women and eight men. The median age of the patients was 75.5 (interquartile range [IQR], 67.8–81.0) years. Patients had a median body mass index of 25.1 (IQR, 22.7–26.0) kg/m2. The tumors were located in the sigmoid (n=6), colon transversum (n=1), cecum (n=5), and colon ascendens (n=2). The median diameter of the tumors was 4.5 (IQR, 3.4–7.0) cm (Table 1).
BMI, body mass index.
During all procedures the flow of dye in the lymphatic vessels could be followed in real time by the bright fluorescent signal (Fig. 1). Proper excitation of the dye occurred almost immediately after ICG injection (approximately 1 minute). The absence of autofluorescence of intra-abdominal structures and a high signal-to-noise ratio made lymph vessel and lymph node identification possible (Fig. 2). During all procedures at least one to four lymph nodes could be identified and harvested. The (sentinel) lymph nodes were being dissected using the white-light modus of the NIR system. Guided by the greenish color of the ICG itself and by switching back to the NIR modes, complete removal of the (sentinel) node could be optimized. There was no need for conversion in any of the procedures. During five procedures more than one injection was used because of the size of the tumor (Table 2). The median time between dye injection and SLN identification was 15 (IQR, 13.3–29.3) minutes. Laparoscopic harvesting of (sentinel) lymph nodes was successful in all 14 patients (100%). The median peroperative number of SLNs found was 2.0 (IQR, 2.0–3.3), and the median number of non-SLNs found by the pathologist in the resected specimen was 10.5 (IQR, 4.8–22.3).
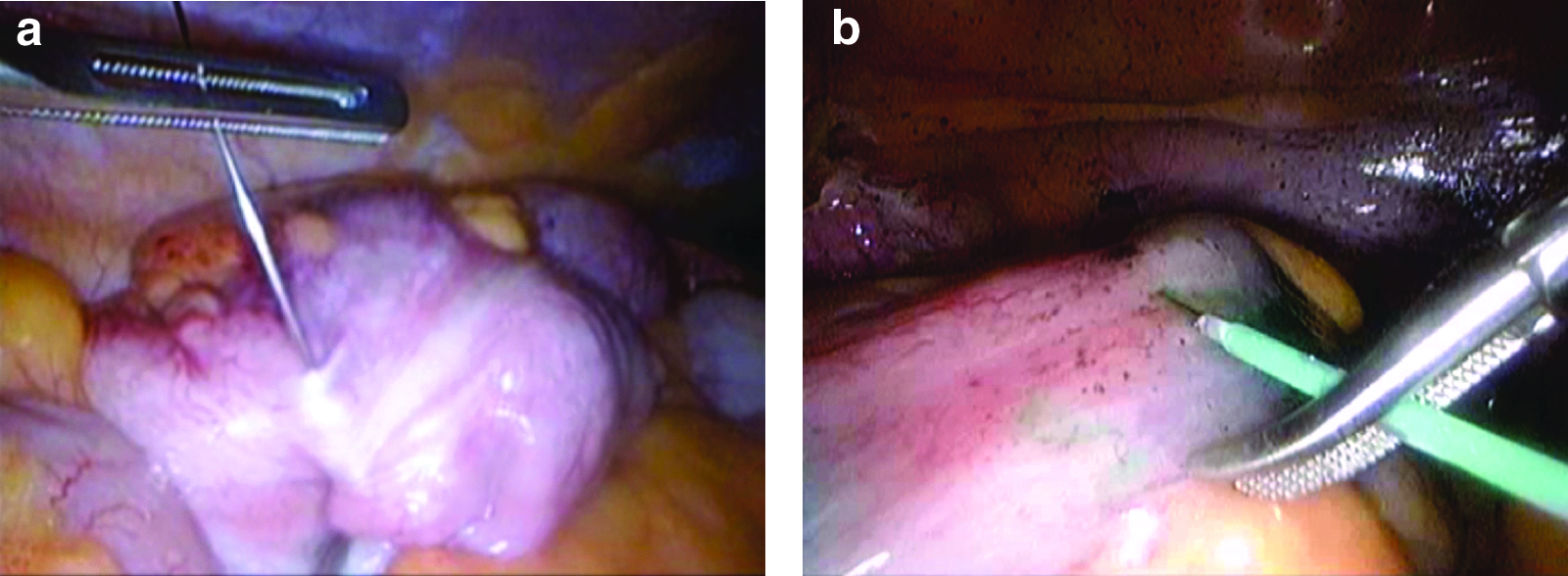
Positioning of the needle near the tumor with
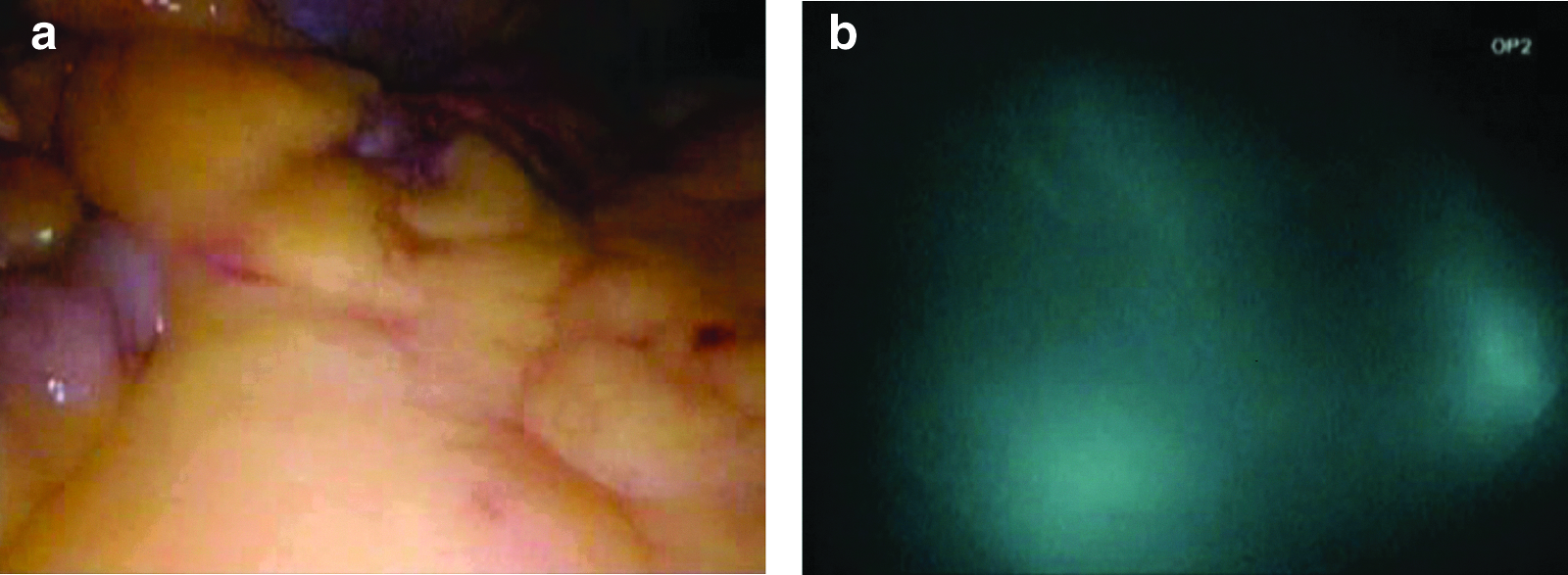
Observation of mesentery with two lymph nodes
Each injection consisted with 1 mL of indocyanine green/human albumin/NaCl solution.
SLN, sentinel lymph node.
In 10 patients no metastases were found during evaluation of the SLN and non-SLNs. In 4 patients a positive non-SLN was found, whereas the presumed SLN was negative (false-negative SLN). No adverse events or complications occurred as a result of laparoscopic SLN identification using ICG.
The usage of a rigid spinal needle made the procedure technical more difficult. In particular, correct positioning of the needle tip into the subserosal layer, for example, depended much on the right angle between colon wall and needle. More spillage of dye occurred when using the rigid needle in contrast to the flexible (Wang) needle. Intra-abdominal spillage of dye made the SLN identification difficult in the first 5 cases, because of the fluorescent abdominal cavity. Time between injection and lymph node identification took longer when spillage occurred. During the final 7 cases a flexible endoscopic needle was used. Positioning of the needle tip into the colon wall was found to be much easier, especially when using the Wang transbronchial cytology needle. No spillage was reported during the final seven procedures. We also observed that NIR light is able to penetrate relatively deeply through living tissue. During our study lymph nodes located 1.5 cm in the fatty tissue could be identified.
Discussion
This study was conducted to describe and assess the feasibility of a new technique using NIR dyes for SLN detection and harvesting in colon cancer patients.
The major issue in our current study is occurrence of the false-negative (sentinel) nodes in 4 patients. We believe the following problems contribute to these findings:
1. Correct placement of the needle close to the tumor is essential for adequate lymph node mapping. However, if the peritumoral injection of the NIR dye is not close enough to the tumor or in the case of big tumors, this can lead to drainage into adjacent lymph vessels instead of the vessels draining on the SLN. As a result SLNs will be missed. 2. During the first seven procedures a rigid spinal needle was used for dye injection. Correct positioning of the needle tip was found to be difficult and occasionally lead to spillage of dye. During the final seven procedures the rigid needle was replaced by a flexible needle. Using a flexible needle, positioning of the needle tip into the colon wall was found to be easier. Intra-abdominal space is limited, and maneuvering of a flexible needle was shown to be more manageable, making finding a correct position easier. 3. Also, the SLN mapping in large-sized tumors (>7 cm in diameter) seems to show less favorable results regarding sensitivity. Obliteration of the lymph vessels by ingrowth of tumor tissue or obstruction by gross metastases in the lymph node, resulting in an alternative route of lymph flow, could be an explanation.
During animal experiments we observed the problem of dye leakage. 6 Spilled ICG will stick to intra-abdominal tissues, resulting in a fluorescent abdominal cavity. Rinsing the abdominal cavity with saline after spillage at the injection site does solve this problem only slightly. We addressed this problem by a pre-injection of saline to assure a correct localisation of the needle. Correct placement of the needle gives bulging of the colon wall.
Other injection strategies could be interesting for future studies. Perioperative colonoscopic injection, for example, could be an alternative. 7 When spillage of dye occurs, the tracer material will leak into the lumen of the colon, making spillage less of a problem. During animal experiments this approach showed favorable results (unpublished data). Different injection routes like intratumoral or submucosal injection by per- or preoperative colonoscopy is a subject of our future studies.
SLN mapping using patent blue and radioisotope tracers, analogous to breast cancer, is noted to have limitations when used in colon cancer patients.8,9 Some authors have concluded that the SLN concept is not suitable for colon cancer patients because high false-negative ratios were seen.8,9 However, results from a meta-analysis addressing sensitivity of the SLN procedure in colorectal cancer patients showed favorable results when selecting for high-quality studies. Sensitivities as high as 90% with a detection rate of 96% could be achieved. 10 In addition, recently published studies showed high sensitivity rates when the procedures were accurately performed.11,12 The type of dye chosen might also have confounded the results of some studies. Ink, for example, show poor tissue penetration, especially in patients with extensive intra-abdominal fat. When radioactive tracers are used, the signal from the injection site might interfere when the SLN is localized nearby the tumor. NIR dyes with their unique characteristics could help to overcome these problems. We clearly show here that lymph nodes in obese patients can be adequately identified using ICG up to 1.5 cm in fatty mesentery.
During our procedures we diluted ICG with saline and human albumin. This was based on previous animal experiments. 6 During these experiments we were not able to detect SLNs when using plain ICG. We could identify lymph vessels, but it seemed that ICG washed through the lymph nodes and did not accumulate in the nodes. After human albumin was added, SLNs could be identified. In addition, human albumin seems to increase the fluorescent capacities of ICG. Other groups reported good kinetics using only ICG.13,14 The need for human albumin and its concentration for ICG dilution also deserve further analysis.
The period of time between dye injection and SLN identification varied from 2.5 to 40 minutes. Tracer material used was equal during all cases. Intra-abdominal lymph node drainage patterns are not consistent, and SLNs can be located at different locations. Exploring the abdomen in search for the SLN can be time consuming, especially when spillage of dye occurred, coloring more intra-abdominal anatomic structures fluorescent.
Lymph vessels can be identified within seconds after dye injection when they are located at the surface. Depending on the depth of localization, a solid amount of dye entrapped in the lymph node will be needed to ensure enough tissue penetration for identification. In the patient in whom the sentinel node was identified in 2.5 minutes, the lymph node was located near the tumor and at the surface of the mesentery.
ICG was used because this dye is clinical grade. Several companies worldwide are busy developing new NIR dyes for clinical purposes. Toxicological studies are needed, but they are time consuming, and the first clinical-grade dyes are still being awaited. These new dyes are reputed to have better fluorescent characteristics compared with ICG. Nevertheless, we demonstrated that ICG was capable of SLN detection by using the NIR modes of an NIR laparoscope.
Conclusions
Laparoscopic (sentinel) lymph node mapping using ICG/albumin/NaCl solution is feasible in patients with colon cancer. However, this novel technique needs more refinement. In particular, the site of injection (subserosal or intramucosal injection and intra- or peritumoral injection) is a point of discussion. More studies concerning the concentration and amount of dye to be injected, the additional value of human albumin, method of injection, and validation of the SLN technique using ICG are warranted.
Footnotes
Acknowledgments
This study was funded by the Cancer Center Amsterdam Foundation, Amsterdam, The Netherlands. Olympus provided the near-infrared system, which the authors could use on an unrestricted basis.
Disclosure Statement
No competing financial interests exist.