
Abstract
Abstract
Background/Aim:
Single-incision laparoscopic fundoplication is not widespread because of its technical difficulty. An additional stay suture or retractor is often needed for liver retraction during the procedure. Here, we share our 7 cases to demonstrate the feasibility of transumbilical single-incision laparoscopic fundoplication with a new technique for liver retraction without any stay suture or retractor.
Patients and Methods:
From March 2010 to October 2011, 3 patients with achalasia underwent a transumbilical single-incision laparoscopic Heller–Dor operation, and 4 patients with hiatus hernia underwent transumbilical single-incision laparoscopic hernioplasty and Nissen fundoplication. The procedures were attempted transumbilically by using three rigid trocars (one was 10 mm, and two were 5 mm) inserted through the 2-cm umbilicus incision. Conventional laparoscopic instruments were used. Adequate retraction of the liver was achieved by binding the lateral left lobe of the liver to the diaphragm with cyanoacrylate.
Results:
The pneumoperitoneal time was 115–170 minutes, and blood loss was 15–50 mL. There were no intra- or postoperative complications. The hospital stay was under 6 days for all patients. The umbilical incision healed well with satisfactory cosmetic effect.
Conclusions:
The transumbilical single-incision laparoscopic technique in the treatment of achalaisa and hiatus hernia is feasible for an experienced laparoscope surgeon with excellent cosmetic effect. Cyanoacrylate, when used as described, offers a safe and simple solution to the problem of liver retraction, thus obviating the need for a stay suture or liver retractor.
Introduction
Patients and Methods
A retrospective review of all patients who underwent TSILF from March 2010 to October 2011 was performed. Data including pneumoperitoneal time, intraoperative complications, blood loss, hospital stay, and development of postoperative complications were collected. There were 4 male and 3 female patients treated using this procedure, ranging in age from 14 to 70 years old. The body mass index at the time of the operation ranged from 19.6 to 24.4 kg/m2. The diagnosis of achalaisa or hiatus hernia was made by gastroscopy, upper gastrointestinal barium meal fluoroscopy, pre-procedure manometry, and upper abdominal tomography. The operation was offered to patients according to criteria specifying clarification diagnosis of achalasia with failure of medical therapy and endoscopic pneumatic dilatation and of hiatus hernia complicated with Barrett's esophagus and severe gastroesophageal reflux or repeated episodes of asthma or hoarseness. Patients with history of upper abdominal operation, esophageal cancer, diffusive esophageal spasm, severe coagulation disturbance, or type IV hiatus hernia were excluded. The nature of the surgical procedure and the risks involved were explained before consents were obtained, and all patients provided complete informed consent. The study was performed under institutional review board approval. The demographic data for each patient are shown in Table 1.
BMI, body mass index.
The procedures were performed with the patients under general anesthesia in the supine position with legs parted and the left shoulder raised 15°–20°. The viewing monitor was placed above the patient's left shoulder, with the surgeon standing between the patient's legs and the camera operator on the patient's right side. Pneumoperitoneum was established by using the closed Veress needle technique through the umbilicus. After insufflation of CO2 and maintaining the pressure at 13 mm Hg, a 2-cm periumbilical incision was made, preserving the fascial layer for trocar access. Conventional trocars were used, including two 5-mm standard trocars and a 10-mm standard trocar. The three ports were placed within the umbilical incision in an inverted equilateral triangular configuration, 1 cm apart, with the camera placed at the apex (Fig. 1). A 30° 10-mm rigid laparoscope (Stryker Endoscopy, Kalamazoo, MI) was used throughout the procedures. A grasper was inserted through the right 5-mm trocar, and a Harmonic® (Ethicon) scalpel was inserted through the left 5-mm trocar for dissection.

Placement of the trocars.
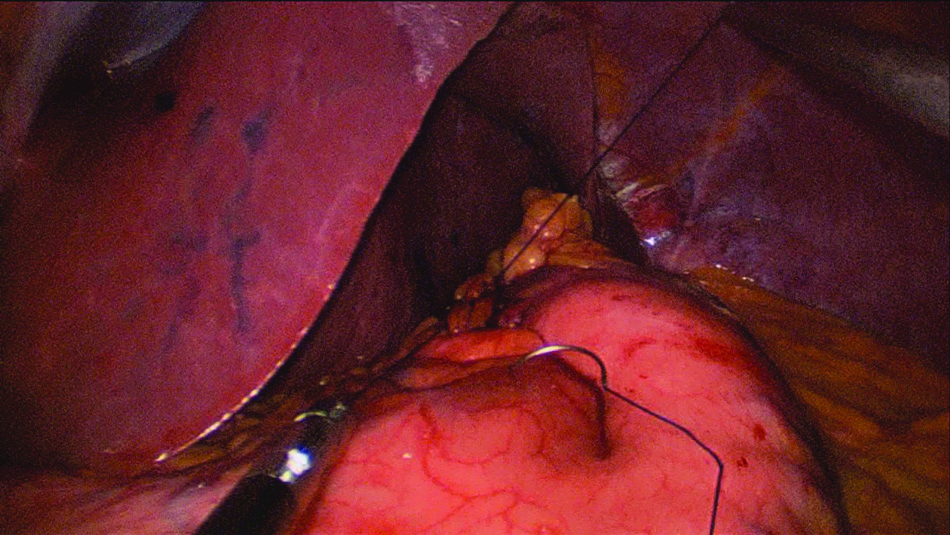
For liver retraction, we offered a new technique using cyanoacrylate (CA) glue. First, the glue was infused into a bottle connected to a sprayer and catheter. Second, the left triangular ligament of the liver was separated using a Harmonic scalpel, and a ¼ piece of gauze (6 cm×6 cm) was introduced into the abdomen through the 10-mm trocar to dry off the the diaphragmatic surface of the lateral left lobe of the liver and the diaphragm. Finally, the catheter was introduced into the abdominal cavity through the left 5-mm trocar for spraying. A 5-mm grasper in the left hand was introduced into the abdominal cavity through the right 5-mm trocar to elevate the left lateral lobe to bind it to the diaphragm (Fig. 2), providing a good operative field at the cardia (Fig. 3).
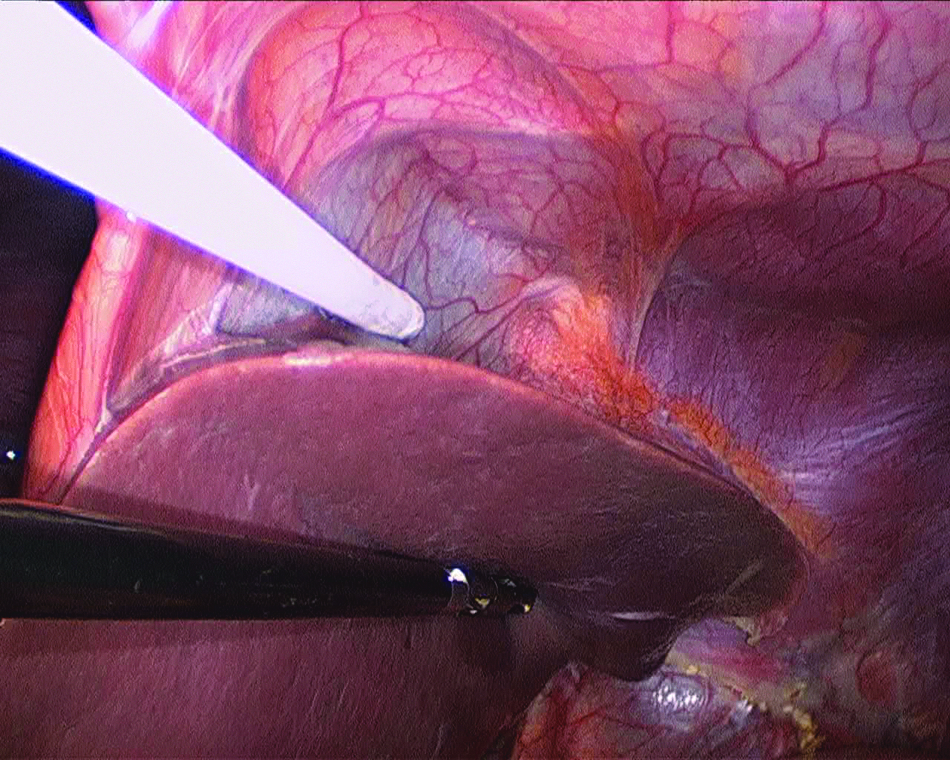
The cyanoacrylate glue was sprayed onto the diaphragmatic surface of the liver to bind the left lobe to the diaphragm.
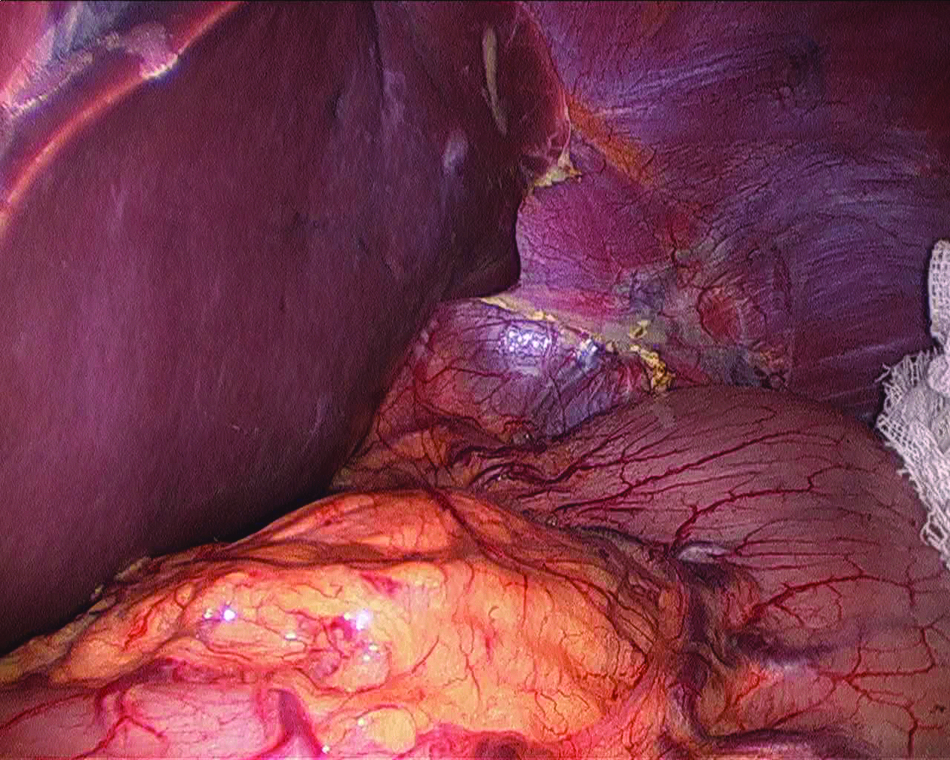
A good operative field at the cardia was created.
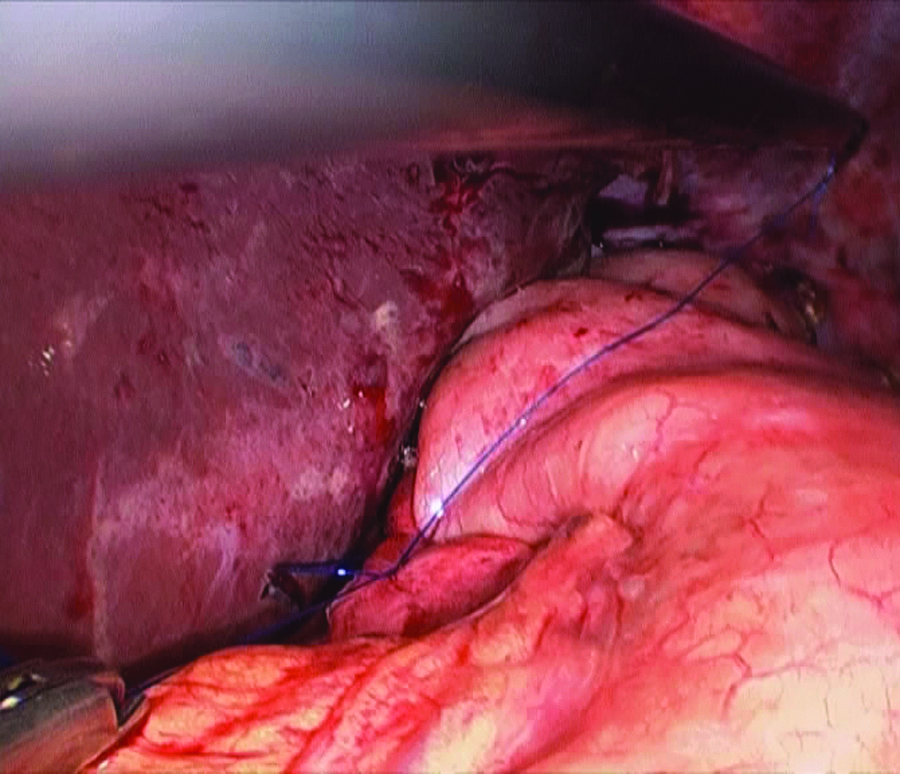
For achalasia, the esophageal–gastric junction was identified by intraoperative gastroscopy. The myotomy was to be 7 cm long, extending 2 cm to the gastric wall, using the Harmonic scalpel (Fig. 4). An intraoperative gastroscope was used to assess the adequacy of the myotomy and to detect any esophageal mucosal tears. The splenogastric ligament was divided to relieve tension from the wrap, and an anterior Dor fundoplication was created, the same as with the conventional laparoscopic multiple-incision procedure (Fig. 5). For hiatus hernia, after retraction of the liver as described above, the rest of the procedure was identical to the conventional laparoscopic Nissen fundoplication. The right crura was retracted laterally with a roticulated grasper, and the peritoneum was incised with the Harmonic scalpel. The hernia sac was dissected and totally mobilized in a standard fashion from right to left. Then, the gastrosplenic ligament was divided. After completion of dissection and removal of the whole hernia sac, a gauze strip was introduced into the abdomen and placed behind the esophagus to encircle the esophagus, thus exposing the posterior crus of the diaphragm. In all the cases, the hernia ring was less than 4 cm; therefore no mesh was used. Prolene suture with or without a needle was used to close the hiatus to 0.5–1.0 cm. The fundus was then brought behind the esophagus, creating a 360° wrap. The Nissen fundoplication was created the same as with the conventional laparoscopic multiple-incision procedure (Fig. 6). The sutures were tied using the intracorporeal technique. The length of the wrap was approximately 3–4 cm.
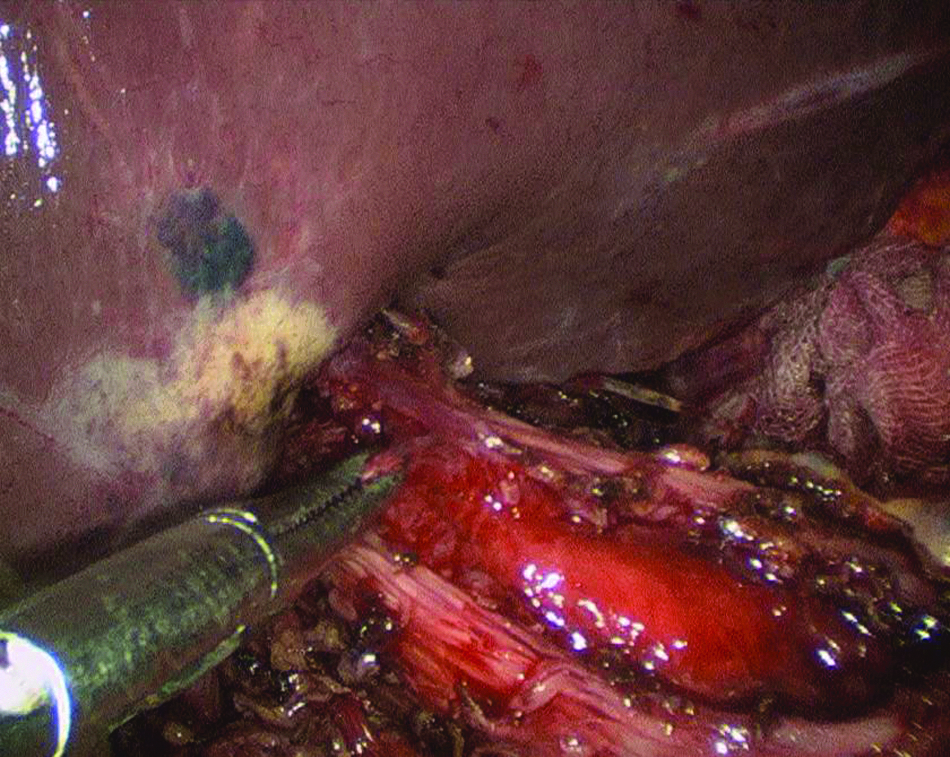
Hellor myotomy was performed, and the mucosa of the esophagus bulged out.
Completion of Dor fundoplication.
Completion of Nissen fundoplication.
At the end of the operations, the left lateral lobe of the liver was not deliberately freed to regain its original position.
Results
In total, seven TSILF procedures were performed. The type of hiatus hernia was confirmed during the operation as type I (Patient 2), type II (Patients 5 and 6), and type III (Patient 7). The operative characteristics for each patient is shown in Table 2. All the operations were successful without requiring conversion to a conventional multiport fundoplication or open surgery. The pneumoperitoneal time was 115–170 minutes, and blood loss was 15–50 mL. There were no intra- or postoperative complications. Postoperative pain was assessed by a visual analog scale. 7 The postoperative pain scores of the patients are shown in Table 3. The hospital stay was under 6 days for all patients. In all cases, the preoperatively observed symptoms immediately disappeared after the operation. There were no surgical site infections, umbilical hernia, postoperative intestinal obstructions, or recurrence of the symptoms at 5–23 months after the operation. The wound recovered very well without obvious scar on the abdominal wall (Fig. 7).

Umbilical incision 2 months after the operation.
Conventional endoscopic procedure: a retrospective analysis of the postoperative pain scores of the last 4 non-complicated cases undergoing conventional three-incision endoscopic fundoplication dated before November 1, 2009.
Discussion
Laparoscopic Heller myotomy has proved to be superior to endoscopic techniques in improving symptoms and duration of effect for achalasia. 8 The addition of an anterior fundoplication decreases symptoms of acid reflux without exacerbating or promoting dysphagia.9,10 It has also been proved that laparoscopic hiatus hernioplasty and Nissen fundoplication are superior to open surgery in medical cost and postoperative complications with a similar antireflux effect.11,12
With the technological advances, the advantages of laparoscopic operations have led to an increasing interest in the development of less-invasive procedures, and SILS has been ready for widespread implementation. Its merits have been witnessed, including minimal injury and cosmetic value. But, only a few sporadic reports about TSILF have appeared worldwide,6–12 with none so far reported in China. A key problem is how to establish an exposure technique without additional puncture of the abdominal wall or incision.
For the time being, we have developed a simple solution to this problem using CA glue. CAs are tissue glues with a chemical structure composed by monomers that polymerize rapidly when hydrogen ions are present, creating an acrylic resin, which solidifies in less than 1 minute. The mechanism of polymerization by contact with blood or water creates a tight closure if CA is applied on tissue. CA exists in two forms: short-chain CA (methyl-2 or ethyl-2), which is rarely used, because the compounds degrade quickly into cyanoacrylate and formaldehyde, which is very toxic for tissues; and long-chain CA (n-butyl-2-CA and n-octyl-2-CA), which degrades slowly so that buildup of toxic products is minimal, resulting in these compounds being safe for topical skin closure. 13 CAs have become widely used globally since the 2004 Cochrane Database report, 14 which stated that surgeons should consider tissue glue as an alternative to traditional suturing material as it is as effective for infection or leakage. Many studies have confirmed its effectiveness and safety in repair of surgical incision, wound closure in circumcision, repair of urethrocutaneous fistula, occlusion of post-paracentesis ascitic leak, embolization for hemangiomas, mesh fixation in hernia repair, etc.15–19
During our clinical practice, we usually use CA in splicing of the operative incision or hemostasis for diffuse staxis of the raw surface during laparoscopic surgery. After offering TSILF for our patients in 2010, we began to use CA for liver retraction. We believe that the glue, when used as described, offers a safe and simple solution to the problem of liver retraction in SILS fundoplication, thus obviating the need for standard trocar placement. The procedure is very rapid (less than 1 minute). In all of the cases, the left liver lobe can be retracted easily. But, the largest body mass index in this small series was just 24.4 kg/m2; whether this method would work on large livers remains to be validated. In any case, the surgeon has to be ready to use standard methods of liver retraction if necessary (5-mm trocar to lift the liver). In the future, magnetic retraction systems may prove helpful for TSILF as well. 20
Significantly improved cosmesis is an obvious advantage of the procedure. Indeed, when performed through the umbilicus, the procedure is virtually scarless (the umbilicus is a natural scar of the abdomen surface). However, in contrast to our expectation, a SILS approach to the fundoplication showed a trend toward a more severe, not less, incisional pain (Table 3); this might be explained by the close placement of trocars in a confined space and stress exerted on the tissue by surgical instruments and laparoscope during the procedure.
In conclusion, it is our opinion that TSILF is feasible for experienced laparoscopic surgeons with excellent cosmetic effect. The CA glue, when used as described, offers a safe and simple solution to the problem of liver retraction. However, TSILF requires a considerably high level of skills to perform and should only be attempted by highly skilled persons. It should be kept in mind that improved cosmesis must be carefully weighed against the potentially increased difficulties and risks of the procedure. Its merits and shortcomings compared with conventional laparoscopic fundoplication are yet to be demonstrated in a prospective clinical study.
Footnotes
Disclosure Statement
No competing financial interests exist.