
Abstract
Abstract
Purpose:
Laparotomy is the preferred option for the surgical treatment of necrotizing enterocolitis (NEC); however, laparoscopy may offer benefit, particularly when it is uncertain if the operation is necessary. Our aim was to review the current evidence for the use of diagnostic and therapeutic laparoscopy in NEC.
Materials and Methods:
A systematic review of published literature (1990–July 2012) found in MEDLINE, EMBASE, the Cochrane Library Controlled Trials Register, and the Cumulative Index to Nursing and Allied Health reporting the use of laparoscopy for management of acute NEC was undertaken.
Results:
Seven studies (six case series and one case report) reporting the use of laparoscopy in 44 infants (weighing 0.5–2.9 kg) with NEC were identified and included for review. There were no randomized controlled trials. Laparoscopic techniques differed among the studies, with standard laparoscopy (gas) used in 28 (64%) cases, fluorescein-aided assessment in 8 cases (18%), and gasless laparoscopy in 8 cases. Eight (18%) infants did not require further surgery following laparoscopy: 4 (9%) had no evidence of NEC, 2 (5%) had no evidence of perforation and/or intestinal gangrene, and 2 (5%) had NEC totalis precluding further surgery. In the remaining 36 (86%) infants in whom further procedures were required following laparoscopy, 9 had placement of a peritoneal drain, 20 had a stoma, and 7 had intestinal anastomosis. Perforation was detected in 25 (57%) infants; however, among the 19 infants who had no detectable perforation at initial laparoscopy, 1 infant (5%) subsequently required laparotomy for a missed perforation. Six (14%) infants died: 2 had care withdrawn due to pan-intestinal NEC, 2 died of ongoing NEC, and 2 of recurrent NEC following recovery from the acute episode.
Conclusions:
Laparoscopy is a useful tool in the armamentarium of surgical management of NEC, with one-fifth of patients not requiring further surgery. Laparoscopy can be useful in selected babies with suspected NEC to avoid unnecessary laparotomy and minimize the trauma of surgery.
Introduction
In those cases of NEC requiring surgery, laparotomy is the preferred surgical option; however, laparoscopy may offer benefit, particularly when signs of bowel perforation are absent.4,7–12 In such cases, laparoscopy may aid visualization of the bowel and determine its perfusion status, as first reported by Pierro et al. 11 Diagnostic laparoscopy allows the detection of cases that would not require any further intervention, thus avoiding further insult and stress, which can only be of benefit in an already compromised, premature baby. Our aim was to review the current evidence for the use of laparoscopy in NEC.
Materials and Methods
Search strategy
We undertook a standard search of all published literature of MEDLINE, EMBASE, the Cochrane Library Controlled Trials Register (CENTRAL), and the Cumulative Index to Nursing and Allied Health (CINAHL) up to July 2012. No lower date limit was used, in order to include all relevant reports. Our search was limited to children, using “necrotizing enterocolitis” and “laparoscopy” and their MeSH terms. We included all studies, in English language, reporting the use of laparoscopy for NEC. All abstracts were screened, and the bibliographies were further examined to identify any additional reports/studies that were eligible for inclusion in this review (see Figure 1 for a full study selection flow chart).
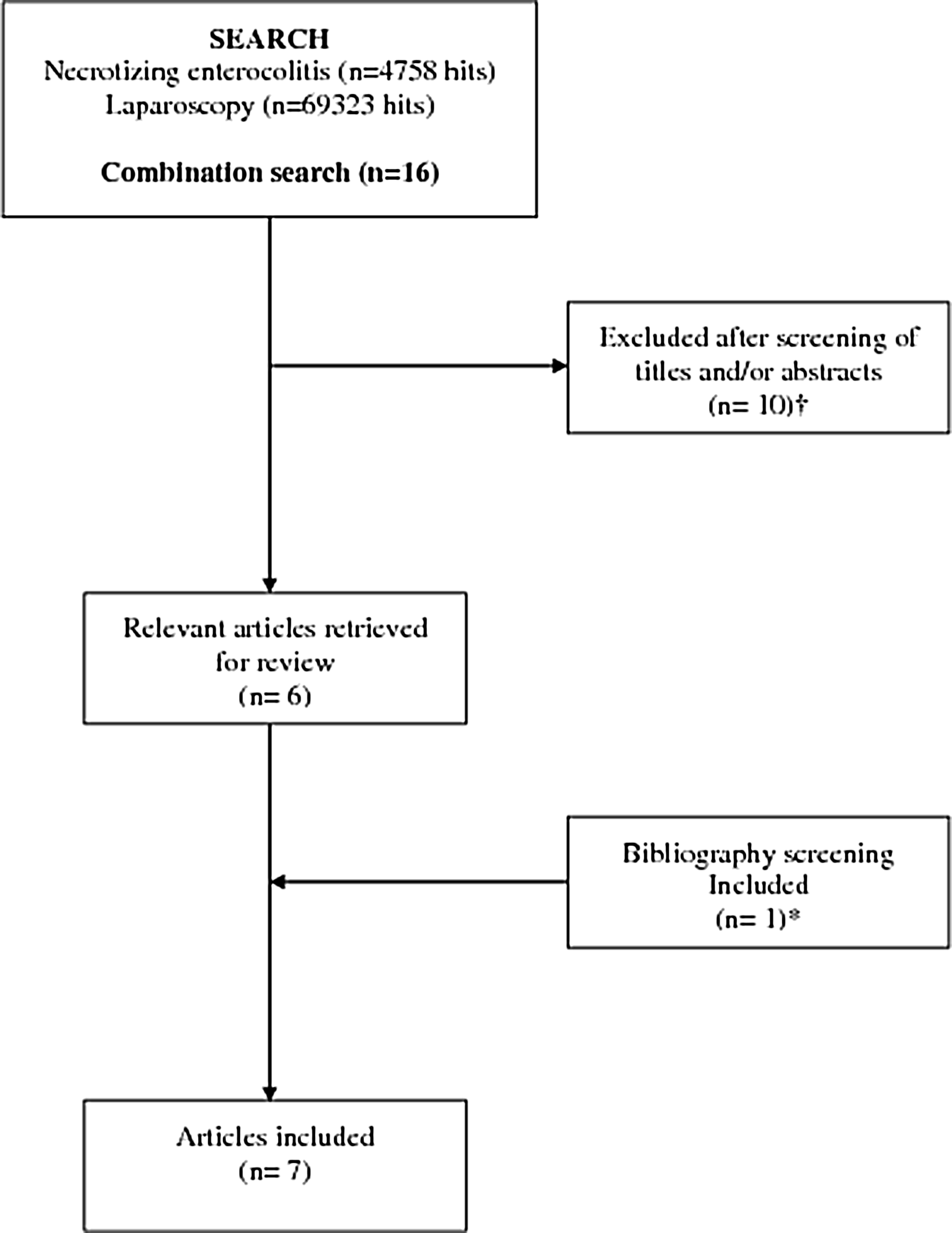
Flow chart for article selection. †Studies not reporting use of laparoscopy. *Book chapter published a personal communication on laparoscopy for necrotizing enterocolitis.
Study selection criteria
Two reviewers (both of the authors) independently assessed all the selected studies. We included all reports of laparoscopy for management of NEC due to the paucity of evidence in form of randomized controlled trials.
Data extraction and analysis
Data were independently extracted by two reviewers (both of the authors) and tabulated on a predefined data extraction form. The following data were extracted: first author, year of study, study duration, methodology, characteristics of study participants, characteristics of laparoscopic procedure, and outcomes following laparoscopy. Any discrepancies were resolved by discussion and consensus. Outcomes were compared using Fisher's exact test, and the significance level was set at 5%.
Results
Characteristics of studies
There were no randomized controlled trials reported. Our combined search retrieved 16 studies; 7 of these (6 studies and 1 book report) were identified and included as relevant to the review (Table 1). All of these reports were case series, with the largest being by Numanoglu and Millar. 10 Of the 10 studies that were excluded from this review, 3 were review articles,3,13,14 2 reported on management of NEC-related strictures,15,16 1 article was in Spanish, 17 and 4 were unrelated.18–21
Personal communication in a book chapter.
Characteristics of patients
Apart from one case report, the number of cases ranged from 3 to 13, giving a total of 44 patients in the final analysis. The weights of the infants at the time of laparoscopy ranged from 0.5 to 2.9 kg.
Laparoscopic technique
There was a variety among the studies in terms of the laparoscopy techniques (Table 1). The port size ranged from 2.5 to 4.7 mm: a standard 3- or 4-mm port was used in five reports (n=37), whereas two reports used 1.9-mm (n=4) and 2.5-mm (n=3) ports. The camera size ranged from 1.9 to 4 mm (0° or 30° lens). Insufflation pressures used ranged from 6 to 15 mm Hg in four studies, and one study used gasless laparoscopy. Standard laparoscopy (gas) was used in 28 (64%) infants, fluorescein-aided laparoscopy for assessment of bowel perfusion in 8 (18%) cases, and gasless laparoscopy in a further 8 (18%) cases.
Outcomes (Table 2 and Fig. 2)
Of the 44 patients who had laparoscopy for management of NEC, 40 (91%) had the diagnosis of NEC confirmed at laparoscopy, and NEC was excluded in 4 (9%) patients (Fig. 2). In those with confirmed NEC at laparoscopy, 29 (72%) had evidence of perforation and/or gangrene, whereas 11 (28%) had neither perforation nor gangrene. In total, 8 (18%) patients did not require further surgery after laparoscopy: 4 (9%) had no evidence of NEC, 2 (5%) had no evidence of perforation and/or intestinal gangrene, and 2 (5%) had NEC totalis precluding further surgery. Overall, 25 (57%) patients had bowel perforation detectable at laparoscopy.
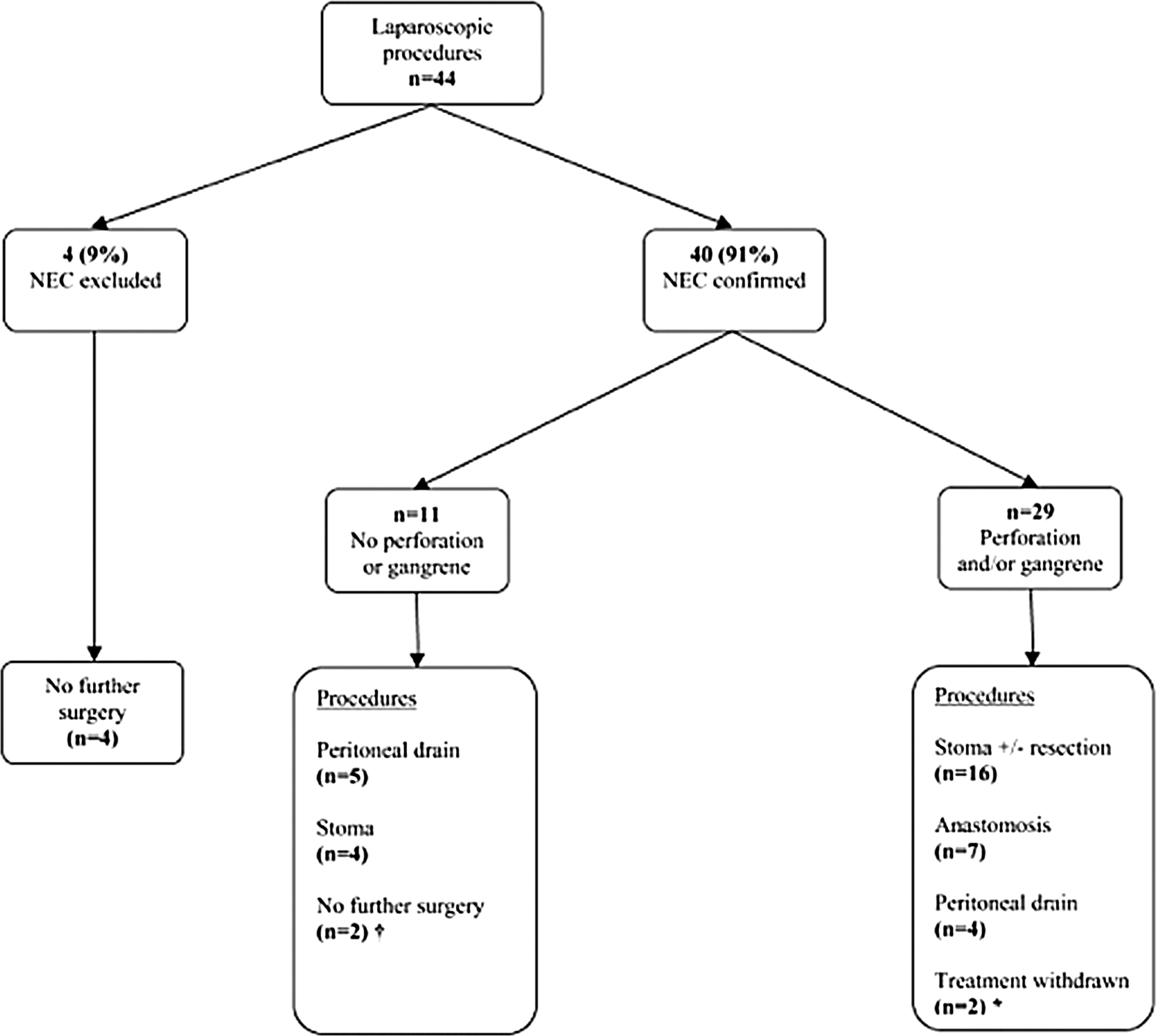
Flow chart showing outcomes of diagnostic laparoscopy. †One infant had missed perforation requiring subsequent laparotomy. *Two infants had necrotizing enterocolitis (NEC) totalis precluding bowel resection.
Personal communication in a book chapter.
Case report.
Mortality
Six (14%) infants died: in 2 infants the deaths occurred later, following complete recovery from the acute NEC episode, whereas in the remaining 4 infants, care was withdrawn in 2 infants who had pan-intestinal disease confirmed at laparoscopy, and the other 2 infants succumbed to ongoing NEC.
Complications
There was only one study that reported 1 case of missed perforation at laparoscopy: the perforation later identified at a subsequent laparotomy for clinical deterioration. This infant had gross intestinal distension that precluded adequate visualization of the entire intestine.
Discussion
Surgical management of infants with NEC in the absence of cardinal signs of perforation poses a great challenge and a clinical dilemma to pediatric surgeons. 3 This dilemma is often exacerbated when all attempts at maximizing medical therapy have been exhausted and yet the infant remains unstable. Laparoscopy may play a role in assisting in the diagnosis of NEC and detection of supervening complications of perforation and/or intestinal gangrene, by providing an opportunity to visualize the tissue and assess its viability. 11 The information gained by direct visualization of the bowel may greatly assist the surgeon in selecting cases that would further benefit from a definite laparotomy. Conversely, of even greater importance is the detection of cases that would not require any further intervention, thus avoiding further insult and stress, which can only be of benefit in an already compromised, premature baby.
There are no randomized controlled studies in the literature to date reporting the use of laparoscopy for management of NEC. The current evidence is based on case series reports. The first published report on the diagnostic use of laparoscopy for infants with NEC was by Pierro et al., 11 although previous to this, Albanese and Rowe 22 in a book chapter described Dr. R.W. Jennings's personal communication of his experience of 3 cases that underwent diagnostic laparoscopy.
In situations where radiological evidence of NEC is lacking, diagnostic laparoscopy offers the clinician the benefit of assessing the intra-abdominal compartment for the presence and extent of disease and of detecting bowel perforation that would otherwise have been missed. This would prevent significant delays in the diagnosis of perforated cases of NEC, avoiding unnecessary morbidity. In our review, laparoscopy was useful in identifying cases in which there was no evidence of NEC (n=4; 9%). This group of patients was able to be excluded from continued medical therapy of NEC. Similarly, in the ones where NEC was confirmed at laparoscopy (n=40; 91%), laparoscopy was able to select 9 (23%) cases in which there were no indications for laparotomy as there was no perforation and/or gangrene. However, this has to be weighed against the single patient in whom initial laparoscopy did not detect perforation but who had evidence of perforation at a subsequent laparotomy for continued clinical detection. It is difficult to know if the perforation was present and therefore missed or if it occurred later on.
Recently, other authors have reported their experience with gas insufflation, gasless laparoscopy, and fluorescein-aided laparoscopy in these infants lacking specific indications for laparotomy.7–10,12 Numanoglu and Millar 10 proposed the use of fluorescein assessment as an adjunct to standard laparoscopy, especially in detecting ischemic changes. Infants diagnosed with NEC may have gross abdominal distension, and therefore the added pneumoperitoneum from laparoscopy may have detrimental effects. In such situations, gasless laparoscopy, as reported by Leva et al., 8 may be beneficial in avoiding the increase in abdominal compartment pressure in these “sick” infants. Gross abdominal distension is a contraindication to laparoscopy for technical and safety reasons. One study 11 reported the use of insufflation pressures of up to 15 mm Hg, but we strongly advocate insufflation pressures not to exceed 5–8 mm Hg. Similarly, gasless laparoscopy may not be feasible if gross abdominal distension is present. 8
Nah et al. 9 reported an extended use of laparoscopy by using it as a therapeutic tool, especially in those with identifiable focal disease. In their report, a select patient group having focal intestinal perforation were managed by laparoscopy, with localization and exteriorization of the perforation through a 1-cm microlaparotomy in three extremely low-birth-weight infants among their four infants. The advantage of a limited, localized incision centered on the area of bowel involvement cannot be overemphasized.
Laparoscopy offers unique benefits in the clinical setting of premature infants with NEC. Laparoscopy allows for direct assessment of bowel viability without the need to grossly handle friable bowel; it can safely be undertaken in the neonatal intensive care unit by the patient's bedside 11 and in some cases without gas insufflation to minimize further increases in abdominal pressure 8 and in the presence of an adjuvant such as fluorescein can assess bowel perfusion and viability. 10 When laparotomy is deemed necessary, the position and size of incision during conversion from laparoscopy can be selected and directed to the area of the site of perforation or disease for bowel exteriorization. 9
This systematic review suffers from the paucity of high-quality studies as most of the reports are single-center case series. However, the current evidence demonstrates that laparoscopy is beneficial in providing additional diagnostic information that would assist the surgeon in decision making in selected babies.
Conclusions
Current available evidence, although limited by the lack of randomized controlled trials, shows that laparoscopy is a useful tool in the armamentarium of surgical management of NEC, with one-fifth of patients not requiring further surgery. In selected babies with suspected NEC, laparoscopy may be beneficial in avoiding an unnecessary laparotomy and minimizing the trauma of surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.