
Abstract
Abstract
Transanal endoscopic microsurgery has been used by surgeons since 1983. All these years of experience and research have shown that this is a safe and successful approach for rectal neoplasms, both benign and malignant. The advantage of this procedure is the excellent view and hence precise surgical margins in an operative field that is otherwise difficult to reach. Furthermore, selected patients who used to require major rectal surgery now may be treated using this minimally invasive technique. These advantages may also be favorable for the gynecological field, especially in intravaginal surgery. Our case report describes the first successfully performed transvaginal endoscopic microsurgery in a woman with residual disease after treatment with chemoradiation for squamous cell carcinoma of the vagina. Despite the difficulty of operating in tissue with post-radiation effect, the rest of the tumor was excised with clear surgical margins without damage to the rectum. The patient was discharged from the hospital 2 days after the procedure and recovered without complications.
Case Report
Gynecological examination showed a large 6-cm tumor of firm consistency on the posterior vaginal wall. A biopsy specimen was taken and showed a carcinoma in situ with strong suspicion of invasion.
Additional investigation by computerized tomography demonstrated thickening of the vaginal wall suspicious for malignancy and an enlarged lymphoma on the right iliacal vessel. Examination with the patient under anesthesia confirmed the findings of a 6-cm tumor located just distal of the hymen, whereas the fornices seemed not to be involved. There were no signs that the rectal mucosa was affected. Larger biopsy specimens were taken, showing a well-differentiated squamous cell carcinoma of the vagina.
Imaging with computerized tomography–positron emission tomography and magnetic resonance imaging showed a tumor of 5 cm on the posterior vaginal wall with signs of extension to the rectum and pelvic wall (Fig. 1). On the right iliacal vessel a suspicious lymphoma of 7 mm was detected as previously seen on the computerized tomography scan. There were no other signs of lymph node involvement or distance metastasis.

Magnetic resonance imaging before treatment.
The patient was staged as a squamous cell carcinoma of the vagina FIGO stage III due to extension to rectal and pelvic wall (cT3N1M0), and she was treated with chemoradiation.
External irradiation included the complete vagina, pelvic, and groin nodes with a dose of 45 Gy in 25 fractions administered by seven modulated photon beams. External radiation was combined with weekly cisplatin (40 mg/kg) for 5 weeks. Finally, she received brachytherapy with seven fractions of 3 Gy three times a week
Response was evaluated by magnetic resonance imaging after 2 months and demonstrated an obvious reduction of the tumor on the posterior vaginal wall (Fig. 2). The lymphadenopathy on the right iliacal vessel had disappeared. The rectum seemed not to be involved. Examination with the patient under anesthesia showed incomplete vaginal remission confirmed by histology. A partial vaginectomy was planned. Because the lesion was located on the posterior wall only a few centimeters from the vaginal vault, intravaginal surgery would be difficult (Fig. 3). Furthermore, the tumor was in close contact with the rectal wall.

Magnetic resonance imaging after chemoradiation.

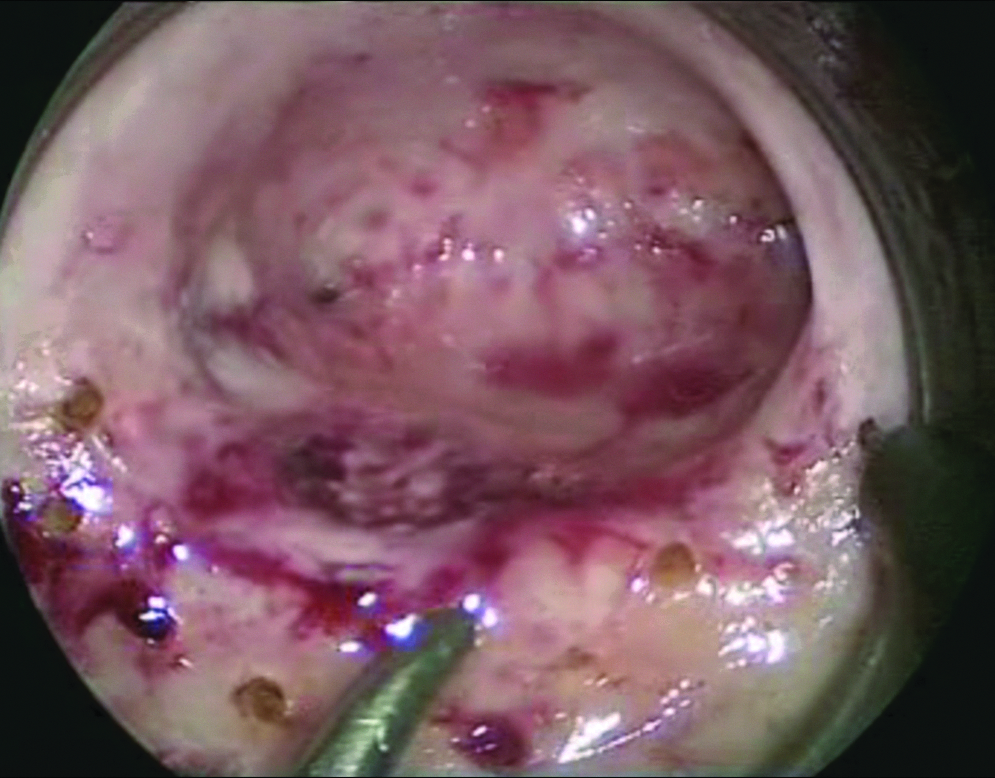
Preoperative situation. On the posterior vaginal wall the lesion is visualized after the rectoscope has been brought into position in the vagina. Distension of the vaginal wall is maintained by constant infusion of carbon dioxide.
Because of risk for rectal damage it was arranged that a surgeon be present. This surgeon was familiar with transanal endoscopic microsurgery, and during the preoperative evaluation the suggestion was made to excise the lesion using this technique. This approach has two great advantages that are significant in vaginal surgery: better access and superior view, both important to get clear surgical margins. Therefore transanal endoscopic microsurgery was used to excise the 1.5-cm lesion with a Harmonic® scalpel (Ethicon Endo-Surgery, a Johnson & Johnson Company, Blue Ash, OH) (Figs. 4–10).

Transanal endoscopic microsurgery instrumentation: video surgical rectoscope for transanal endoscopic operations (TEO®) from Karl Storz (Tuttlingen, Germany).

Transanal endoscopic microsurgery instrumentation: rectoscope with its introducer and the airtight faceplate.

Positioning of the rectoscope in transvaginal endoscopic microsurgery.
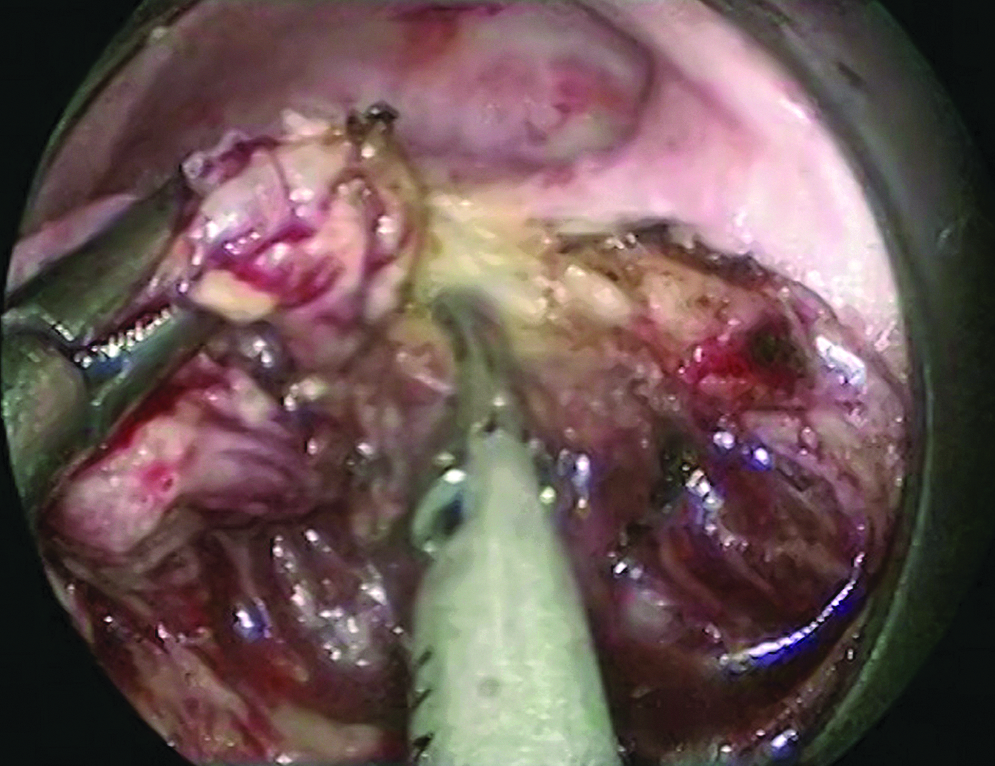
The lesion is marked off by electrocautery.
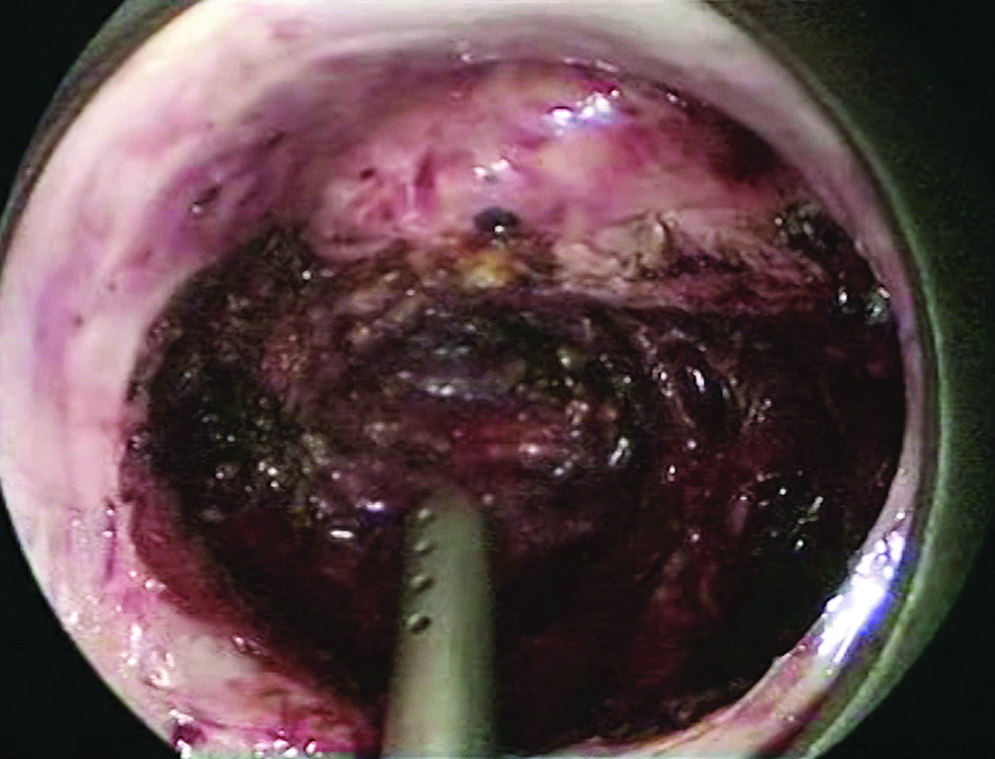
The lesion is excised.
The lesion is totally excised without damage to the rectum.
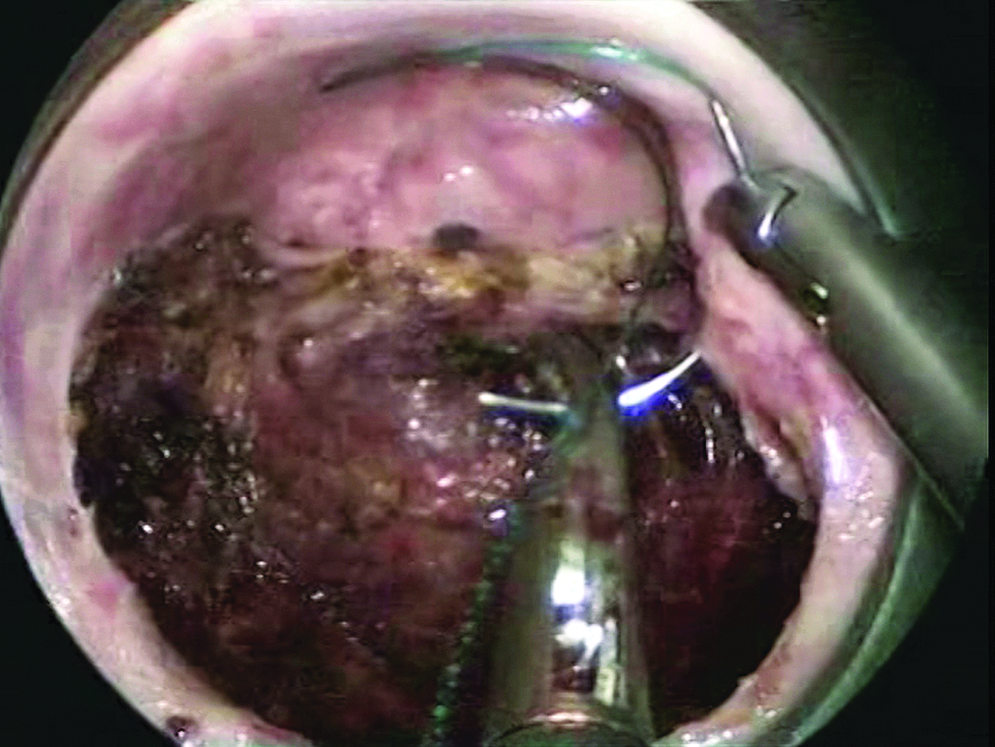
The defect is closed with POLYSORB 1 because V-Loc, which is normally used, is not suitable.
The rectal wall was clearly visualized during the procedure. The vaginal tumor did not invade into the rectal wall and could be excised with sufficient margin to leave the rectal wall intact. After removal of the tumor, fluid was brought into the vagina, and the rectum was filled with air. No air leak was seen, which confirmed that the rectum was intact. The pathology report showed complete excision of the tumor. The patient was discharged from the hospital after 2 days and recovered with no signs of complications.
Discussion
Vaginal cancer is rare and constitutes about 2% of gynecological malignancy. There is no consensus as to the proper management. 1 Surgery has a limited role in the management of patients with vaginal cancer. 2 This is mainly due to the impaired clarity in visualization and accessibility of the vagina to obtain clear surgical margins, often leading to absence of radicality. Nevertheless, in selected cases satisfactory results can be achieved. Radiotherapy with or without chemotherapy with curative intent is, in the majority of cases, the treatment method of first choice. 3
The view and exposure of the tumor during intravaginal surgery are often hampered by difficult exposure due to the narrow and small region and the use of specula. Additionally, surgery is hampered by the fact that most women are postmenopausal and have undergone radiation therapy. Post-radiation lesions in the proximal part of the vagina are frequently seen and can be a difficult surgical hurdle.
Transanal endoscopic microsurgery is a minimally invasive procedure used by gastrointestinal surgeons for the management of benign and carefully selected malignant rectal tumors.4–6 This technique uses a 40-mm-diameter rectoscope, which is available in two different lengths. The rectoscope has an airtight faceplate through which instruments can be brought in (Figs. 4–6). Carbon dioxide is constantly infused to maintain distension of the rectal cavity, and gas loss is prevented by the airtight faceplate. Because of stereoscopic magnification the visualization is improved, and therefore the surgical margins can be more precise even when the lesion is located more proximally. After correct positioning of the rectoscope with a double-ball jointed Martin arm, fixed to the operating table, the procedure can be started. The surgical margin around the lesion is marked out by electrocautery. Subsequently, a full-thickness excision of the lesion is performed with electrocautery and/or the Harmonic scalpel in our clinic. The defect is sutured using resorbable sutures such as V-Loc™ 2.0 (Covidien, Norwalk, CT) or POLYSORB™ 2.0 (Covidien). One of the advantages of using endoscopy in vaginal surgery is a clear view and the magnification. This allows better visualization of anatomical structures such as the rectal wall. Other advantages are the better access and more space in which to operate. All these advantages are significant in vaginal surgery and are helpful to obtain clear surgical margins. Buess et al. 6 already described this method in the 1980s and concluded that compared with traditional transanal excision, transanal endoscopic microsurgery is more accurate because of the use of microsurgical preparation and an easier access to higher located lesions. There were no complications in the patients they described. The considerable technical complexity of the endoscopic procedure was seen as a possible disadvantage. 6
Subsequent studies that followed over the years showed that transanal endoscopic microsurgery has several advantages compared with traditional surgery and that it is a safe and successful approach with a low recurrence rate.7,8 In our opinion, these advantages also are valid for vaginal surgery, which prompted us to utilize this technique in our patient.
When transanal endoscopic microsurgery is used in rectal surgery, the rectal sphincter helps to create a pneumorectum, together with the diameter of the rectal port used. In our patient there were no problems in creating and maintaining a pneumovagina. However, one can imagine that a wide introitus could give problems in creating a pneumovagina. Because there are different sizes of tubes, we feel that this limitation is of minor importance, and therefore new larger models can be developed.
Careful preoperative evaluation and patient selection remain important because transvaginal endoscopic microsurgery will initially only be suitable for a small group of patients with circumscript smaller lesions of vaginal cancer. The technique can be done by experienced endoscopically trained gynecological oncologists or gastrointestinal surgeon operators. The learning curve of the transanal endoscopic microsurgery technique is relatively short, depending on the surgeon's experience, and it can be learned with proper training and tutoring.
Extensive research of PubMed was performed for relevant literature concerning the use of transvaginal endoscopic microsurgery for gynecological indications without success (search terms used were “transanal endoscopic microsurgery,” “TEM,” “TEMS,” “transvaginal endoscopic microsurgery,” “TVEM” AND “vaginal carcinoma,” “vaginal cancer,” “vaginectomy”). To our knowledge, this is the first report of using the minimally invasive endoscopy in vaginal surgery.
In conclusion, we show that the transanal endoscopic microsurgery technique in vaginal surgery offers advantages and is safe to perform. We believe that there are more indications in the gynecology field where this advantageous technique could be used. Finally, this case demonstrates the extra value of good understanding and cooperation between different surgical disciplines in a period of quickly developing surgical innovating techniques.
Footnotes
Disclosure Statement
No competing financial interests exist.