
Abstract
Abstract
We report a case of a 7-year-old boy with a voluminous 8.5-cm “cobra-head” calculus in a duplex system ureterocele causing flank pain, hematuria, and infection. Combined cysto-ureteroscopy and percutaneous cystolithotomy enables dependent ureterocele incision along its inferolateral border and efficient stone clearance in a single minimally invasive procedure. Protracted and repeated urethral instrumentation is avoided.
Introduction
Case Report
A 7-year-old boy presented with left flank pain, hematuria, and recurrent urinary infections from infancy. Abdominal radiography and ultrasound imaging showed a left intravesical ureterocele packed with a voluminous 8.5-cm “cobra-head” calculus without proximal hydronephrosis (Fig. 1). Mercapto-acetyltriglycine renography attributed 39% differential function to his duplex kidney with apparent good drainage. A coliform urinary tract infection was treated preoperatively, and intravenous antibiotics were administered on induction of general anesthesia.
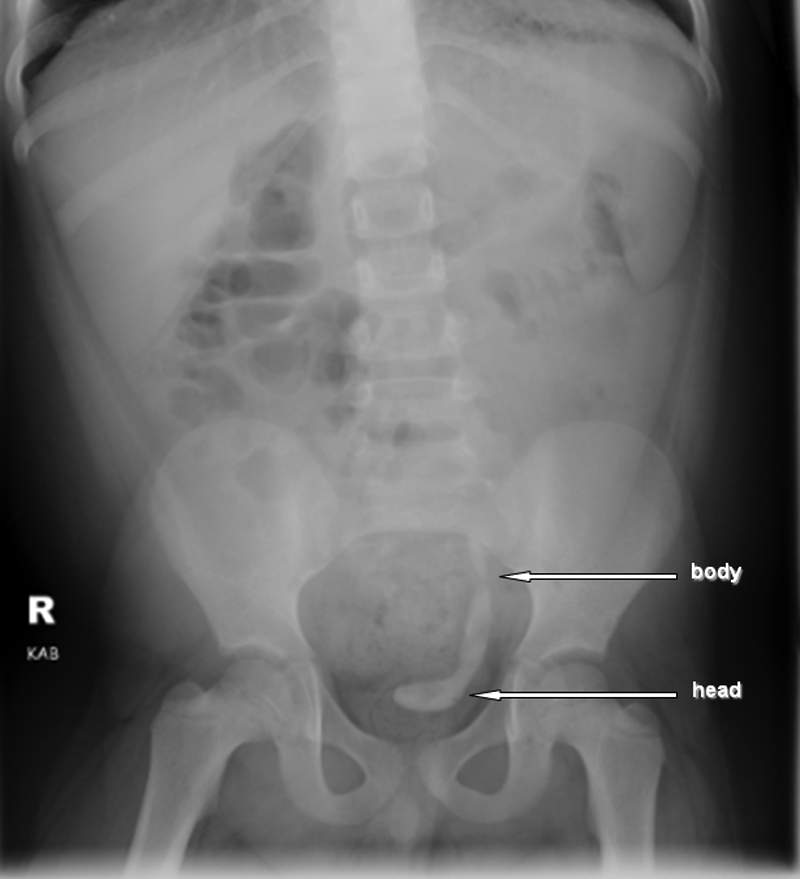
Plain abdominal radiograph demonstrating a “cobra-head” stone filling an intravesical ureterocele and ureter of the upper moiety of a left duplex kidney.
The patient was positioned supine in lithotomy. By cystoscopy, the upper moiety ureterocele was incised along its inferolateral border with a holmium–yttrium-aluminum-garnet (YAG) laser (Versapulse®; Lumenis®, Santa Clara, CA). A PCCL tract was established suprapubically: a Kellett needle allowed placement of a guidewire (0.035 sensor; Boston Scientific™, Marlborough, MA), over which the tract was dilated (7Fr rigid dilator [Cook Medical, Limerick, Ireland, United Kingdom] and NephroMax™ balloon [Boston Scientific]) to a clear Amplatz sheath (30Fr; Cook Urological). An unsheathed nephroscope (Karl Storz, Tuttlingen, Germany), passed through the PCCL tract into the ureterocele, allowed the “head” of the calculus to be cleared by ultrasonic lithotripsy (LithoVac [Swiss Lithoclast® Master; EMS, Nyon, Switzerland]) and a grasping forceps. In view of the 90° angulation from the stone's “head” to “body,” a semirigid ureteroscope (4.5/6.5Fr; Richard Wolf Medical Instruments, Vernon Hills, IL) was passed through the urethra. A second guidewire (0.035 sensor; Boston Scientific) was inserted under direct vision and image guidance retrograde into the renal pelvis. With the ureteroscope alongside the wire, complete stone fragmentation was achieved by a holmium-YAG laser. After transfer from the ureter to the bladder by a Dormia basket (1.9Fr zero-tip; Boston Scientific), the stone fragments were cleared by the LithoVac via PCCL. A JJ stent (4.7Fr 8–20 cm; Cook Medical) was inserted under X-ray guidance.
The suprapubic and urethral catheters were removed 3 and 5 days, respectively, postoperatively. Following an uneventful recovery, the child was discharged home on postoperative Day 3. On removal of the JJ stent and check ureteroscopy 4 weeks later, the upper-moiety ureter, ureterocele, and bladder were found to be stone free.
Results
At the 3-month follow-up, the patient was asymptomatic with a good urinary stream. Ultrasound imaging and dynamic renography showed collapse of the ureterocele, absence of hydronephrosis, no stone recurrence, and preserved function with good drainage. Stone analysis showed 100% carbapatite.
Discussion
To our knowledge this is the first case report of combined minimally invasive techniques for ureterocele incision and lithotomy in a child. Despite apparent good drainage on dynamic renography and absence of hydro-ureteronephrosis, our patient developed an extensive 8.5-cm “hockey-stick” stone in the upper-moiety ureter and ureterocele of a unilateral duplex kidney after years of recurrent urinary tract infections. As the stone was confined to the distal upper-moiety ureter, the ureterocele must have been obstructed. Transurethral cystoscopy enables a precise puncture of the ureterocele at its most dependent point. An incision along its inferolateral border maintains the roof of the ureterocele intact, resulting in a potential flap valve to reduce subsequent iatrogenic vesicoureteric reflux. 6 Ureteroscopic stone fragmentation by a holmium-YAG laser is a well-established treatment modality for ureteric stones in children. The rate of laser lithotripsy depends on stone size rather than composition. 7 As operative time has a direct effect on the incidence of septic shock and hemorrhage following stone surgery, 8 the efficiency of stone fragmentation and extraction is of great importance in the presence of an extensive stone burden. Stone fragmentation by the Swiss LithoClast is faster than by a holmium-YAG laser, 9 but stone fragments cannot be passed through the pediatric 4.5/6.5Fr ureteroscope. Deploying the Swiss LithoClast via a PCCL tract allows rapid stone fragmentation of the “cobra-head” as well as simultaneous transurethral ureteroscopic laser lithotripsy. For extraction, larger stone fragments can be cleared via a PCCL tract using grasping forceps or by continuous suction (LithoVac) rather than transurethrally. 10 Prolonged and repeated urethral instrumentation is avoided, reducing the risk of iatrogenic urethral stricturing.
Conclusions
This combined approach permits accurate ureterocele incision along its inferolateral border and access to both the stone's “head” and “body” in a single minimally invasive procedure, as well as highly efficient stone clearance.
Disclosure Statement
No competing financial interests exist.