
Abstract
Abstract
Objective:
We introduce a new laparoscopic cholecystectomy by using 2-mm needle-shape instruments and compare it with single-incision laparoscopic cholecystectomy.
Patients and Methods:
From January 2011 to June 2011, 60 patients who satisfied the inclusion and exclusion criteria were prospectively selected and randomized to receive either a scar-hidden novel laparoscopic cholecystectomy (NLC group) (n=30) or a single-incision laparoscopic cholecystectomy (SILC group) (n=30). Their operation time, pain score, and satisfaction score were contrasted.
Results:
All operations were successful. Two patients were converted to conventional three-port laparoscopic cholecystectomy in the SILC group. No postoperative complications occurred in both groups. The operation time was significantly lower in the NLC group (14.17±3.51 minutes in the NLC group versus 24.67±4.12 minutes in the SILC group, P<.01). As to the satisfaction score, the NLC group was superior to the SILC group (4.53±0.57 in the NLC group versus 4.07±0.52 in the SILC group P<.01). There was also a lower postoperative pain score in the NLC group, although the results did not reach statistical significance.
Conclusions:
The new scar-hidden laparoscopic cholecystectomy is a safe and feasible technique. Compared with single-incision laparoscopic cholecystectomy, it has a lower operation time and less difficulty but a higher satisfaction score. It demonstrates a new approach for minimal invasive surgery.
Introduction
Patients and Methods
For this study, 60 patients with benign gallbladder disease such as chronic cholecystitis, cholelithiasis, and gallbladder polyps were selected. Patients with acute illness and a history of abdominal surgery were excluded from the study. They were randomly divided into two groups, with 30 patients in each group. The novel LC patients (NLC group) had an average age of 51.83±8.51 years and a body mass index of 24.58±1.96 kg/m2, and the SILC patients (SILC group) had an average age of 51.07±8.13 years and a body mass index of 24.56±2.09 kg/m2. Statistically, the two groups had no significant differences in terms of age or body mass index (P>.05) (Table 1). All interventions were performed by the same operative team at East Hospital of Tongji University in Shanghai, China, and the study was approved by the Institutional Review Board of Tongji University.
Data are mean±standard deviation values.
BMI, body mass index; NLC, novel laparoscopic cholecystectomy; SILC, single-incision laparoscopic cholecystectomy.
Instruments
The 2-mm needle-shape grasper and electrocautery (Fig. 1) were specially designed by the authors and manufactured by KANGJI Medical Device Co. Ltd. (Hangzhou, Zhejiang Province, China). These products were approved for clinical use by the Chinese State Food and Drug Administration. The ultrasonic Generator 3000 and the 5-mm Harmonic® scalpel were purchased from Ethicon Endo-Surgery, Inc. (Cincinnati, OH). The scissors were developed by Wilson Instruments Co. Ltd. (Shanghai).

The specially designed 2-mm needle-shape grasper and electrocautery device.
Operative procedures
The preoperative preparation was the same as for conventional LC. Anesthesiologists followed the same general anesthetic protocol. In both groups, during laparoscopy the gas used was CO2.
NLC procedure
The patients were placed in the 30° reverse Trendelenberg position. The monitor was set on the right side of the patient, with the operator and assistant standing on the left side. A 15-mm incision was made at the right side of the umbilicus; a 10-mm trocar for the optic unit and another 5-mm trocar for the ultrasonic scalpel or clips were inserted side by side into the incision. A 2-mm needle-shape grasper was placed direct through the abdominal wall in the midclavicular line 20 mm inferior to the costal margin, and the electrocautery device was placed 20 mm inferior to the xiphoid (Fig. 2). After the gallbladder had been grasped and lifted, the triangle of Calot was exposed for dissection (Fig. 3). Then the next steps were the same as for conventional LC. The fascial incisions were closed with an absorbable suture, and the umbilicus was restored with absorbable cutaneous stitches to its physiologic position (Fig. 4).

Positions of trocars and instruments. A 10-mm trocar and another 5-mm trocar were inserted side by side into the umbilical incision. A 2-mm needle-shape grasper was placed in the midclavicular line 20 mm inferior to the costal margin, and the electrocautery device was placed 20 mm inferior to the xiphoid.
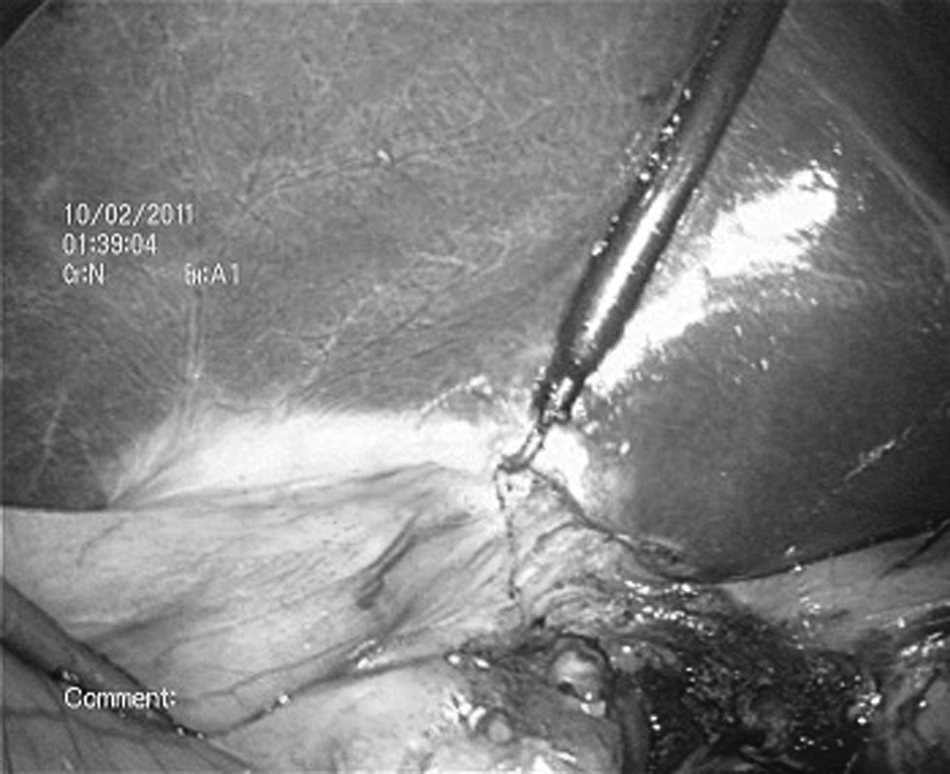
Exposure of the triangle of Calot during the operation.

The scars of the novel covert laparoscopic cholecystectomy 7 days postoperatively.
SILC procedure
In brief, the patient was placed in the lithotomy position. The operator stood between the patient's two legs, and the assistant stood on the left side of the patient. The monitor was placed near the patient's head. A 20-mm incision was made at the right side of the umbilicus for insertion of the Triport™ (Olympus/Advanced Surgical Concepts, Bray, Ireland). Finally, the gallbladder was removed through the umbilical incision after hemostasis of the gallbladder bed was ensured and no drainage was left. The closure of incision was similar to that with the NLC procedure.
Outcome measure
The primary outcome measures were the number of patients converted to traditional LC and operation time. Secondary outcome measures were postoperative abdominal pain and incision satisfaction. Abdominal pain was recorded at 24 hours postoperatively. To assess postoperative pain, a visual analog scale with a 10-cm vertical score ranging from “no pain” (score 0) to “worst possible pain” (score 10) was used. After the patients had been adequately instructed about the range for measuring pain, they selected a value on the scale (between 0 and 10). When patients were discharged 2 days postoperatively, the satisfaction score for the incision was evaluated. Scores ranged from “worst satisfaction” (score of 1) to “best satisfaction” (score of 5). We used a picture of “the incisions of normal LC” as the objective reference. Then all the patients determined the score of satisfaction with their incisions compared with the same picture.
Statistical analysis
Statistical analysis for operation time, pain intensity scores, and satisfaction scores were performed by using the Mann–Whitney U test. Disease difference between groups was assessed by use of the chi-squared test. Patient demographic data were compared using the t test. All statistical analyses were conducted by using SPSS statistical software (version 15.0; SPSS, Inc., Chicago, IL). The level of significance was set at .05.
Results
All operations were performed successfully. Two patients were shifted to conventional three-port LC in the SILC group. All patients felt well postoperatively and did not required analgesics. They were discharged 48 hours after the operation. No postoperative complications occurred in both groups at the 1-month follow-up evaluation in the outpatient clinic.
The operation time in the NLC group (14.17±3.51 minutes) was significantly shorter than in that in the SILC group (24.67±4.12 minutes) (P<.01). As to postoperative pain score, the value in the NLC group was lower than that in the SILC group, although the results did not reach statistical significance. The incision satisfaction score was 4.53±0.57 in the NLC group and 4.07±0.52 in the SILC group (P<.01, significant difference) (Table 2).
Data are mean±standard deviation values.
P<.01.
NLC, novel laparoscopic cholecystectomy; SILC, single-incision laparoscopic cholecystectomy.
Discussion
In the last decade, NOTES and SILS were developed with the aim of reducing the invasiveness of traditional laparoscopy. The surgeon's interest was focused on reducing the invasiveness and scarring caused by the procedure. Towards nonvisible scar surgery, research is conducted mainly through the following ideas. First, new access was obtained to the peritoneal cavity, represented by NOTES, which was first described by Kalloo et al. 1 in 2004. It completely eliminated anterior abdominal wall incisions but was hampered by difficulty in accessing anatomical sites, lack of appropriate devices, and sterility. Second, the incision was hidden in the anterior abdominal wall. The limitations of NOTES led to the concept of transumbilical endoscopic surgery (TUES) 2 or SILS, 3 which also produced a nonvisible scar as it was hidden easily in the umbilical plica. However, TUES or SILS is also more technically difficult than traditional laparoscopic surgery because of challenges such as loss of triangulation and external and internal conflict of instruments. 4
As the approaches mentioned above were fraught with problems, we attempted other methods and termed them “scar-hidden LC”: (1) We transferred the incision to the superior margin of the suprapubic hair. Our research indicated that the approach (one 10-mm trocar above the umbilicus with two 5-mm suprapubic trocars) was characterized by no visible scar, a shorter operation time, minimal bleeding, etc., but longer instruments should be used. 5 (2) We placed the incision at the linea alba or at a previous operation scar (data not shown). (3) We reduced the size of incision. According to our previous study, 6 the optimized two-trocar TUES technique (a 2-mm trocar inserted for a grasper in the right upper abdomen) was found to be faster and less painful than the TUES approach.
Under the guidance of reducing the size of incisions, we proposed another novel “scar-hidden LC” as described in the NLC procedure. Using the 2-mm needle-shape instruments, the new technique has following advantages:
1. The 2-mm grasper and the electrocautery device are at the normal location, the same as for the traditional laparoscopic surgery. It helps to regain triangulation for manipulation, which not only enables performing sufficient traction of the gallbladder but also allows good mobilization of the gallbladder in order to dissect the triangle of Calot safely. 2. Compared with SILC, the novel covert LC was performed more feasibly and safely, with a significantly shorter operation time and higher satisfaction score. Cosmesis, safety, operability, and economy were balanced better in this new technique. 3. The scars of the new technique were hidden in the natural folds of the skin around the navel and were too small to affect cosmesis while the 2-mm puncture hole on the upper abdomen was healing. Compared with conventional laparoscopic surgery, it produced better cosmetic results, whereas the operative time was almost equal according to our data.
Certainly, the novel scar-hidden LC has several limitations, including the small number of patients involved in the analysis and the fact that patients with acute illness were excluded. Besides, because of shrinking of the incision diameter, the grasper's tractive effort was not as good as that for conventional laparoscopic instruments. To overcome this problem and reduce transformation, the length of these instruments was shortened.
In conclusion, the safety and feasibility of this novel procedure are comparable with those for conventional LC. At the same time, it almost achieves a “nonvisible scar.” A new technique was provided for minimal invasive surgery.
Footnotes
Acknowledgments
We thank KANGJI Medical Device Co. Ltd. for providing the equipment that made this study possible.
Disclosure Statement
No competing financial interests exist.