
Abstract
Abstract
Objective:
To report success, complication, and atrophy rates, as well as cost analysis and surgeon preference, for standard laparoscopic versus laparoscopic Fowler–Stephens (FS) approaches to intra-abdominal testes.
Patients and Methods:
The records of children who underwent laparoscopic orchiopexy for impalpable testes at our institution were reviewed. Two groups were assessed: Group 1, who underwent a standard laparoscopic orchiopexy; and Group 2, who underwent either a single-stage or two-stage FS orchiopexy. Success was defined as an intrascrotal testis without atrophy. Cost analysis was performed by obtaining operating room charges for the procedures. Surgeon preference was evaluated by calculating the number of each type of orchiopexy performed.
Results:
From 1998 to 2005, 61 laparoscopic orchiopexies were performed on 46 patients. In Group 1, 31 orchiopexies were performed on 22 patients. In Group 2, 30 orchiopexies were performed in 26 patients. Eight orchiopexies were performed on 7 patients in a single stage, whereas 22 orchiopexies in 19 patients were performed in two stages. Two patients underwent both unilateral FS and laparoscopic orchiopexy. Success rates for Groups 1 and 2 were 96.7% and 83.3%, respectively. There were three complications in Group 1 (9.7%) and nine complications in Group 2 (30%). Atrophy rates for the two groups were 6.5% (2/31) and 16.7% (4/24), respectively. The average operating room cost for a standard laparoscopic approach was $3686, $3604 for the first stage and $3909 for the second stage of a two-stage FS approach, and $3785 for a single-stage FS approach.
Conclusions:
Data from this series suggest that completing a laparoscopic orchiopexy in a single operation without ligating the testicular vessels has comparable, if not better, success rates to those of FS procedures, while reducing cost and potentially reducing complications. Outcomes between single- and two-stage FS approaches are similar, but the former can be accomplished at half the cost.
Introduction
Patients and Methods
After Institutional Review Board approval was obtained, a retrospective chart review was performed on all the boys at Children's Mercy Hospital (Kansas City, MO) who underwent laparoscopic evaluation for impalpable testes. Data collected included patient age, surgeon, surgical approach, operative charges, pre- and postoperative exam, length of follow-up, atrophy rates, and complications. All boys who underwent laparoscopic repair of their intra-abdominal testis were included. Those who underwent an open repair or were found to have an atrophic or vanishing testis were excluded. Two groups were assessed: Group 1, those who underwent a standard laparoscopic orchiopexy; and Group 2, those who underwent either a single-stage or two-stage laparoscopic FS orchiopexy. In Group 1 the testis was mobilized laparoscopically and placed into the scrotum in a single stage without ligating the testicular vessels. In Group 2 the testis was mobilized by ligating the testicular vessels and placing it in the scrotum in a single setting or by ligating the vessels and in a separate surgery returning to place the testis in the scrotum. Details of the surgical techniques used have been described previously.10,11 Success was defined as an intrascrotal testis without atrophy.
Success, complication, and atrophy rates were calculated. A cost analysis was performed by obtaining operating room charges for each procedure. Facility, surgeon, and anesthesia fees were similar between groups and were not included. Surgeon preference was evaluated by calculating the number of each type of orchiopexy performed by each of the surgeons at our institution.
Results
From July 1998 to July 2005, 61 laparoscopic orchiopexies were performed on 46 patients with a mean age of 2.1 years (range, 0.25–13 years) and a mean follow-up time of 11.3 months (range, 1–48 months). Follow-up consisted of interval history and examination of the testis. Five patients had incomplete follow-up after their procedure.
In Group 1, the standard laparoscopic orchiopexy group, 31 orchiopexies were performed on 22 patients. In Group 2, the FS group, 30 orchiopexies were performed on 26 patients. Eight orchiopexies were performed on 7 patients in a single stage, whereas 22 orchiopexies on 19 patients were performed in two stages. Success rates for Groups 1 and 2 were 96.7% (30/31) and 83.3% (20/24), respectively. Six patients were lost to follow-up. There were three complications in Group 1 (9.7%) and nine complications in Group 2 (30%). Atrophy rates for the two groups were 6.5% (2/31) and 16.7% (4/24), respectively. Complications included six atrophied testes, three postoperative wound infections, two cystotomies, and one unsuccessful placement of the testis in a dependent position requiring additional surgery.
Analysis of the FS group was further divided into single- and two-stage procedures. In the single-stage group the success, complication, and atrophy rates were 75% (6/8), 37.5% (3/8), and 25% (2/8), respectively, compared with the two-stage procedure yielding respective values of 87.5% (14/16), 37.5% (6/16), and 12.5% (2/16).
Operating room charges were available on 23 of 46 patients: 8 of 22 in Group 1 and 15 of 26 in Group 2 (Fig. 1). The average operating room cost for a standard laparoscopic approach was $3686, versus $6484 for the FS approach. It was $3604 for the first stage, $3909 for the second stage of a two-stage FS approach, versus $3785 for a single-stage FS procedure.
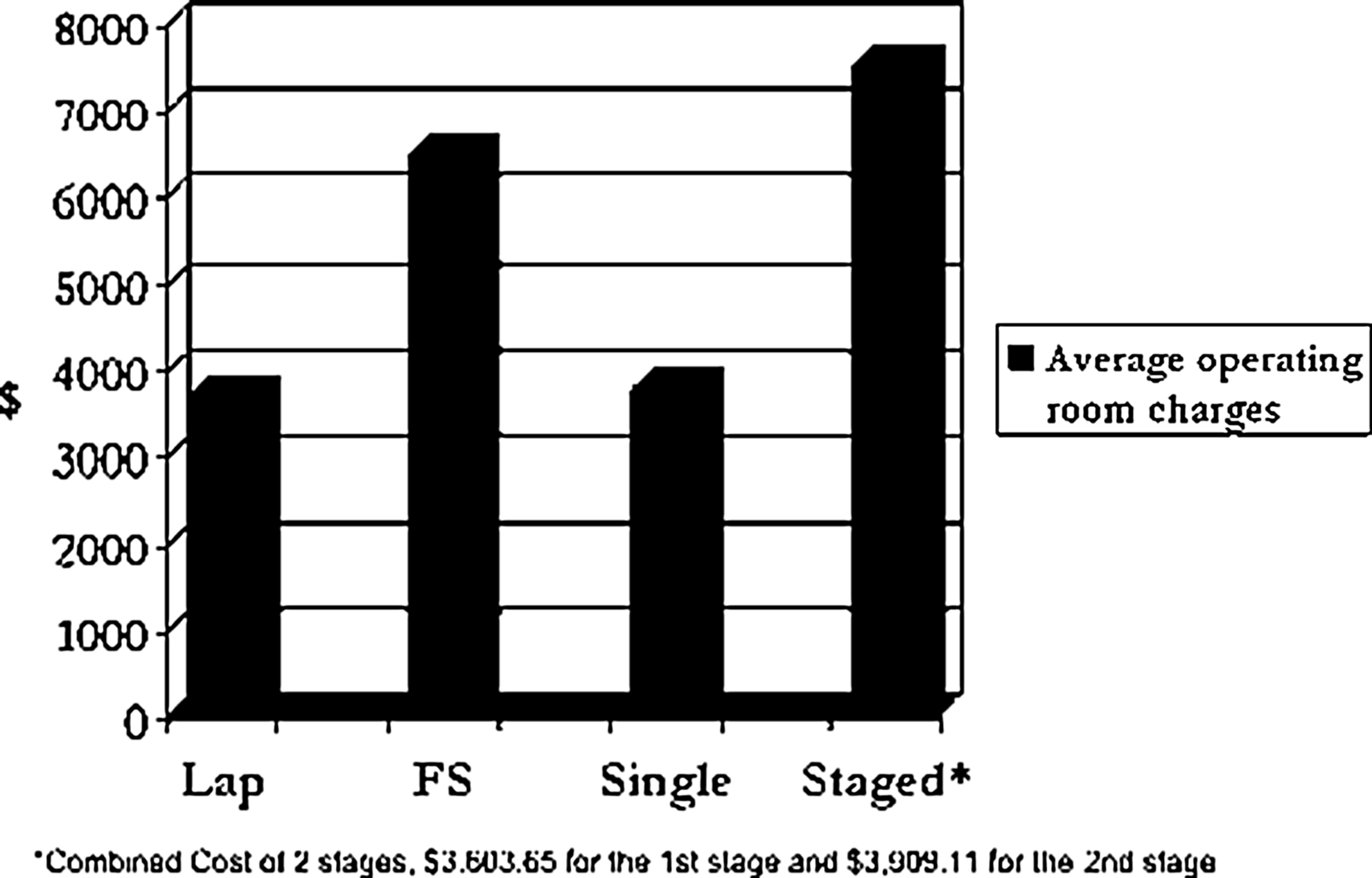
Average operating room charges.
Seven surgeons performed laparoscopic orchiopexies at our institution, identified as surgeons 1–7 (Fig. 2). They performed an average of 8.7 (range, 2–20) laparoscopic orchiopexies each. Surgeons 1–4 performed >87% of their surgeries using the FS approach. Surgeons 1–3 only performed two-stage laparoscopic FS, whereas surgeons 6 and 7 performed >83% of cases using the standard laparoscopic technique. Upon review of the operative reports, the description of position in the operative reports did not differentiate which technique was used.
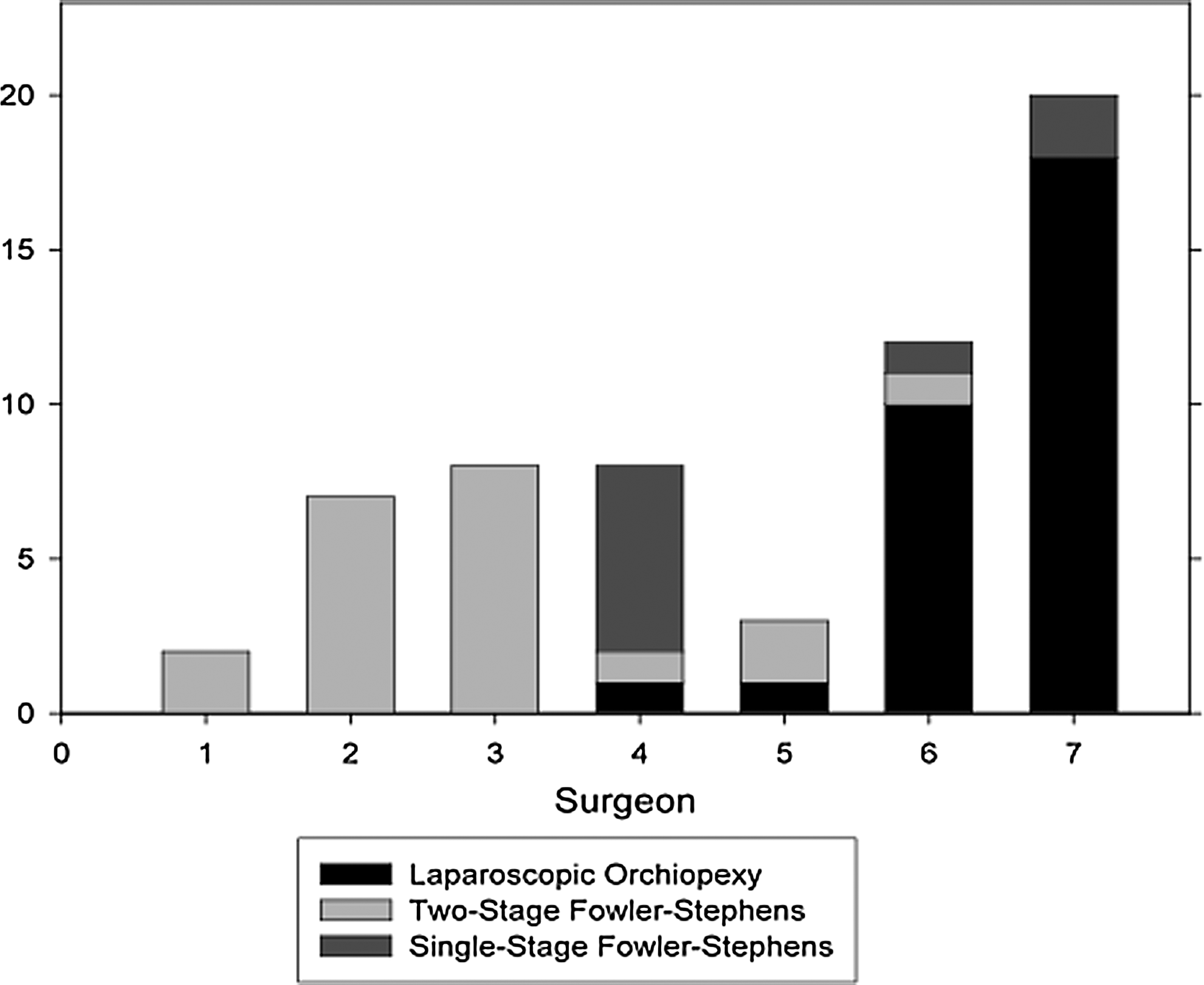
Procedures performed by each of the seven surgeons.
Discussion
Laparoscopic orchiopexy provides a method for both diagnosing and treating intra-abdominal testes. It has been shown in several studies to be both safe and effective.4,7–10,12,13 Historically, open orchiopexy for intra-abdominal testes has a success rate of 74%. 14 Compared with open techniques, laparoscopic orchiopexy has proven to have superior success rates with fewer complications.
Our success and atrophy rates are similar to those found in other studies (Table 1).
FS, Fowler–Stephens; LO, standard laparoscopic approach.
Also, the numbers of testes in our series were similar to those in other studies; however, there were not enough cases to illustrate statistical significance between the groups. The findings of this study reiterate the need for a randomized prospective approach to determine the best surgical approach.
Complications in our series were low, but it is interesting that two of the complications were cystotomies by two different surgeons, which occurred during the second stage of FS approach. In 1 patient the injury occurred during his fourth surgery, as he had previously had a staged FS procedure on the contralateral testis and laparoscopic ligation of the ipsilateral testis. Other studies have also found that atrophy rates are higher in patients who have had prior testicular surgery.7,9 Thus, operating as few times as possible may reduce complications and risk of atrophy.
In reviewing operative notes we found no objective intraoperative measurement or consistent documentation of how high the testes were in the abdomen. The location of the testis was routinely described as “high intra-abdominal” despite the method of orchiopexy. Some studies have adopted specific definitions for location of testes; unfortunately, there is currently no standardization of classification. This poses a significant problem not only for this study, but for any study evaluating treatment modalities for intra-abdominal testes. Because the referral pattern at Children's Mercy is similar for each surgeon, it would not be expected that one surgeon would receive more high intra-abdominal testes than the other surgeons. This led us to investigate the surgical patterns of the seven different surgeons at our institution. It is interesting that we found that most surgeons performed one technique more than another, and thus the location of the testis appeared to play less of a role than did surgeon preference for the technique. It was also noted that the fewer the orchiopexies performed by a surgeon, the more likely it was to be a FS procedure. It is postulated that this is due in part to training and comfort level with a specific technique by the surgeon.
Rising healthcare costs and criticisms that laparoscopy is often more expensive than open surgery motivated us to perform a cost analysis of laparoscopic orchiopexies by obtaining operating room charges for each procedure. Even though a true cost analysis was not performed, our findings support the intuitive notion that two surgeries is equal to nearly double the cost. Each visit to the operating room was around $3000. Our data suggest that for surgeons who perform both techniques, >80% can be done using a standard laparoscopic approach technique, which implies that others who performed primarily staged FS procedures could have done some standard laparoscopic approach at a lower cost and higher success.
Conclusions
Laparoscopic orchiopexy has been well established and is accepted as part of the standard armamentarium for repair of intra-abdominal testes. Data from this series suggest that completing a laparoscopic orchiopexy in a single operation without ligating the testicular vessels has comparable success rates to FS procedures, while reducing cost and potentially reducing complications. It also illustrates that surgeon preference often plays a large role in determining the type of procedure rather than testicle location. If a testis is amendable to a laparoscopic orchiopexy, this is preferable to a FS approach given its lower cost and higher success. If an FS procedure is required, outcomes between a single- and a two-stage procedure are similar, but the former can be accomplished at half the cost.
Footnotes
Disclosure Statement
No competing financial interests exist.