
Abstract
Abstract
Purpose:
Low conversion rate, high safety, and good cosmetic result with less medical cost are chased by all laparoscopic surgeons. We used general laparoscopic instruments and combined with absorbable thread trying to perform a clipless minilaparoscopic cholecystectomy for benign gallbladder patients and got all the above-mentioned results.
Subjects and Methods:
From January 2008 to February 2011, 1096 minilaparoscopic cholecystectomies were performed for patients with uncomplicated or complicated benign gallbladder disease by our treatment team. The three-port technique with the help of an electrocautery hook, forceps, and suction was applied for laparoscopy cholecystectomy, and the cystic duct and vessels were ligated by absorbable thread rather than hemostasis clips and Harmonic® scalpels (Ethicon, Cincinnati, OH). The operative time, blood loss, subhepatic drain, conversion rate, drainage time, and hospital stay were reviewed and statistically analyzed.
Results:
Our conversion rate was 0.18%, which was much lower than those reported by many studies. The mean operating time was 28 minutes (range, 11–70 minutes). Mean blood loss was 12 mL (range, 5–200 mL). A subhepatic drain was placed in 63 patients, with a mean drainage time of 1.7 days (range, 1–6 days). The mean postoperative hospital stay was 2.5 days (range, 2–7 days). No postoperative bleeding, biliary leakage, intraabdominal infection, umbilical site infection, umbilical incision herniation, biliary duct or bowel injury, or mortality occurred.
Conclusions:
Minilaparoscopic cholecystectomy using absorbable thread instead of clips and Harmonic scalpels offers a safe, effective, and economical surgical alternative for benign gallbladder patients.
Introduction
Less invasive methods and better cosmetic results are the constant pursuits of surgeons and instrument companies. In recent years, with the development of minimally invasive technology, many novel surgical approaches such as single-port surgery and natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) have emerged. Despite those new technical innovations, the method for closure of both the cystic duct and artery is still simple in that they are occluded with clips, and most frequently with metal clips. 3 Many reports have shown the disadvantages of using metal clips, which include bile leakage, bleeding caused by accidental dislodgement from a vessel or structure, 4 inflammatory reaction to a foreign body, 5 erosion into adjacent anatomic structures in some instances leading to clip embolism, pancreatitis, and acute cholangitis from intraductal gallstone formation around a surgical clip,6,7 and significant interference for roentologic studies, including computerized tomography and magnetic resonance imaging. 8
Alternative techniques for cystic duct closure have included sutures, a three-throw reef knot, or Roeder slip knots. 9 However, these alternatives are technically more difficult and, therefore, used infrequently. 10 Other techniques, including hemostasis clips (absorbable or unabsorbable clips) and Harmonic® scalpels (Ethicon, Cincinnati, OH),11,12 cannot be routinely used in China, especially in undeveloped areas, for economic reasons. Metal clips continue to be the primary tool used by laparoscopic surgeons.
The aim of this retrospective study of 1096 patients is to present an alternative surgical solution. Clipless mini-LC (MLC) using general laparoscopic instruments and absorbable thread to replace hemostasis clips and Harmonic scalpels allows for a simpler, safe, and effective LC, thereby avoiding the disadvantages of metal clips, reducing costs, and making it possible for this practice to become a routine procedure.
Patients and Methods
From January 2008 to February 2011, in total, 1096 consecutive patients (698 women and 398 men) with benign gallbladder disease were treated by our treatment team using MLC. Most of the patients were admitted from the outpatient department and were assigned randomly to one of three treatment teams in our Department. The three teams are all affiliated with East Hospital, a teaching hospital associated with Tong Ji University, Shanghai, China. The three teams combined did more than 1500 laparoscopic cholecystectomies in a 12-month period. Two of the teams, headed by two different chief surgeons, also performed MLCs, but these teams closed the cystic duct and vessels by hemostasis clips and endoloop, respectively. Their results were not included. All the clipless operations were performed by the same chief surgeon and assistant. Table 1 lists the characteristics of the 1096 patients. The clipless-treated group was composed of patients with both uncomplicated and complicated disease. The uncomplicated patients were scheduled for an elective cholecystectomy and diagnosed with gallbladder polyp, gallstone with chronic cholecystitis, chronic cholecystitis in the mild acute stage, or mild acute cholecystitis. Complicated patients included patients with severe acute cholecystitis, most of whom had gangrenous, empyematous cholecystitis, patients who had a previous history of an upper abdominal operation, and patients who had common bile duct stones. Most of the symptomatic patients were given elective cholecystectomy after fasting and intravenous supplying of antibiotics, antispasmodics, and pain medication, and only a few patients whose symptoms could not be controlled by conservative therapy accepted emergency LC. All patients were given hematologic liver function tests, conventional blood tests, tests for hepatitis B, hepatitis C, and human immunodeficiency virus markers, ultrasonography, chest radiography, and electrocardiography as part of the preoperative routine workup for LC. Magnetic resonance cholangiopancreatography was performed when common bile duct stones or other bile duct diseases were suspected. If common bile duct stones existed, endoscopic retrograde cholangiopancreatography would be performed to take out the stones before the LC, and then elective MLC was arranged. Patients with cholangile cancer or severe hepatobiliary stones and patients whose pathologic results showed gallbladder cancer were excluded.
A different diagnosis may be determined for the same patients.
HBsAg+, hepatitis B surface antigen positive.
Surgical technique
Once the patient was anesthetized using general anesthesia, a second-generation cephalosporin was given. Surgery was then performed using a three-port MLC technique. Routinely we chose the right edge of the umbilicus to make the first port by the open technique. A 10-mm trocar was inserted, and the pneumoperitoneum was maintained at a pressure of 13 mm Hg. If the patient had had a previous abdominal operation, the first trocar was positioned around the umbilicus but as far as possible from the previous incision, avoiding any possible preexisting adhesion under the incision. Guided by the laparoscopy, the second port was made below the xiphoid near the crossing of the liver edge with the ligament teres, and a 5-mm trocar was inserted. The third port was made below the right costal margin as near as possible to the bottom of the gallbladder, where a 3-mm trocar was inserted.
After insertion of the trocars, the gallbladder was evaluated. If there was severe inflammation and adhesion, we first tried to dissect the adhesion and expose the triangle of Calot. There were fewer than 10 cases in which the triangle of Calot could not be dissected clearly. These surgeries were performed in the retrograde fashion, mostly using the anterograde method. The procedure started with the dissection of the neck, opening the pre-membrane, and dissecting the cystic duct using the electrocautery hook, dissecting forceps, and suction. If the gallbladder wall was very thick because of severe inflammation, we changed the right costal trocar to a 5-mm one. After the skeletoning of the cystic duct, a 10-cm-long absorbable thread (VICRYL® W9215; Ethicon) was threaded into the abdomen, and the proximal end of the cystic duct was ligated with the absorbable thread near the common bile duct. Knots were made intraperitoneally with the forceps, and the distal end of the cystic duct was cut directly with the electrocautery hook. The cystic artery was treated using the same method. The gallbladder was further dissected from the liver bed with the electrocautery hook. In place of an expensive manufactured endobag, a sterile condom was used to remove the gallbladder. The condom, with a thread sutured to its neck, was inserted through the 10-mm trocar. After the gallbladder was put into the condom, the scope and trocar were removed. The condom was then dragged by the thread to the umbilical port, and the gallbladder was removed. A subhepatic drain was placed in patients who had severe inflammation or where there was concern about postoperative bleeding or bile leakage (for the whole operating procedure and cosmetic result, see (Figs. 1 and 2, respectively).
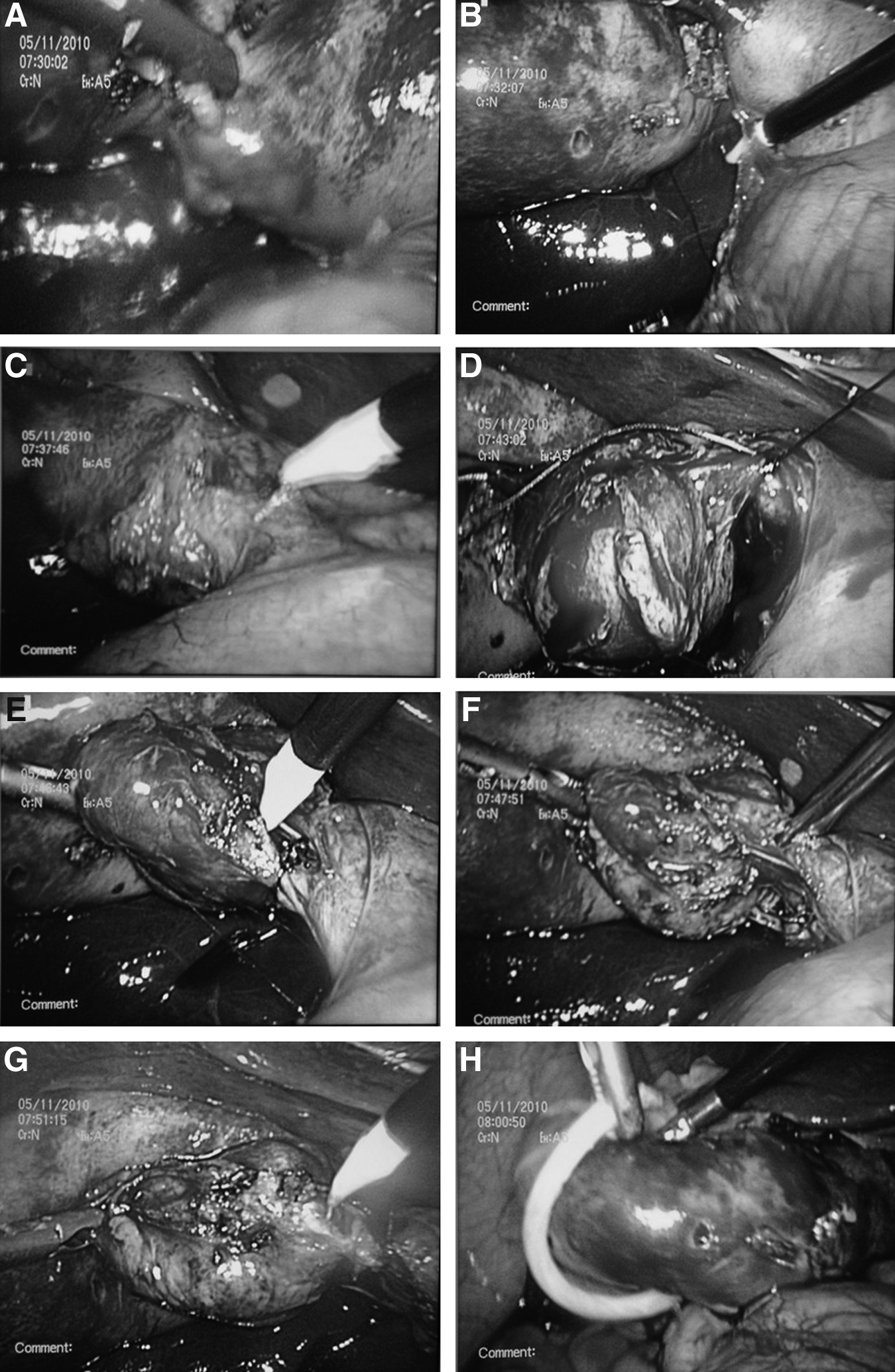
The whole operating procedure of clipless minilaparoscopic cholecystectomy.

Cosmetic result.
Results
Of the 1096 surgeries, 1094 were performed using MLC, and only 2 patients were converted to open surgery, yielding a conversion rate of 0.18%. Reasons for conversion included difficulty exposing the triangle of Calot due to gallbladder perforation in 1 patient and a fistula forming between the gallbladder and duodenum in a second patient. Patients with a previous upper abdominal operation and patients with common bile duct stones were successfully treated. Among the common bile duct stones patients, 1 patient experienced bile duct bleeding, and 2 patients suffered from acute pancreatitis after endoscopic retrograde cholangiopancreatography. All of them recovered smoothly after conservative treatment. Three patients successfully treated by endoscopic retrograde cholangiopancreatography who were found to have common bile duct stones after MLC. Ninety-seven patients needed to be changed from the 3-mm trocar below the costal margin to a 5-mm trocar because of difficulty grasping the gallbladder, which was caused by its severe inflammation. The mean operating time was 28 minutes (range, 11–70 minutes). The mean blood loss was 12 mL (range, 5–200 mL). A subhepatic drain was placed in 63 patients. The mean drainage time was 1.7 days (range, 1–6 days). The mean postoperative hospital stay was 2.5 days (range, 2–7 days). There were no complications such as postoperative bleeding, biliary leakage, or intraabdominal infection. There were no incidences of umbilical site infection, umbilical incision herniation, or injuries to the common bile duct and bowel. The mortality rate was 0% (Table 2). The postoperative time to out-of-bed activity was 2 hours. Patients noted there was only minimal pain after the operation, with only a few pain medications. Because the surgery leaves only two small scars, patients also demonstrated great satisfaction with the cosmetic outcomes.
Data are mean (range) or percentage values as indicated.
Discussion
Laparoscopy is considered the third revolution in medicine, following the introduction of asepsis and anesthesia. The desire for less trauma and better cosmetic result causes surgeons to constantly seek new minimally invasive surgical approaches, which are typically done by a surgeon inserting three to five instruments into a patient through incisions less than 10 mm in diameter. 13 Today we have many minimally invasive surgical methods to select for LC, and typical examples are innovative techniques of MLC, NOTES, and single-incision laparoscopic surgery (SILS). Although NOTES and SILS mark the beginning of a new era in the field of surgery and will be promising techniques in the future, ethical, procedural, and technique limitations prevent them from currently being used for routine LC. 14 So it is important to choose a suitable LC method that can be widely used in clinic practice. Compared with other MLCs, our method has several advantages and can be easily, safely, and economically used in the clinic.
Making and selection of incision
There are two methods for making a transumbilical incision: Veress needle insertion and open technique. Most surgeons choose the lower lip of the umbilicus for making the incision. We chose the right edge of the umbilicus for the open technique. In China, many women have a history of cesarean sections, resulting in a scar in the lower abdomen. In this instance using the open technique is safe. Under direct vision we can avoid damage to the organs, especially the intestines. The right edge is easy to use for incision making because we stand on the left side of the patient. If complications arise it is easy to enlarge the incision without much damage to the muscles. Considering cosmetics, we make the incision in the inner side of the edge, so that the scar is invisible. Based on the size and level of the liver, the other two incisions are always made under the guidance of laparoscopy: on the abdominal wall at the cross point of the liver's lower margin with the ligament teres and the point where the bottom of the gallbladder is located. These sites make it easy to drag and hold the gallbladder and to operate the instruments. To start, we usually make a 3-mm incision below the right costal margin, and if the gallbladder is difficult to grasp because of severe inflammation, we change the trocar to 5 mm. After the operation the umbilicus incision is closed with absorbable suture. Carvalho et al. 15 reported umbilical site infection was present in 1.9% of cases and incisional herniation occurred in 1.0%. We had no umbilical site infection, incisional bleeding, or herniation. All the operations were performed with a three-port MLC without an added extra port, which is different from other clipless LCs reported using a four-trocar method. Using our clipless method patients had better results both internally and cosmetically. For patients with a previous abdominal operation, the first trocar should be placed as far as possible from the previous abdominal incision site, avoiding the adhesion under the incision, but as near as possible to the umbilicus for cosmetic reasons. If no adhesion was detected using the laparoscope, the second and third trocars were inserted on the previous incisions, improving cosmetic results and patient satisfaction.
Closure of the cystic duct and cystic artery
The reported incidence of bile leak ranges from 0.3% to just under 3%. 16 The main cause of bile leakage was cystic duct stump leak, nearly 80% of which originated from the cystic duct. 17 Cystic duct stump leak can occur from clip dislodgement, imperfect clip application, necrosis of the cystic duct stump, or an electrosurgery-related injury. In this study there was no case of bile leakage and no other related complications such as bleeding, biloma, and abdominal infection. Our result was the same as that of Golash, 18 who suggested that an intracorporeal ligature of the cystic duct considerably reduces the cystic duct stump leak. The mean time taken for the cystic duct ligation was 0.8 minutes (range, 0.5–1.5 minutes) shorter than that of Golash 18 (3.5 minutes) because we only made one knot at the proximal end of the cystic duct and cut the distal part directly by electrocautery hook. The method for knot making was different from that of Saha, 19 who made the knot partially intraabdominally; we dragged a 10-mm-long absorbable thread into the abdomen, and the knot was made totally intracorporeally. We ligated both the cystic duct and cystic artery with absorbable thread, a procedure different from that of Carvalho et al., 15 who ligated only the cystic duct and cauterized the cystic artery using monopolar electrocautery, and also different from that of Miller et al., 13 who closed the cystic duct and cystic artery with harmonic scalpel, and Leung et al., 10 who closed the cystic duct and cystic artery with absorbable clips. The absorbable thread was cut from the end part of an absorbable suture (VICRYL w9215), which was used to suture the umbilical incision, so that it did not add the cost of operation. Compared with other methods (Harmonic scalpel and clips), ours was more cost-effective.
Effect of the procedure
Although we used a three-port method, which is more difficult than the four-port one, and the conditions of our patients were more complex and severe in that the pathologic result showed about 10.4% of patients had acute, gangrenous, empyematous cholecystitis (Table 3), our average operative time was only 28 minutes (range, 11–70 minutes), a lower average than most of the studies in this field. It was shorter than those of Carvalho et al. 15 (68.8±31.9 minutes), who replaced the 10-mm trocar below the xiphoid and also replaced the two trocars below the right costal margin with a 3-mm trocar and two 2-mm trocars. Yano et al. 20 (84.6±1.6 minutes) used the absorbable clip. Bessa et al. 21 (32.1±7.6 minutes) and Kandil et al. 22 (33.21±9.62 minutes) both closed the cystic duct and artery with the Harmonic scalpel. Our conversion rate of 0.18% is much lower than other conversion rates in recently published studies (range, 2.6%–7.7%), lower than that of Genc et al. 23 (3.16%), who reviewed the conversion rate of 5164 patients over a 10-year period, and Leung et al., 10 whose conversion rate was 2.7% for uncomplicated and 17.5% for complicated gallbladder diseases. Our mean postoperative hospital stay was 2.5 days (range, 2–7 days), with most patients being discharged within 72 hours, which is longer than that of Carvalho et al. 15 (16 hours) and Kandil et al. 22 (23.44±2.29 hours). Several reasons exist for the longer postoperative hospital stay: patients with acute or severe gallbladder disease need more observation, the cost for hospitalization in China is very low, and culturally Chinese patients are willing to stay longer in the hospital after an operation than Western patients. Given safety concerns, low costs for hospitalization, and patient expectations, both doctors and patients prefer to discharge only when the patient is completely well.
The mortality rate of laparoscopic cholecystectomy was 0.3% 24 in the United States and 0.1% 25 in Europe. We had no mortality. We also had no hemorrhage, bile duct injuries, or bowel damage. All these complications have been widely reported in many published studies on this subject.25,26
Cost savings
Abandoning the use of Harmonic scalpels, various clips, and manufactured endoloops significantly decreased equipment costs18,27 and also avoided certain complications that are inherent to clip usage, especially when the bile duct is very wide or thick. Our method using absorbable thread allows a firm closure and reduces cost.
In order to reduce the cost further we also replaced the manufactured endobag with a sterile condom, which is supplied free by the government. We obtained the informed consent of patients when we used condoms in surgeries. And, there was no injury to patients during surgery or postoperatively. In comparison with the manufactured endobag, the condom was more easily inserted through the 10-mm trocar of the umbilicus and occupied less space. The condom can be easily opened and maneuvered in a limited space and is large enough to hold nearly all gallbladders. There were only a few cases where we turned to use of sterile gloves.
Conclusions
The development of new technology means doctors and patients have expanding treatment options. We need to consider both advantages and disadvantages, such as the clinical utility, cost-effectiveness, and cosmetic results, when evaluating choices. We recognize the positive cosmetic results of NOTES and SILS, but we question the benefits of closing the bile duct and gallbladder vessels using metal clips. We recognize the benefits of closing the bile duct with Harmonic scalpels and performing LC with needlescopy but doubt the overall advantages of always performing the operation with a four-trocar method on patients mostly limited to elective surgery and turning to a thicker trocar if complications are encountered. These methods also require expensive instruments. From a cost-effectiveness standpoint, we believe that these methods cannot be widely implemented in the world today. We conclude that our method is more useful in clinical practice both internally and cosmetically, as well as in cost-effectiveness. The method may be used with many types of gallbladder disease and can been easily grasped after a period of training. Today it is especially useful in China because most places are still underdeveloped, and many patients do not have the means to pay for expensive treatments. Our method, which has lower cost, high safety, and good cosmetic results and is easily taught, brings benefits to both doctors and patients.
Footnotes
Acknowledgments
This work was financial supported by the Technology Development Fund of Shanghai Pudong New Area (number PKJ2009-Y21).
Disclosure Statement
No competing financial interests exist.