
Abstract
Abstract
Background:
To determine whether performing transient occlusion of uterine arteries (TOUA) immediately before laparoscopic myomectomy can reduce intraoperative complications.
Subjects and Methods:
In a retrospective case–control study, laparoscopic myomectomy with and without TOUA was examined. Data were analyzed from 89 laparoscopic myomectomies performed by a single surgeon (Y.-S. Kwon) at Ulsan University Hospital (Ulsan, Korea) between March 2011 and December 2011. Surgical outcomes included preoperative myoma size, number of myoma, operative time, and operative blood loss.
Results:
Forty-nine women underwent laparoscopic myomectomy with TOUA with endoscopic vascular clipping, whereas 40 control patients underwent laparoscopic myomectomy alone. The TOUA group had no case of nerve or vascular injury during the operation time. The mean time of occlusion of both the uterine arteries was 15 minutes. The TOUA group had less mean blood loss during the operation than the group with laparoscopic myomectomy alone (111.9 versus 203.4 mL; P<.001). There were no significant differences in size and number of uterine myomas and intraoperative complications between the two groups. Moreover, there was not even a single case of conversion of laparoscopy to laparotomy in either group.
Conclusions:
TOUA performed immediately before laparoscopic myomectomy facilitated minimally invasive surgery with lower blood loss and no differences in other intraoperative complications.
Introduction
With the help of advanced laparoscopic surgeries in the gynecologic field, the surgical trend of myomectomy has been shifting from abdominal myomectomy to laparoscopic myomectomy. Since Semm and colleagues described the procedure in the late 1970s,5–8 there has been tremendous advancement in laparoscopic myomectomy technique with favorable surgical outcomes.
There are several comparative studies on surgical outcomes with abdominal procedures. The published reports demonstrate that laparoscopic myomectomy is clearly associated with a shorter period of hospitalization, faster recovery, less expense, less pain, less blood loss, less fever, and fewer surgical complications compared with abdominal myomectomy.9–11
In spite of the benefits of laparoscopic myomectomy, the technique is associated with several surgical limitations that might affect outcomes. These include the suturing method, enucleation of the myoma, and intraoperative bleeding, depending on the number and location of myomas.
Several current reports describe suturing methods with comparable surgical outcomes and enucleation methods, but there are fewer reports demonstrating reduction of intraoperative bleeding and securing a clean operative field. To demonstrate an advanced technique to reduce intraoperative bleeding, the present study introduces the technique of transient occlusion of uterine arteries (TOUA) during the operation with comparable surgical outcomes between the group of patients with occlusion of the uterine arteries and the non-occlusion group.
Subjects and Methods
Enrolled in the study were 89 patients who received laparoscopic myomectomy with or without TOUA from March 2011 to December 2011 at Ulsan University Hospital (Ulsan, Korea). The patients were selected consecutively. The inclusion criteria included the presence of a symptomatic myoma measuring 9 cm or less on ultrasonographic examination that was an intramural type of myoma. Those cases with submucosal and subserosal types were excluded from this study. Laparoscopic myomectomy with TOUA was preoperatively suggested to all patients who fulfilled the inclusion criteria, and the procedure was performed after obtaining consent from the patients. The operating time was defined as the period from skin incision to closure. The size of the myoma was the maximal diameter of the myoma on ultrasonography. The operative blood loss was estimated by subtracting the rinse volume from the blood volume that was collected in the suction apparatus. This study was approved by the Ulsan University Hospital Institutional Review Board.
Surgical technique
The patient was placed in a dorsal lithotomy position under general anesthesia with endotracheal intubation. A uterine manipulator (Hangzhou Shikonghou Medical Equipment Co. Ltd., Hangzhou, China) was placed in the uterine cavity to allow movement of the uterus. This manipulator facilitates moving the uterus into the optimal position during enucleation and suturing. The intra-abdominal pressure was maintained at 13 mm Hg with carbon dioxide gas. Once the pneumoperitoneum was achieved, video laparoscopy (laparoscopic camera from Karl Storz, Tuttlingen, Germany) was performed using a 10-mm trocar that had been introduced through the umbilicus. Three trocars were needed for the operation: a 12-mm trocar for placement of the endoscopic vascular clip on the left side, a 5-mm trocar on the right side of the lower abdomen, and another 5-mm trocar on the median line just above the pubic hairline. These ports were inserted for the introduction of the surgical instruments. Through the triangular area (round ligament, ovarian ligament, infundibulopelvic ligament, and psoas muscle), along the infundibulopelvic ligament, the peritoneum was incised using a monopolar electrode. Using a blunt-tip suction, the umbilical artery was first isolated, and the assistant moved the umbilical artery upward and in the lateral direction. Second, it was possible to isolate the branching uterine artery along the umbilical artery using blunt-tip suction. The isolated uterine artery was occluded by an endoscopic vascular clip (temporary atraumatic endo-vessel-clips; B. Braun Korea Co., Ltd., Seoul, Korea) (Fig. 1). Occlusion of the uterine artery on the other side was performed by using the same method with an endoscopic vascular clip.

Transient occlusion of uterine arteries with a endoscopic vascular clip.
About 3 minutes was allowed for the uterine blood to flow out just after completion of occlusion of both the transient uterine arteries. The myometrium covering the myoma was deeply incised by a monopolar cutting electrode until the underlying myoma was visually exposed. The enucleation of myoma was completed using endoscopic scissors and a dissector. 12
The defect area was sutured after excision of the myoma with the three layers, which included first a widely deep single interrupted suture, a continuously nonlocking running suture, and a continuously interlocking suture. The first assistant held the stitch to maintain the suture tension throughout the repair process (Fig. 2). Finally, both the endoscopic vascular clips were removed safely, and the excised tumor was removed using an electric morcellater (Gynecare Worldwide, a division of Ethicon Inc., Somerville, NJ). A drainage tube was inserted through the suprapubic incision.
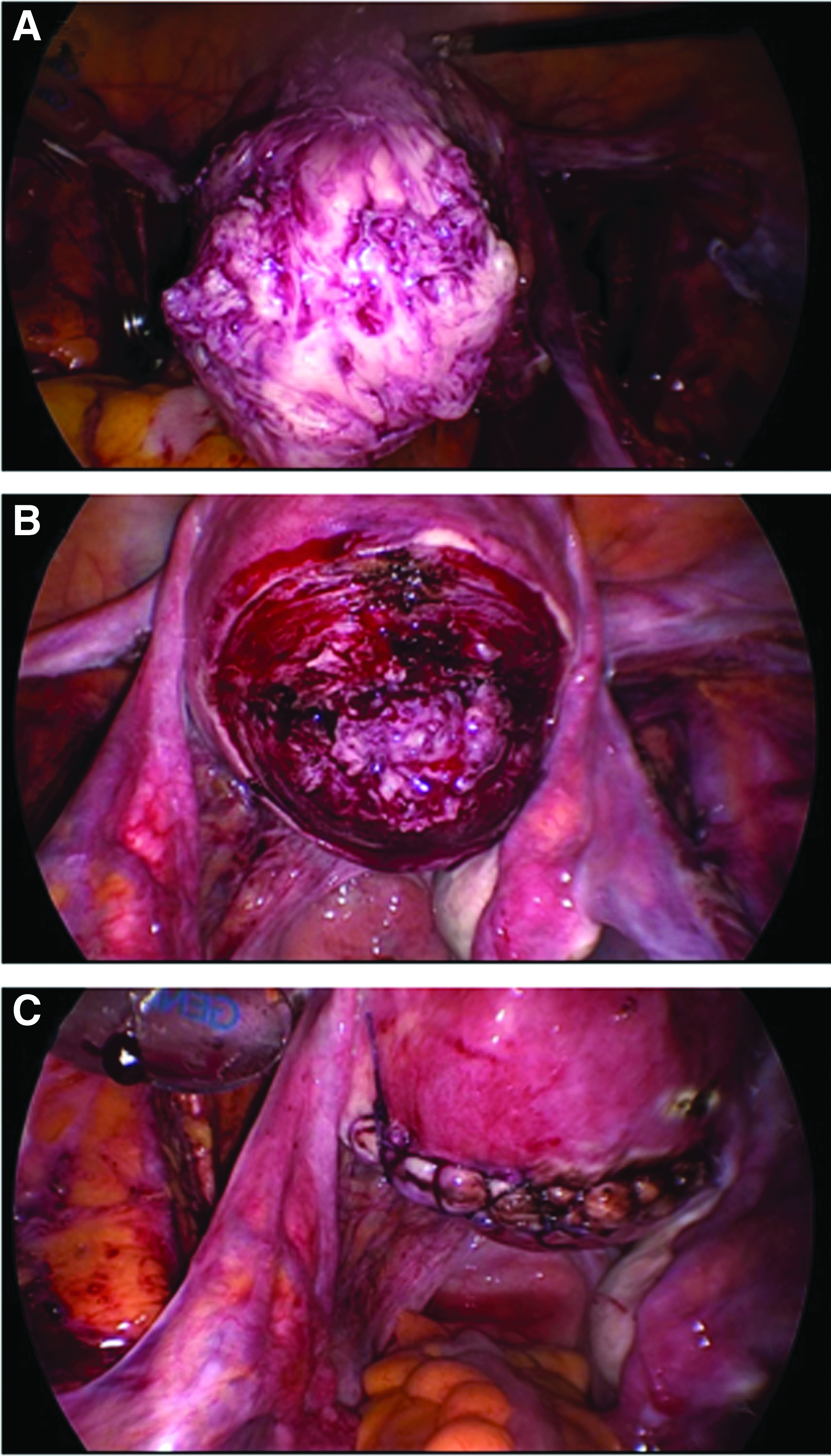
Laparoscopic myomectomy.
Statistics
Statistical Package for Social Science software (SPSS, Inc., an IBM Company, Chicago, IL) was used for the statistical analysis. Data are expressed as mean±SD values or absolute number (%). Categorical variables were analyzed by using the chi-squared test, and continuous variables were analyzed by using Student's t test. The differences were considered significant at a level of P<.05.
Results
From March 2011 to December 2011, 89 patients with a diagnosis of uterine myoma and a strong desire to preserve the uterus were enrolled for the present study. These patients underwent laparoscopic myomectomy with or without TOUA by a single surgeon (Y.-S.K.) using the procedure described above. The mean age of the group with TOUA was 44.2 years, and that of the group without TOUA was 41.9 years. Table 1 gives clinical information for both the groups, including maximal diameter and number of uterine myomas, symptoms, and history of previous operation. In this study, the operative findings assessed included operation time, estimated blood loss (EBL), and number of cases of laparotomic conversion (Table 2). In the group with TOUA, the operation time was longer compared with the other group, and the mean time difference was 17 minutes (P=.001). In the group with TOUA, the mean total time of TOUA was 14.5 minutes (SD 6.02 minutes). The EBL was significantly less in the group with TOUA than in the group without TOUA (mean EBL of 111.9 mL with TOUA and 203.4 mL without TOUA; P<.001). There was no laparotomic conversion and vascular injury in either group.
Data are mean±SD values or number (%).
TOUA, transient occlusion of uterine arteries.
Data are mean±SD values or number.
From the time of incision of the serosa of the right adnexa to the time of occlusion of the left uterine artery.
Any vascular injury during transient occlusion of uterine arteries (TOUA) involving the adnexal and pelvic side retroperitoneal vessels.
EBL, estimated blood loss.
None of the patients was reported to have fever during their stay in the hospital. The mean hospital stay was 3.32 days with TOUA and 3.09 days without TOUA. The total recurrence rate within 6 months after operation was found to be 5.62% (Table 3).
Data are mean±SD values or number (%).
Recurrence was confirmed by ultrasonography.
TOUA, transient occlusion of uterine arteries.
Discussion
Laparoscopic myomectomy is beneficial for women who want to preserve their uterus with minimally invasive surgery. The benefits include fast recovery time, minimal postoperative pain, and cosmetic satisfaction. Not all women with a uterine myoma can receive laparoscopic myomectomy because of the different and difficult characteristics of uterine myomas. Under similar conditions of uterine myoma, the performance of laparoscopic myomectomy strongly depends on operators who are diverse in surgical skills. In addition, this dependence is strongly related to number, location, and size of uterine myomas: larger, multiple, and deeply located uterine myomas are at high risk for laparoscopic myomectomy.
Laparoscopic myomectomy has several limitations, which include easy excision of the myoma and safe suture of defective myometrium without any dead space. 12 There are few reports dealing with ways to overcome these limitations, but one of these is introduction of surgical techniques. 13 For the beginner in laparoscopic myomectomy, these limitations could be an obstacle to learn any techniques of laparoscopic myomectomy safely and easily. For a safe learning curve of laparoscopic myomectomy, especially for beginners, the safe condition of laparoscopic myomectomy has to be guaranteed regardless of operation time. This safe operative condition can be achieved by less bleeding and a clean operation field regardless of operation time, which are very important for both the beginner and the expert surgeon.
In most cases, to reduce blood loss, surgeons try to shorten operation time or to control bleeding foci by using a coagulation electrode, which may render suturing the burn sites a difficult task. Regardless of operation time and any coagulation procedures, both uterine arteries can be occluded transiently during the operation by using endoscopic vascular clips. About 95% of uterine blood flow is supported by the uterine artery, with the rest by utero-ovarian vessels. Transient blockage of both the uterine arteries can provide surgeons a clean operation field and safe operation conditions. After finishing the operation, the operator can start reflow of both uterine arteries by removing the endovascular clips.
The TOUA method does not need any control over bleeding or the use of any coagulation electrode and can achieve tight suturing of the fresh myometrium with minimal burn injury of the myometrium.
In TOUA, there are a few limitations to safe execution of laparoscopic myomectomy. The major limiting factor is the pelvic space occupied by the uterine myoma; the larger the myoma, the less is the pelvic space. Based on the clinical practice of the surgeon in the present study (Y.-S.K.), a myoma of about 8 cm in diameter is an upper limit size for carrying out laparoscopic myomectomy. The first author has performed laparoscopic myomectomy without TOUA in cases of myoma with a diameter of more than 8 cm (about 10 cm). In the current study, blood loss was statistically significantly different between the group with or without TOUA.
In conclusion, safe performance of laparoscopic myomectomy and extension of the lower bleeding condition can be achieved by TOUA, which may be an important additional technique in difficult laparoscopic uterine procedures, such as myomectomy or uteroplasty.
Footnotes
Disclosure Statement
No competing financial interests exist.