
Abstract
Abstract
Purpose:
As the interest in minimal invasive surgery has turned to single-site access surgery, single-incision laparoscopic surgery (SILS) is becoming popular. Recently limited numbers of pediatric SILS series have been published. SILS needs nonconventional three-lumen ports and articulated working instruments. However, it is possible to perform single-port laparoscopic cholecystectomy using a single conventional port and conventional working instruments. We herein present our preliminary experience with cholecystectomy conducted with single-port incisionless-intracorporeal conventional equipment-endoscopic surgery.
Subjects and Methods:
During December 2009–October 2012, 27 patients (12 boys, 15 girls) underwent single-port incisionless-intracorporeal conventional equipment-endoscopic cholecystectomy. A 10-mm 0° scope with a parallel eye piece and an integrated 6-mm working channel is inserted through an 11-mm “conventional umbilical port.” Conventional working instruments were introduced through the integrated working channel. The fundus of the gallbladder is hung with a transabdominal sling suture. The infundibulum is retracted laterally to expose the triangle of Calot with a second transabdominal sling suture. Then the cystic duct and the artery are dissected and clipped separately. The gallbladder is dissected from the liver bed with monopolar cautery and extracted through the umbilicus.
Results:
The patients were 5–17 years of age (mean, 10.7±4.6 years). Cholecystectomy was performed through a single port in 23 patients. A second port insertion was necessary in 4 patients. No preoperative or postoperative complications were encountered. Mean operating time was 74.3±13 minutes.
Conclusions:
Single-port incisionless-intracorporeal conventional equipment-endoscopic cholecystectomy is feasible in pediatric patients with reasonable operating times. It is a safe, cheap, and highly minimal invasive procedure with excellent cosmetic results.
Introduction
Subjects and Methods
During December 2009–October 2012 all patients requiring cholecystectomy (27 patients; 12 boys, 15 girls) underwent single-port incisionless-intracorporeal conventional equipment-endoscopic cholecystectomy. A 10-mm 0° operating scope with a parallel eye piece and an integrated 6-mm working channel (Karl Storz, Tuttlingen, Germany) was used for laparoscopy. The cost of this operating scope is 15% more expensive compared with standard (without integrated working channel) scopes. The operating scope was inserted through an 11-mm “conventional umbilical port” with the Hasson technique (Fig. 1). Pneumoperitoneum was created with CO2 insufflations up to 10 mm Hg pressure. Conventional working instruments were introduced through the integrated working channel, one instrument at a time. The fundus of the gallbladder was hung with a transabdominal sling suture using a 2-0 silk suture with a straight cutting needle (Fig. 2). The sling suture was introduced to the abdomen from the midclavicular line at the costal margin or between the 11th and 12th ribs, under laparoscopic guidance (Fig. 3). The needle was grasped with a laparoscopic needle-holder (Karl Storz), passed through the fundus of the gallbladder, and then taken out of the abdomen close to its entry point. The two ends of the suture were held with a hemostat. The infundibulum was retracted laterally to expose the triangle of Calot with the aid of a second transabdominal sling suture introduced through the right side of the abdominal wall (Fig. 4). The pericholecystic adhesions, if present, were freed with blunt dissection. Then the cystic duct and the artery were dissected with a conventional endoscopic dissector (Karl Storz) and L-shaped monopolar cautery (Karl Storz). The desired traction was maintained by manipulating the sling sutures. The artery and the cystic duct were double-clipped (Hem-o-lok™; Weck Closure Systems, Teleflex, Research Triangle Park, NC) separately (Fig. 5). The gallbladder was dissected from the liver bed with the help of monopolar cautery and extracted through the umbilical port or umbilical port site.
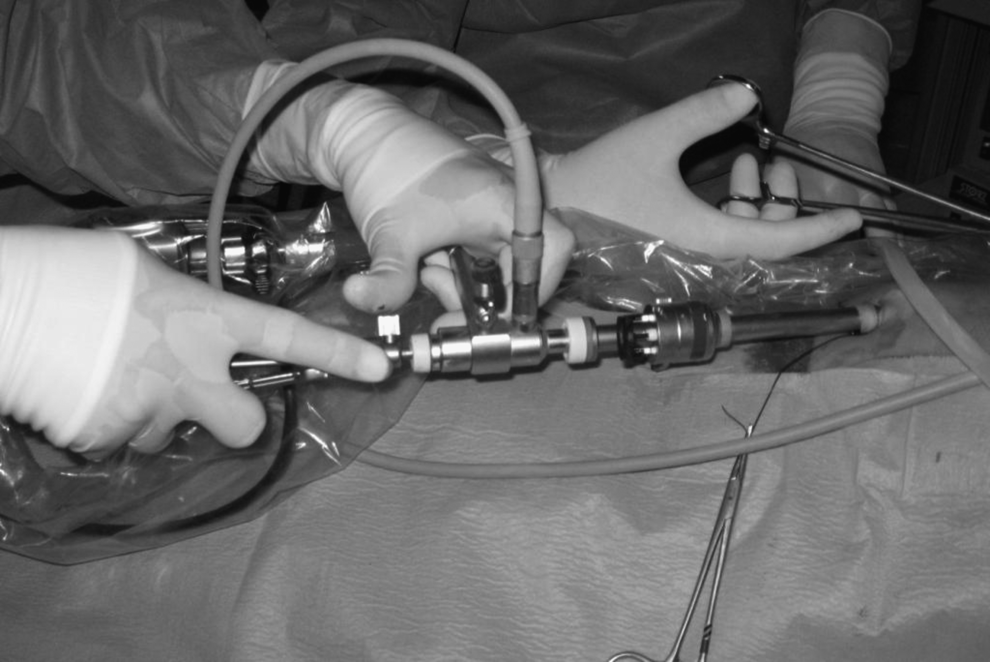
Operating scope introduced through a single conventional umbilical port.
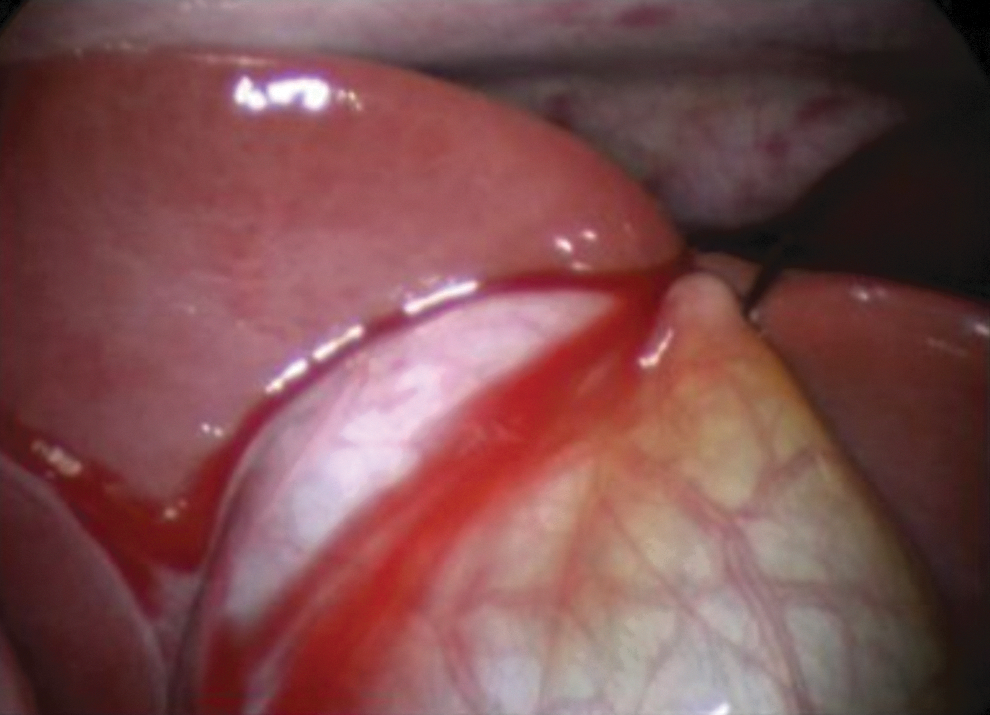
Sling suture at the fundus of the gallbladder.

Appearance of the sling suture introduced to the abdomen from the midclavicular line between the 11th and 12th ribs.

Sling suture retracting the infundibulum of the gallbladder.
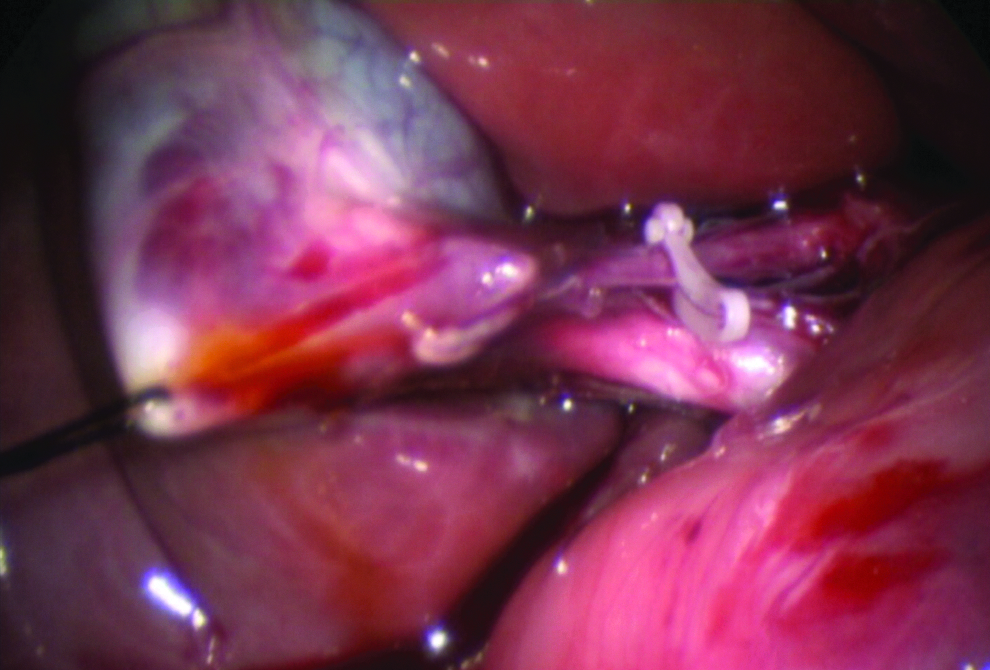
Plastic locking clip at the cystic artery.
Postoperative pain control was managed with preoperative infiltration of bupivicaine (1 mg/kg per dose) to the umbilical incision site, and intravenous or rectal paracetamol (10 mg/kg per dose) was given to all the patients at 6-hour intervals on the postoperative first day.
The data were expressed as mean±1 standard deviation values.
Results
The patients were 10.7±4.6 years old (range, 5–17 years). This procedure was performed by five different surgeons.
Patients' characteristics are shown in Table 1. Cholecystectomy was performed through a single port in 23 of the 27 patients. A second port insertion was necessary in 4 patients to dissect the gallbladder from the adhered organs or from the surrounding fatty tissue. Body mass indexes of these 4 patients were between 26.5 and 31.2 kg/m2. Additionally, 2 of these patients had acute cholecystitis with inflammation.
Data are mean±standard deviation values.
BMI, body mass index.
None of the patients had chronic cholecystitis or symptomatic cholelithiasis. The mean operating time was 74.3±13 minutes. Gallbladder drainage was not performed before resection. Spillage from the gallbladder was seen in 3 patients in whom only aspiration was performed. No intraoperative complications were encountered.
The mean hospital stay of the patients was 2.2±0.6 days (range, 1.5–3 days). Postoperative recovery was uneventful for all patients. No postoperative complications such as wound infection were encountered. Cosmetic results of the port insertion site, the umbilicus, were excellent according to the patients' and the parents' definition (Fig. 6). There was no residual scar formation at the sling suture insertion sites. Average follow-up of the patients was 4.5±1.9 weeks (range, 2–8 weeks).

Postoperative view of the port insertion site at the umbilicus.
Discussion
Four-port laparoscopic cholecystectomy is the “gold standard” in the treatment of patients with cholelithiasis.9,10 As endoscopic surgery evolves toward being less and less invasive, scarless surgery, many new techniques have been developed to minimize the wound scars. To minimize the number of the ports, pain, and scar formation, SILS, also termed single-site access surgery (SSA), has come into practice and started to be preferred in many laparoscopic procedures.4,11–14
Recently SILS cholecystectomy has been introduced as an alternative to the standard multiport laparoscopic cholecystectomy in adult patients.15,16 When performing SILS, usually a nonconventional three-lumen port 20–30 mm in size and articulated working instruments are being used. These nonconventional instruments are more expensive than the conventional ones; therefore, to lower the cost alternative techniques have been developed. In place of using a nonconventional umbilical port, transumbilical multiport access has been reported for SSA laparoscopic cholecystectomy.2,17–21 In this procedure, multiple ports are introduced into the abdomen from a single umbilical skin incision but with separate fascial incisions. Then the operation is conducted with conventional or nonconventional instruments. To decrease the number of the ports, Navarra et al. 22 first suggested in 1997 usage of multiple transabdominal sling sutures to retract the gallbladder, thus reducing the number of the ports to 2 (one in umbilicus, one from epigastrium) for laparoscopic cholecystectomy. Two years later, Piskun and Rajpal 23 reported laparoscopic cholecystectomy that was transumbilical and single incision and used two umbilical ports with the aid of sling sutures. SSA laparoscopic cholecystectomy using a single conventional port and only conventional laparoscopic instruments was reported in 2009 by Bucher et al. 24 In this series, the authors used conventional instruments (i.e., a 12-mm umbilical port, a 10-mm operating scope with a 6-mm working channel, a dissector, hook cautery, endoscopic clips, and two transabdominal sling sutures) to perform cholecystectomy.
Although SILS is gaining popularity in adult patients, there are limited reports concerning pediatric patients published in the literature.1–6 Apart from the high cost of the instruments, a relatively large umbilical incision (approximately 2–3 cm) compared with pediatric patient size is the other disadvantage of SILS in pediatric patients. Clashing of the instruments in a limited, restricted space in children and the loss of the triangulation complicate the procedure. However, it is possible to perform SSA laparoscopic surgery using conventional working instruments, through a conventional 11-mm umbilical port. In our institution, since 2005, we have been performing single-port laparoscopic appendectomy with a conventional port and instruments.7,8 We named our technique single-port incisionless-intracorporeal conventional equipment-endoscopic surgery. 8
We have been performing single-port incisionless-intracorporeal conventional equipment-endoscopic cholecystectomy since 2009, with the technique similar to that of Bucher et al. 24 For our new cholecystectomy technique, unaware of the literature, we had inspiration from single-port incisionless-intracorporeal conventional equipment-endoscopic appendectomy and adapted the procedure to laparoscopic cholecystectomy. During our literature search we encountered the reports of Bucher et al. 24 and Piskun and Rajpal. 23 Other adult series of SSA multiport laparoscopic cholecystectomy using sling sutures have been published.19,25 Garcia-Henriquez et al. 26 had reported a pediatric series where cholecystectomy was performed via a SILS port together with sling sutures. However, there are no pediatric series of SSA laparoscopic cholecystectomy performed using the technique described in the present series. So far this is the first pediatric single-port–single-instrument cholecystectomy series in the literature.
SSA laparoscopic surgery performed with nonconventional ports and single-incision transumbilical multiple ports has an increased potential of developing a hernia.6,21,25 The wide fascial incision done to place the nonconventional ports poses a risk for development of fascial defects. During “single-incision transumbilical multiple-port” procedures, the two or three closely placed fascial incisions and the tight-fitting instruments within a narrow area affect the blood supply and may lead to necrosis and port-site hernias.6,19,25 During single-port incisionless-intracorporeal conventional equipment-endoscopic cholecystectomy, all the operation is done through a single 11-mm umbilical port with an operating scope having an integrated working channel, which minimizes the hernia risk.
One disadvantage of the operating scope is that the surgeon has to operate in one axis without the advantage of “triangulation” of the instruments. This is also a disadvantage of SILS. For those surgeons who do not have experience with an operating scope, the management of the scope and the working instrument might be complicated at the beginning as the camera moves parallel with the working instrument. However, this inconvenience is easily overcome with practice. The other advantage of using an operating scope is that it provides easier control of the camera movements. As the camera moves parallel with the working instrument, it is easier to keep the target in the middle of the view. Additionally, the operating surgeon controls the zoom in and out. Thus operating surgeon controls all of the camera's movements without the need for an extra person just to operate the camera. Because the surgeon controls the camera's movements by him- or herself, this technique can also be named “single-surgeon therapeutic laparoscopy” through a single conventional port.
In a prospective randomized trial, Ostlie et al. 27 had compared SILS with standard four-port laparoscopic cholecystectomy; they emphasized that the operating times and the degree of difficulty for SILS cholecystectomy were significantly greater than for four-port cholecystectomy. In the present series, the average operative time was longer than that for standard multiport laparoscopic cholecystectomy. However, we think that dissection of the triangle of Calot in overweight patients with gallbladder inflammations is more difficult compared with multiport cholecystectomy. Therefore standard multiport laparoscopic cholecystectomy should be preferred in overweight patients.
During single-port incisionless-intracorporeal conventional equipment-endoscopic cholecystectomy, as the umbilical incision (1 cm) is done inside the umbilicus, the scar does not exceed the umbilical margins. It is hidden inside the belly pit, forming an invisible scar. All of the patients and the parents were content with the cosmetic results of our current cholecystectomy technique. Because the only incision is about 1 cm long, the postoperative pain is minimal and easily controlled.
Single-port incisionless-intracorporeal conventional equipment-endoscopic cholecystectomy is feasible in pediatric patients with reasonable operating times. Because it is performed totally with conventional laparoscopic instruments, it is cost-effective. The current technique is a real “scarless” surgery. The surgeon controls the camera movements by him- or herself; thus current technique enables “single-surgeon therapeutic laparoscopy.” These are the advantages of the current technique over SILS procedures like appendectomy and cholecystectomy. The current cholecystectomy technique is a safe, cheap, and highly minimal invasive procedure with excellent cosmetic results.
Footnotes
Disclosure Statement
No competing financial interests exist.