
Abstract
Abstract
Background:
Although current guidelines recommend performing cholecystectomy via laparoscopy, consensus on the application of single-incision laparoscopic surgery for cholecystectomy is still lacking. The aim of the current study was to perform a meta-analysis of randomized controlled trials (RCTs) and nonrandomized comparative studies (NRCSs), comparing single-port laparoscopic cholecystectomy (SPLC) and conventional multiport laparoscopic cholecystectomy (CMLC) for benign gallbladder diseases.
Subjects and Methods:
A systematic review of the literature was performed to identify studies published between January 1997 and December 2012 comparing SPLC and CMLC. Operative outcomes, postoperative parameters, complications, cosmetic results, and quality of life were evaluated.
Results:
Forty studies were included in the analyses (16 RCTs, 24 NRCSs) that included 3711 patients (1865 SPLCs, 1846 CMLCs). SPLC had higher conversion rates (odds ratio [OR], 4.21; 95% confidence interval [CI], 2.71–6.56; P<.001), longer operating time (mean difference [MD], 16.1; 95% CI, 9.93–22.26 minutes; P<.001), and shorter hospital stay (MD, 0.16; 95% CI, −0.28 to −0.04 day; P=.01) than CMLC. There were no significant differences between the two procedures for early (MD, −0.1; 95% CI, −0.44 to 0.24; P=.57) or late (MD, −0.13; 95% CI, −0.45 to 0.19; P=.42) visual analog scale pain scores and overall complications (OR, 1.21; 95% CI, 0.92–1.61; P=.18). Cosmetic outcomes favored SILC at 2 weeks (MD, −1.39; 95% CI, −2.66 to −0.12; P=.03) and 1 month (MD, −0.13, 95% CI, −2.05 to 0.55; P=.0007) after surgery (index score, 0–10).
Conclusions:
SPLC can be performed safely and effectively with better cosmetic results than with the CMLC technique for benign gallbladder diseases.
Introduction
At present, SPLC is gaining more and more popularity, and with the aim of minimizing invasiveness it may replace CMLC, achieve reduced postoperative pain, and optimize cosmetic results.6,7 The initial evidence in support of SPLC was mostly based on single-institution case series and a few randomized controlled trials (RCTs). At present, several systematic reviews and meta-analyses, which synthesized data obtained from published RCTs to evaluate the feasibility and safety of SPLC by comparison with those of CMLC, have been published.8–12 SPLC was reported to have higher procedural failure rates and longer operative times than cases associated with CMLC. There were no significant differences in overall complications between the two procedures. In addition, conflicting results in the incidence of incisional hernia and cosmetic outcomes were observed among these meta-analyses. However, most of the previous meta-analyses included small sample sizes; the pooled results of these studies may be unreliable and underpowered for comparison among surgical techniques because potential studies and publication biases are more likely to occur. Furthermore, there is evidence that estimates derived from high-quality nonrandomized comparative studies (NRCSs) may be similar to those derived from RCTs, and when comparing surgical procedures, pooled analysis of high-quality NRCSs may be as accurate as those of RCTs.13,14 However, to date, no meta-analysis has combined the data of any published RCTs and NRCSs.
Therefore, we conducted the first study that included the largest available dataset from RCTs and NRCSs to overcome these limitations, to evaluate the safety and efficacy of SPLC in patients with benign gallbladder diseases, and to determine whether SPLC is an alternative to CMLC. Potential advantages of each technique were indentified using the meta-analytical method and sensitivity analyses.
Subjects and Methods
Type of intervention
For the purpose of this study, we defined SPLC as a surgery performed through a single skin incision regardless of the surgical device used, and CMLC was defined as the standard three- or four-port procedure. Laparoscopic-assisted and robotic laparoscopic cholecystectomies were excluded.
Literature searches
To identify all potential relevant articles that evaluated SPLC versus CMLC for benign gallbladder diseases, two reviewers independently searched the electronic databases PubMed, Embase, and the Cochrane Library according to the 2009 PRISMA statement. 15 The search terms belonged to the MSH database and included “laparoscopy,” “single incision,” “single port,” “multi-incision,” “multi-port,” “cholecystectomy,” “randomized controlled trial,” and “comparative study.” These terms were searched individually as well as in combination. In addition, we manually searched the Google Scholar database and five high-impact journals (Annals of Surgery, Journal of the American College of Surgeons, British Journal of Surgery, Archives of Surgery, and Surgical Endoscopy) from January 1997 to December 2012. For additional articles, the reference lists of these articles were selected for full-text review. We completed the literature search in December 2012.
Inclusion and exclusion criteria
Inclusion criteria were (1) cohort comparisons of SPLC and CMLC, (2) reported at least one of the following essential measured outcomes such as operative parameters, postoperative outcome, postoperative complications, cosmetic outcomes, or quality of life (QoL), and (3) when two studies were reported by the same institution (and/or authors), only the latest or the most detailed and informative article, or the one with the best quality in methodology, was included. However, this was not applicable if the outcome measures were mutually exclusive or measured at different time intervals.
Exclusion criteria were (1) previously published cohorts with considerable overlap, (2) the essential outcomes of interest were impossible to calculate or the standard deviation and confidence interval of the tested parameters were not reported, (3) studies involving exclusively robotic procedures, (4) letters, editorials, expert opinions, abstract, reviews, or meta-analyses without original data, and (5) studies written in languages other than English.
Two reviewers independently screened the title and abstract of publications for this study. Citations having suspected compliance with our eligibility criteria underwent a full review. The two reviewers independently determined the eligibility of all included publications for a full-text evaluation during the screening process, and disagreements were resolved through discussions between the two reviewers. To resolve disagreements, a third person made a final decision on the eligibility of the study.
Outcomes of interest and definitions
The following outcomes were used to compare SPLC with CMLC procedures:
1. Operative parameters: operative time (minutes), estimated blood loss (mL), and conversion rate 2. Postoperative outcomes: length of hospital stay (days), wound length (mm), early visual analog scale (VAS) pain scores, late VAS pain scores, total analgesic requirement (mg), and the time taken by the individual to return to work (days) 3. Postoperative complications: overall complications, wound infections, wound hematoma, incisional hernia, retained common bile duct stone, bile duct injury, bile leakage, and pneumonia 4. Cosmetic outcomes 5. QoL
A standard 10-cm VAS with options ranging from 0 (no pain) to 10 (worst pain) was used to assess postoperative pain scores. Early postoperative pain was assessed 2–48 hours after surgery, whereas late postoperative pain was assessed from 72 hours to 1 week after surgery.
An index scored from 0 (no satisfaction) to 10 (complete satisfaction) was used to assess the cosmetic satisfaction result. For the operative parameters, the following situations were recognized as conversions to SPLC procedure: (1) conversion to CMLC; (2) conversion to open technique; and (3) need for another incision or trocar outside the umbilicus except suture retraction. For CMLC, conversion to open surgery, conversion to SPLC, or use of an extra trocar was considered to be a failure.
Data extraction
The following variables were independently extracted from the included studies by the two reviewers: name of the first author, year of publication, study design, definition of SPLC, characteristics of study population, indications for surgery, number of subjects operated upon with each technique, and perioperative outcomes. The same consensus process mentioned above was used to resolve disagreements. Furthermore, to obtain these data, we contacted the authors of eligible studies if there were missing data or inaccurate information extracted from the original article. If the author failed to respond, the study was excluded from the outcome analysis.
Quality assessment
Two authors (J.Q. and H.Y.) examined the studies independently and extracted data according to a predefined criteria. The methodological quality of each RCT was evaluated by individual components based on the Cochrane risk of bias tool. 16 For NRCSs, the quality of the studies was assessed by using the Modified Newcastle–Ottawa Score, 17 which allocates a maximum of 9 points each to patient selection, the comparability of the two groups (SPLC and CMLC), and outcome assessment.
Statistical analysis
This meta-analysis was performed in line with recommendations from the Cochrane Collaboration and the Quality of Reporting of Meta-analyses guidelines.18,19 The statistical software Review Manager version 5.0 (The Cochrane Collaboration, Oxford, United Kingdom) was used to perform all statistical analyses. For the analysis, continuous data with mean differences (MDs) and corresponding standard deviations were presented as weighted MDs with 95% confidence intervals (CIs). However, odds ratios (ORs) with 95% CIs as the summary statistics were used to perform statistical analysis for dichotomous variables. Clinical heterogeneity was tested by means of the I2 value; a value exceeding 50% was considered to represent a significant difference. A random-effects model was used to report the results of heterogeneous data; otherwise, a fixed-effects model was used. Funnel plots were constructed to detect and assess publication bias and any associations between treatment estimates and sample size. Forest plots were constructed, and the value of P<.05 was considered to indicate statistical significance.
Results
Study selection
The PRISMA flow chart of literature search strategies is illustrated in Figure 1. Initially, in total, 424 potential articles published until 2012 were identified from literature searches after screening all titles and abstracts; no other eligible studies were found from other sources. Overall, 57 articles were included for a full-text evaluation. Of these, 11 were excluded for not meeting the inclusion criteria. Subsequently, 46 studies were potentially included in this study. Of these, two studies, in which mixed groups of surgeries were reported and from which data could not be extracted separately, were excluded. Eight authors were contacted for additional information or to correct inaccurate information, and four provided data that were incomplete or not extractable from the original report. Finally, in total, 40 studies20–59 met our inclusion criteria and were retrieved for more detailed evaluation. The reviewers achieved perfect agreement with the eligibility criteria for all 40 studies.
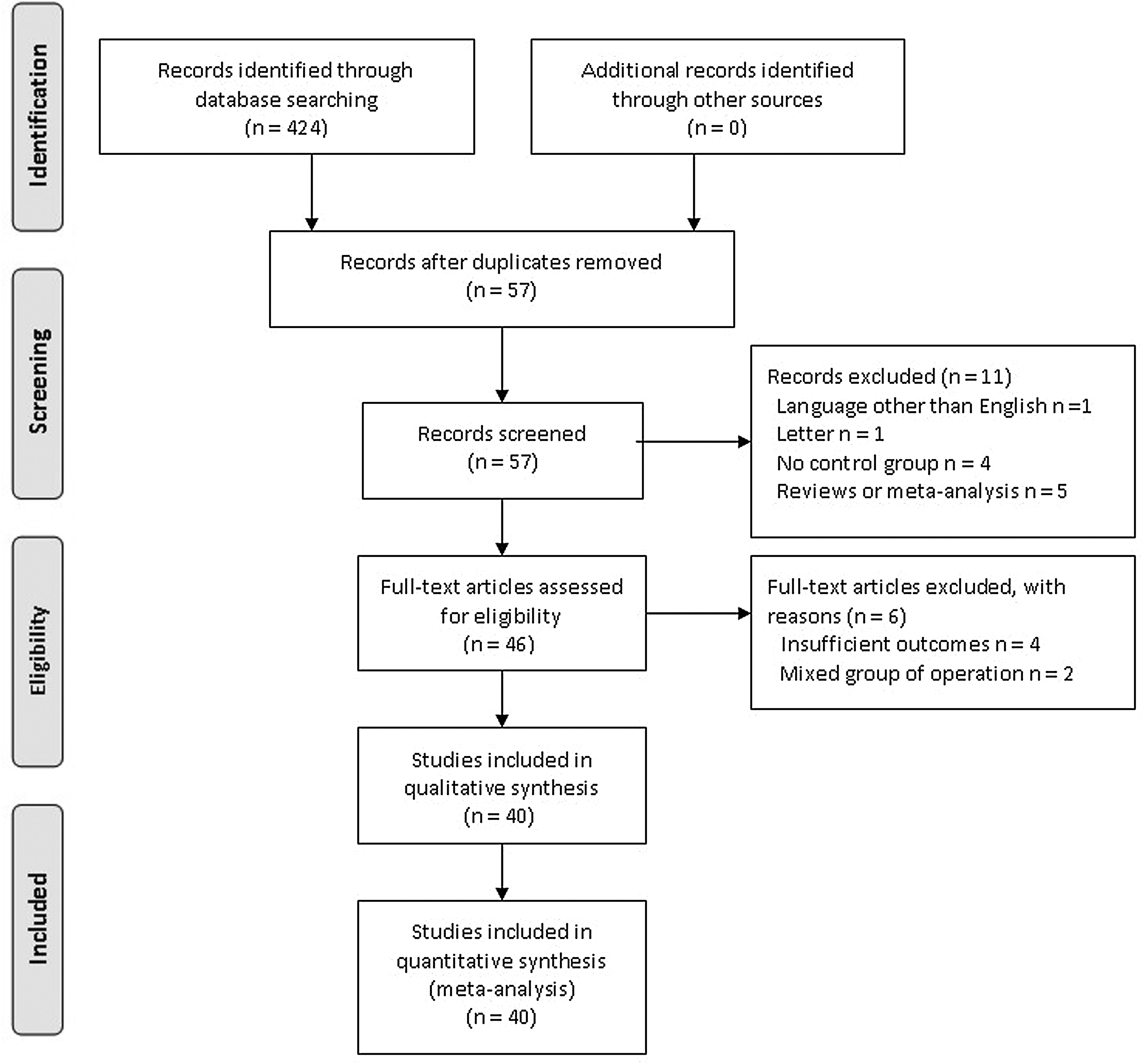
The PRISMA flowchart of literature review.
Study characteristics and methodological quality assessment
The baseline characteristics of the 40 included studies and the study design are summarized in Table 1. The sample size of these studies ranged from 34 to 315 patients. Analysis was performed on 3711 patients, of whom 1865 (50.2%) underwent SPLC and 1846 (49.8%) underwent CMLC. The quality assessment of RCTs is shown in Table 2. Twelve studies adequately fulfilled all methodological requirements and were considered to be at a low risk of bias, and the remaining trials were graded as moderate risk. The quality assessment of NRCSs is also presented in Table 1. In general, 17 studies were considered to be of high quality by achieving a score of ≥6. The results from a meta-analysis of the studies with regard to operative parameters, postoperative recovery, postoperative complications, and cosmetic results are summarized in Table 3.
1, symptomatic cholelithiasis; 2, gallbladder polyp; 3, acute cholecystitis; 4, chronic cholecystitis; 5, pancreatitis; 6, biliary dyskinesia; 7, incidental cancer; 8, cholesterolosis; 9, choledocholithiasis; 10, unknown gallbladder disease.
When studies had a quality score of ≥6, entries are given in bold type.
CMLC, conventional multiport laparoscopic cholecystectomy; NR, not reported; NRCS, nonrandomized comparative study; RCT, randomized controlled trial; SPLC, single-port laparoscopic cholecystectomy.
The level of bias was determined as follows: “Yes,” indicating a risk of bias; “Unclear,” indicating an uncertain risk of bias; and “No,” indicating no risk of bias. When articles fulfilled all methodological requirements, entries are given in bold type.
Statistically significant results are shown in bold type.
CBD, common bile duct; CI, confidence interval; HG, heterogeneity between studies; MD, weighted mean difference; OR, odds ratio; VAS, visual analog scale.
Intraoperative parameters
Thirty-two studies20–30,33,34,36–38,40–43,45,46,49–53,56,58,59 reported data on operative time that included a total of 2947 patients. The meta-analysis showed that SPLC had a longer operative time than CMLC by 16.1 minutes (95% CI, 9.93–22.26 minutes; P<.001) (Fig. 2). Although there was heterogeneity between the studies (I2=97%), no difference was found when a random-effects model was used. Estimated blood loss was reported in seven studies22,24,30,34,42,55,59 that included 569 patients. The meta-analysis showed that there was no significant difference between the two groups (MD, 0.44 mL; 95% CI, −0.96 to 1.85 mL; P=.54). Nineteen trials20,23–25,27,28,31,35,36,39,41–43,48,51,54,56,57 reported both the number of patients who required conversion to an open procedure or the addition of a port to the procedure in the SPLC group and those who required conversion to SPLC or open procedures in the CMLC group. The meta-analysis showed SPLC had a higher rate of conversion than CMLC by 4.2% (95% CI, 2.71%–6.56%; P<.001) (Fig. 3) without any heterogeneity between studies (I2=48%).
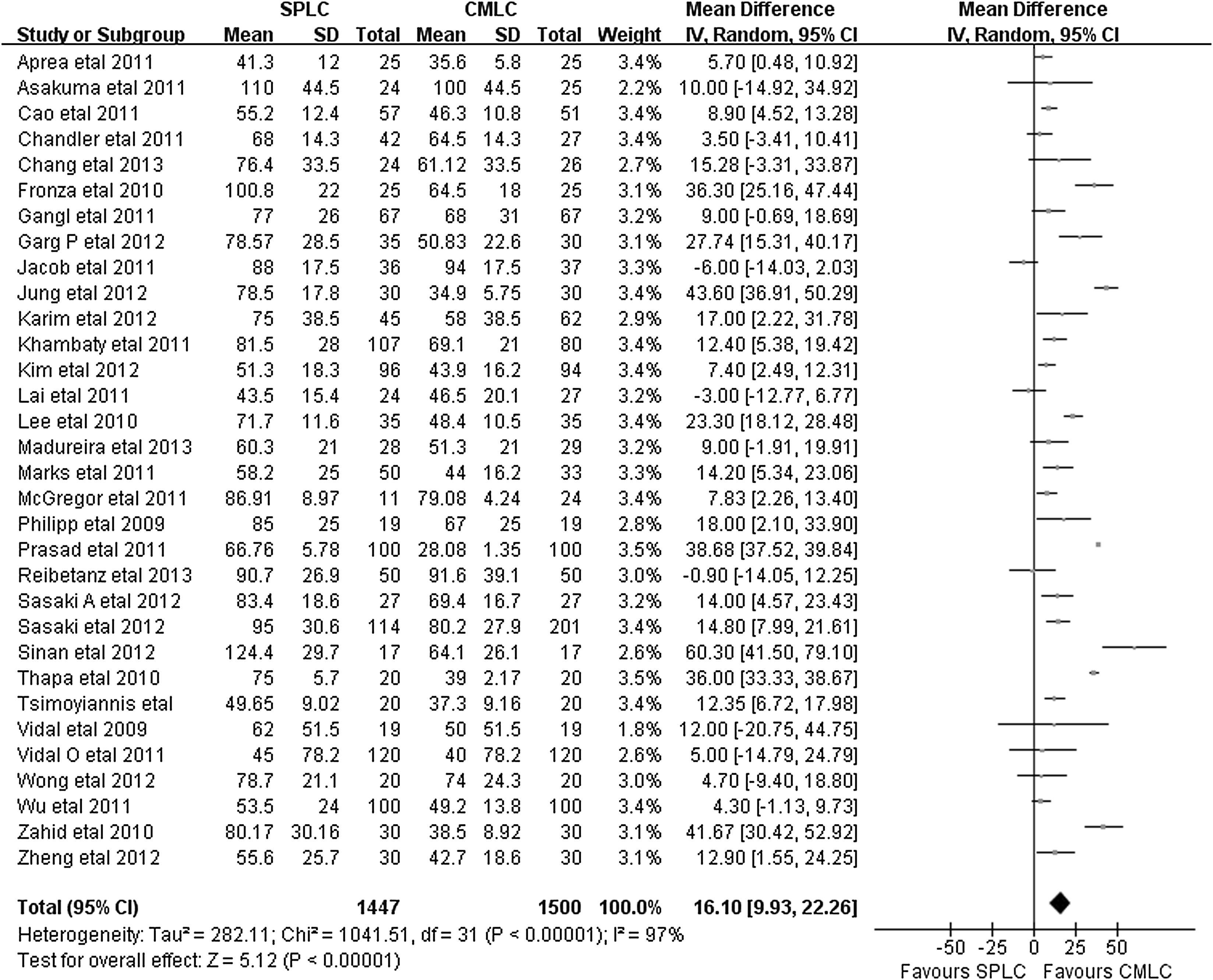
Meta-analysis for the outcome of operative time comparing single-port laparoscopic cholecystectomy (SPLC) with conventional multiport laparoscopic cholecystectomy (CMLC). CI, confidence interval; IV, inverse variance; SD, standard deviation.

Meta-analysis for the outcome of conversion rate comparing single-port laparoscopic cholecystectomy (SPLC) with conventional multiport laparoscopic cholecystectomy (CMLC). CI, confidence interval; M-H, Mantel–Haenszel.
Postoperative outcomes
A meta-analysis of 21 studies21–27,33–35,37,41,43–45,51,53,56,57,59 that included 1700 patients showed that SPLC had a negligible shorter hospital stay than CMLC by 0.16 days (95% CI, −0.28 to −0.04 days; P=.01) (Fig. 4). Although there was heterogeneity between the studies (I2=57%), no difference was found when a random-effects model was used. Five studies23,32–34,43 that included 304 patients reported the length of incision. The meta-analysis showed a 7.7-mm shorter length of wound in the SPLC compared with the CMLC group (95% CI, −14.15 to −1.25 mm; P=.02). The time taken by the individual to return to work was shorter by 0.23 days for the SPLC group, although the difference was not statistically significant (95% CI, −0.80 to 0.34 days; P=.43).
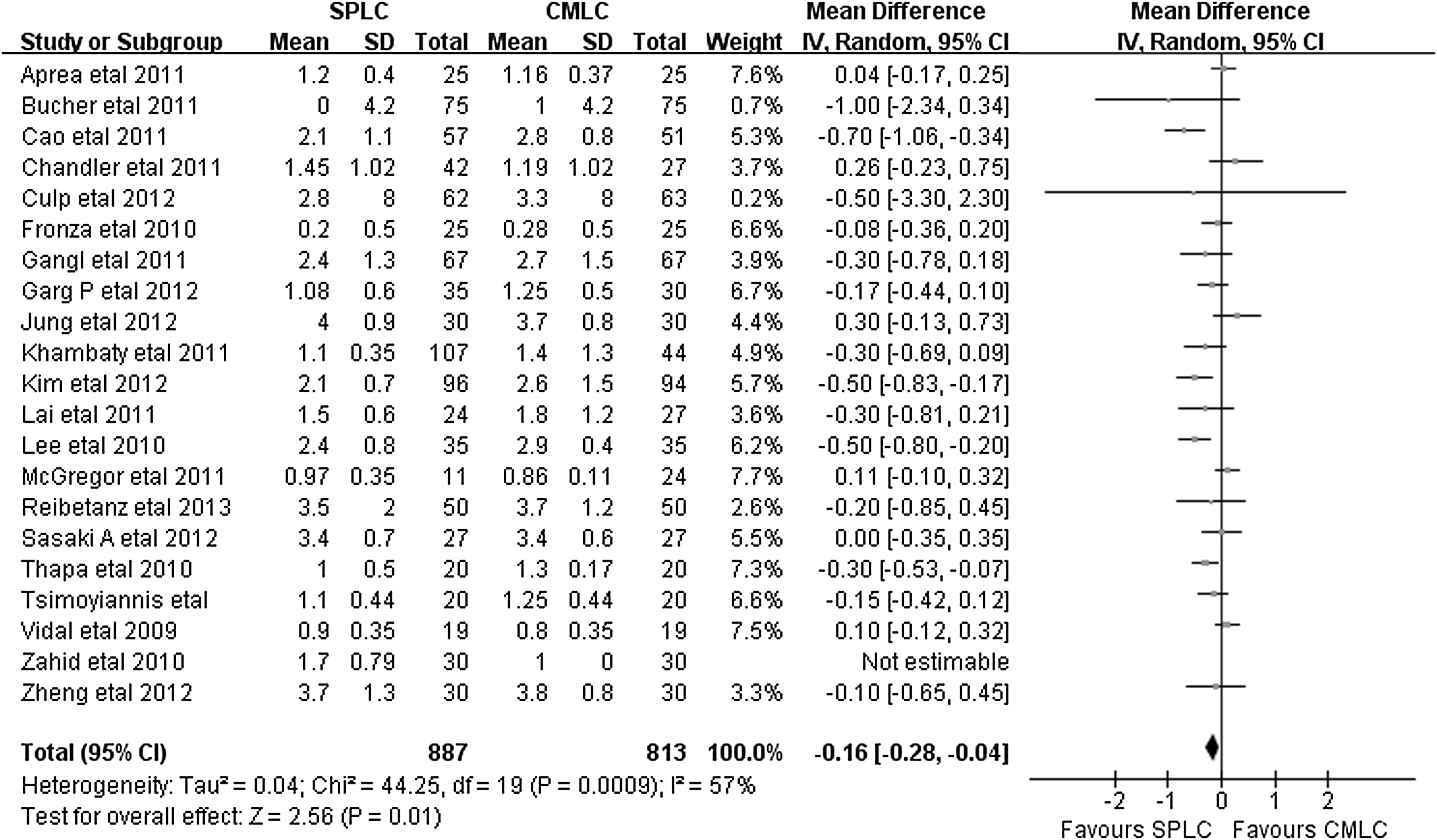
Meta-analysis for the outcome of hospital stay comparing single-port laparoscopic cholecystectomy (SPLC) with conventional multiport laparoscopic cholecystectomy (CMLC). CI, confidence interval; IV, inverse variance; SD, standard deviation.
Four studies27,35,36,51 reported the dosage of morphine used postoperatively, and pooled analysis showed that there was no significant difference between the two groups (MD, −3.78 mg; 95% CI, −13.78 to 6.22 mg; P=.46). Eight trials22,29,33,35,50,52,55,57 used the VAS score to investigate early postoperative abdominal pain at 2, 4, 6, 12, 24, and 48 hours after surgery. The meta-analysis of these data showed no significant difference in pain scores at any of the early time points between the SPLC and CMLC groups (OR, 0.1; 95% CI, −0.44 to 0.24; P=.57) (Fig. 5). Four studies22,34,51,59 reported abdominal pain scores at 48 hours and 1 week after surgery, but the meta-analysis showed that there were no significant differences between the two groups (MD, −0.13; 95% CI, −0.45 to 0.19; P=.42) (Fig. 6).
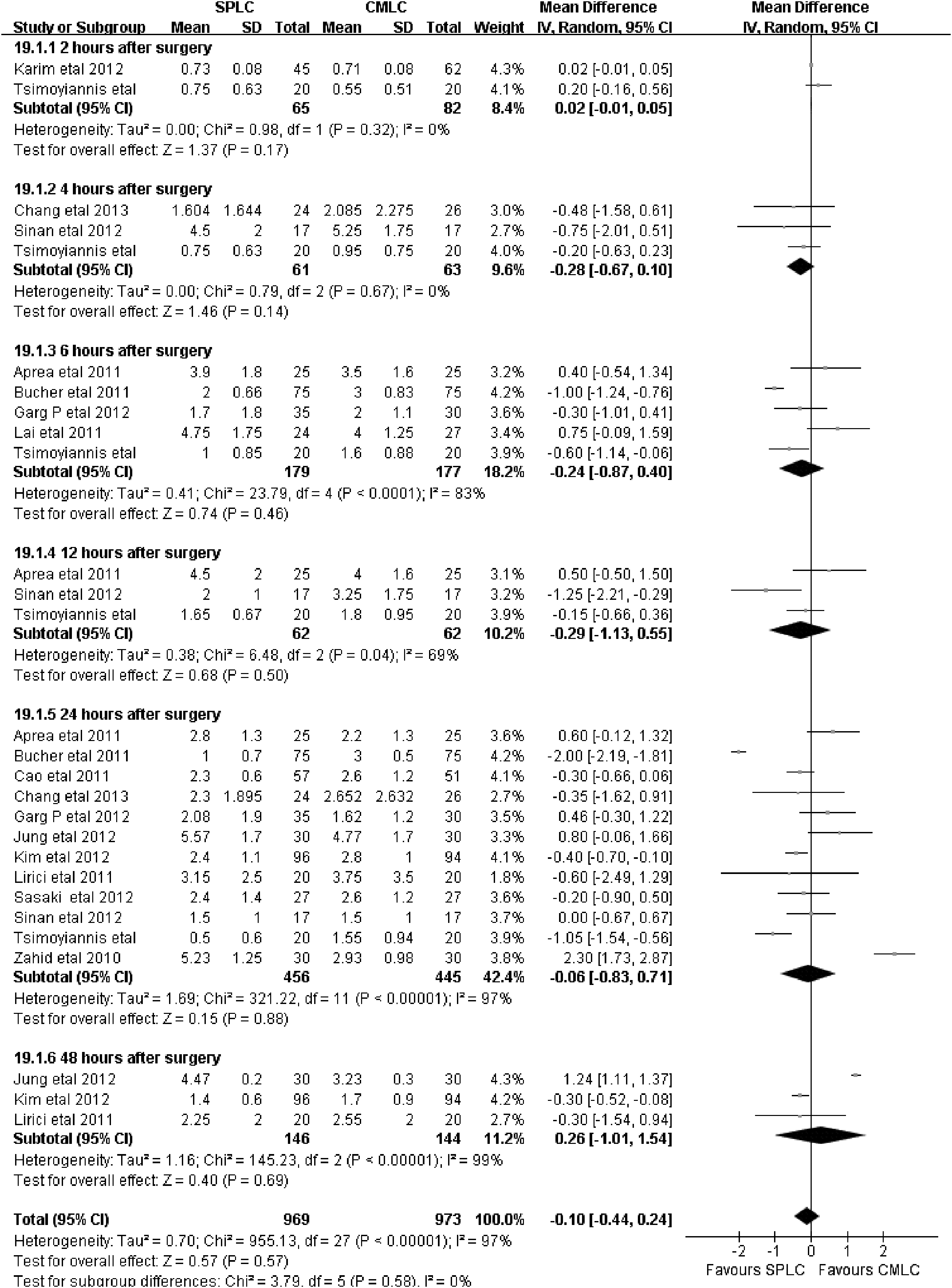
Meta-analysis for the outcome of early visual analog scale scores comparing single-port laparoscopic cholecystectomy (SPLC) with conventional multiport laparoscopic cholecystectomy (CMLC) at 2, 4, 6, 12, 24, and 48 hours after surgery. CI, confidence interval; IV, inverse variance; SD, standard deviation.

Meta-analysis for the outcome of late visual analog scale scores comparing single-port laparoscopic cholecystectomy (SPLC) with conventional multiport laparoscopic cholecystectomy (CMLC) at 72 hours and 1 week after surgery. CI, confidence interval; IV, inverse variance; SD, standard deviation.
Postoperative complications
Thirty studies20,21,23–28,30,31,33–35,37–39,42,43,45,46,49–59 that included 2857 patients reported the overall incidence of postoperative morbidity. The meta-analysis showed that the incidence of overall morbidity was 1.21% lower in the SPLC group than in the CMLC group, although this difference was not statistically significant (95% CI, 0.92–1.62; P=.18) (Fig. 7). Fifteen studies20,23,28,31,33,34,37,39,43,45,46,50,52,54,56 reported on the wound infection rates after surgery. Meta-analysis showed there was no significant difference between the SPLC and CMLC groups (OR=1.03; 95% CI, 0.53–2.0; P=.92), as were the rates of wound hematoma (OR=2.27; 95% CI, 0.9–4.73; P=.09) and incision hernia (OR=1.67; 95% CI, 0.65–4.27; P=.29). Bile duct injury rates were reported in five studies.20,23,49,56,57 According to pooled analysis, both SPLC (6 of 309) and CMLC (19 of 382, 3.1%) had similar rates of bile duct injury (OR, 0.52; 95% CI, 0.22–1.25; P=.14).
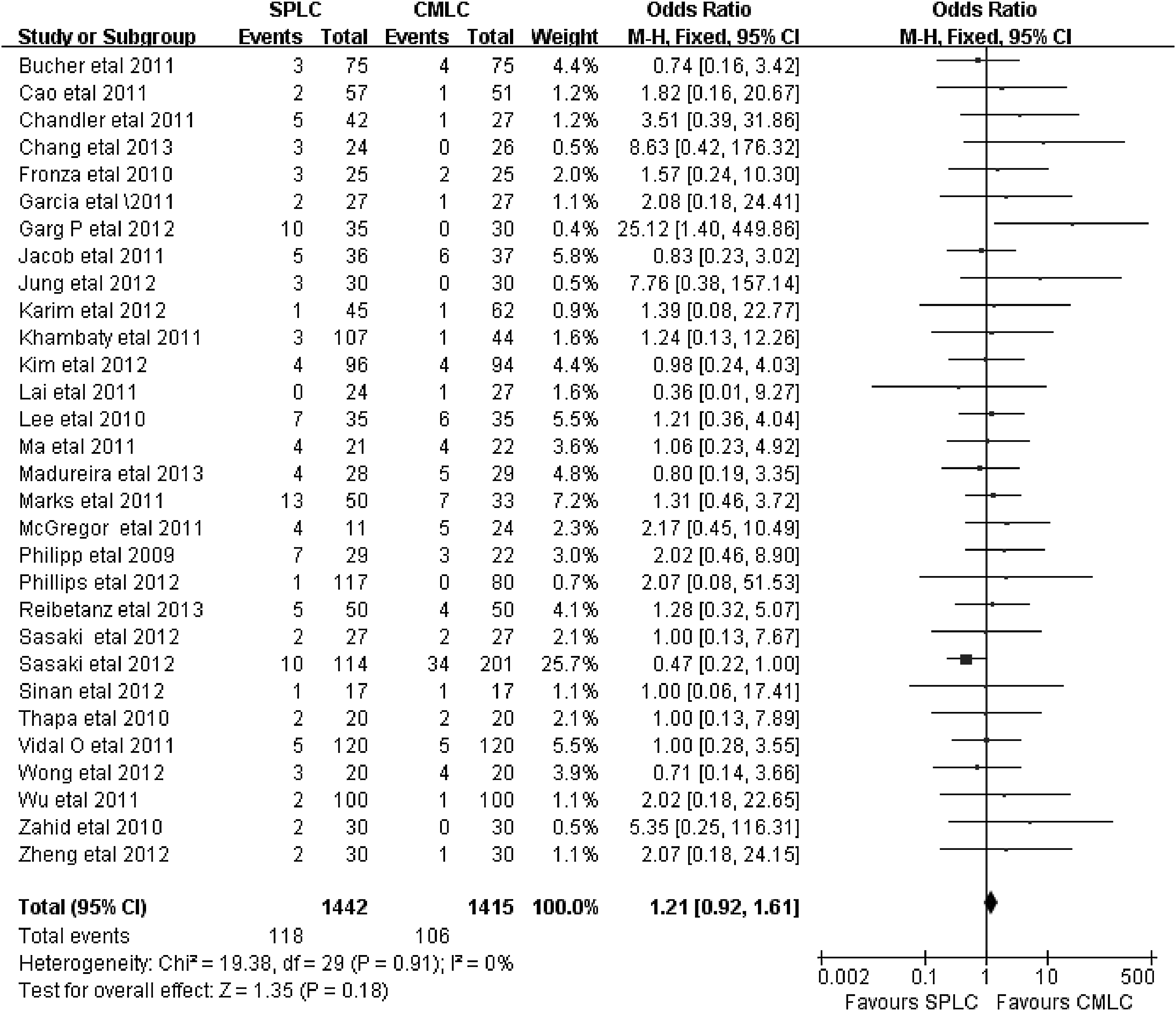
Meta-analysis for the outcome of overall complications comparing single-port laparoscopic cholecystectomy (SPLC) with conventional multiport laparoscopic cholecystectomy (CMLC). CI, confidence interval; M-H, Mantel–Haenszel.
On the basis of data available from six studies,24,28,31,34,54,59 there was no significant difference in the rate of retained common bile duct stones between the SPLC and CMLC groups (OR, 1.11; 95% CI, 0.35–3.49; P=.86). The incidence of bile leakage was measured in eight studies22,23,34,42,49,56,58,59 with 1047 participants. Meta-analysis showed there was no significant difference between the SPLC and CMLC groups (OR=1.33; 95% CI, 0.84–2.11; P=.22), as was the incidence of pneumonia (OR=0.72; 95% CI, 0.14–3.74, P=.70) from three studies.24,26,46
Cosmetic outcomes
Six studies23,30,32,47,48,58 assessed cosmetic outcomes (Fig. 8), of which only two studies45,48 reported data on the Body Image Scale questionnaire ranging from 5 (best) to 20 (worst results). Data obtained at different time points (postoperatively 1 and 2 weeks and 1, 3, and 6 months) were available for use in the pooled analysis. The meta-analysis showed that there were significant differences between the two groups for the cosmetic satisfaction score at 2 weeks (MD, −1.39; 95% CI, −2.66 to −0.12; P=.03) and at 1 month (MD, −1.3; 95% CI, −2.05 to −0.55; P=.00007) in favor of the SPLC group after surgery.
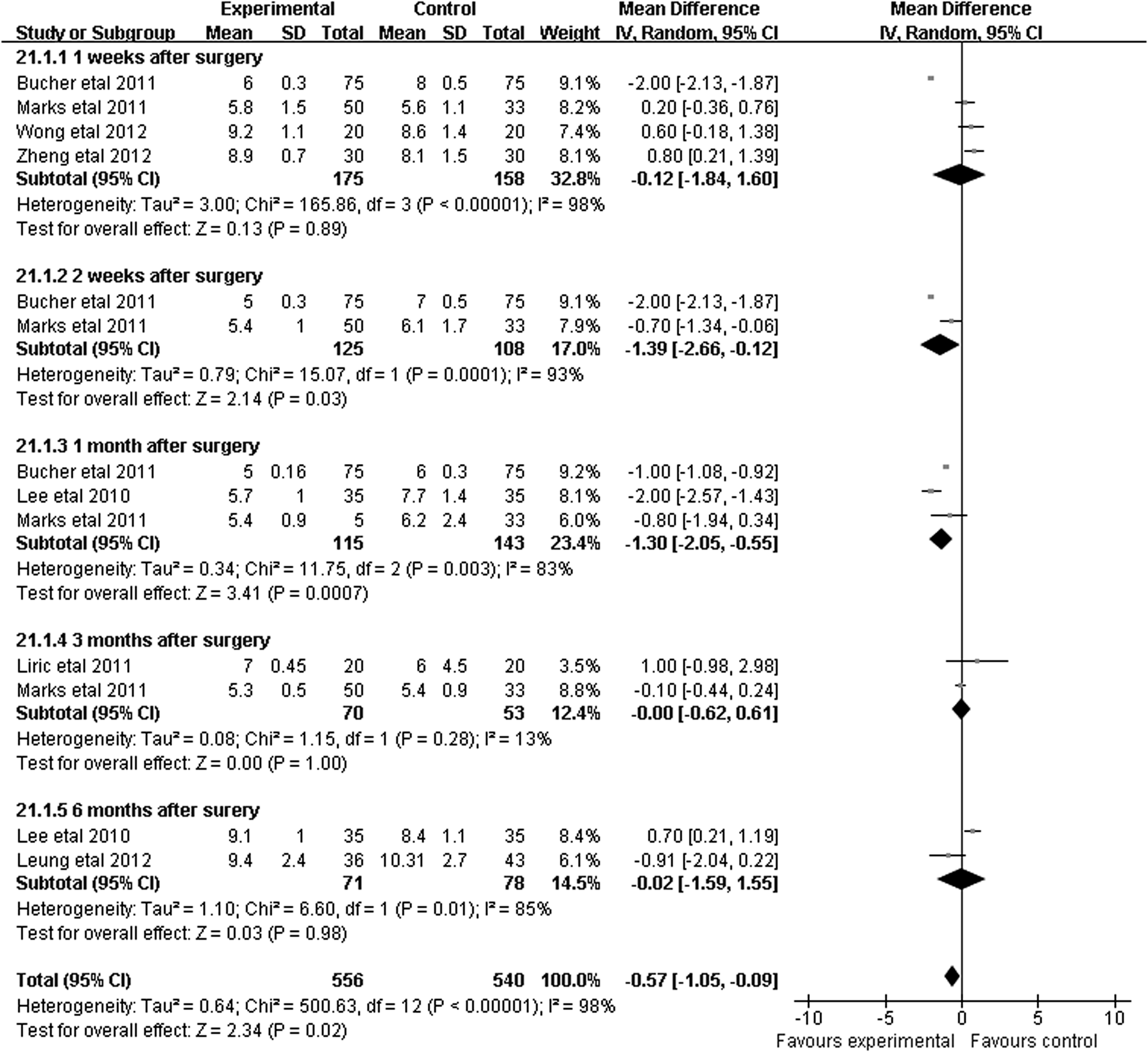
Meta-analysis for the outcome of cosmetic results comparing single-port laparoscopic cholecystectomy (SPLC) with conventional multiport laparoscopic cholecystectomy (CMLC) at 1 week, 2 weeks, 1 month, 3 months, and 6 months after surgery. CI, confidence interval; IV, inverse variance; SD, standard deviation.
QoL
Only five studies31,32,35,48,54 reported QoL outcomes. However, because of heterogeneities in items measured and the different time points used, we could not conduct the pooled analysis of the studies. Ma et al. 31 measured the QoL by the Short Form-36 questionnaire and reported no significant difference in the average follow-up after surgery between the SPLC (19.4 days) and CMLC (16.0 days) groups (P>.05). Lirici et al. 32 applied the Short Form-36 questionnaire at the 30-day follow-up to compare QoL between the SPLC and CMLC groups and found that the role emotional scale scores were significantly better in the SPLC group (80.05) than in the CMLC group (68.33) (P<.0001). Leung et al. 48 reported that the QoL was measured postoperatively at 1 week, 3 weeks, and 6 months through the self-organizing maps technique; no significant differences were found between the two groups at all time points after surgery. Furthermore, Bucher et al. 35 demonstrated that the QoL was better after SPLC than CMLC (P=.02) by means of the Short Form-12 questionnaire (Quality Metric, Lincoln, RI). Finally, Phillips et al. 54 compared SF-8™ QoL questionnaire scores between the two groups and found that the QoL scores statistically favored SPLC over CMLC at 3 days (P=.02) and at 2 weeks (P=.03) after surgery.
Sensitivity analysis
The sensitivity analysis included the following: (1) 16 RCTs; (2) 24 NRCSs; (3) 33 studies of high quality (16 RCTs and 17 NRCSs with quality score of 6 or more using the modified Newcastle-Ottawa scale); and (4) 23 studies with more than 30 patients in each group. The results from sensitivity analysis were summarized in Table 4.
Statistically significant results are shown in bold type.
CBD, common bile duct; CI, confidence interval; HG, heterogeneity between studies; MD, weighted mean difference; OR, odds ratio; VAS, visual analog scale.
RCTs
When only RCTs were analyzed, estimated blood loss became significantly higher in the CMLC group compared with the SPLC group (MD=1.70 mL; 95% CI, 0.19–3.21 mL; P=.03). The rest of the outcomes were consistent with the overall analysis, including operative time (P<.0001), hospital stay (P=.01), conversion rates (P<.0001), overall complications (P=.08), and early (P=.13) or late (P=.08) VAS pain score. There was generally a reduction in the degree of heterogeneity.
NRCSs
Twenty-four NRCSs compared the operative, postoperative outcome, and complications between the SPLC and CMLC procedures. Difference in hospital stay became nonsignificant between groups (MD=0.09 days; 95% CI, −0.25 to 0.07 days; P=.27). Operative time remained significantly higher in the SPLC group by 16.14 minutes (P<.0001). The blood loss became significantly less in the SPLC group compared with the CMLC group (MD=–7.78 mL; 95% CI, −11.65 to −3.91 mL; P<.0001). The other variables remained similar to the original SPLC versus CMLC analysis. Heterogeneity was once again reduced.
High-quality studies (scores of >6 and RCTs)
The outcomes showed similar results as the original analysis. Heterogeneity was once again reduced.
Sample size (studies with more than 30 patients in each group)
There were 23 studies with more than 30 patients in each SPLC and CMLC group. Time return to work became significantly shorter in the SPLC group than CMLC group (MD=0.84 days; 95% CI, −1.6 to −0.09 days; P=.03). The remaining results were similar to the original analysis, and heterogeneity was once again reduced.
Publication bias
The funnel plot of this study based on postoperative overall complications is shown in Figure 9. All studies except two lay inside the limits of the 95% CIs and distributed more evenly about the vertical, showing no evidence of publication bias.
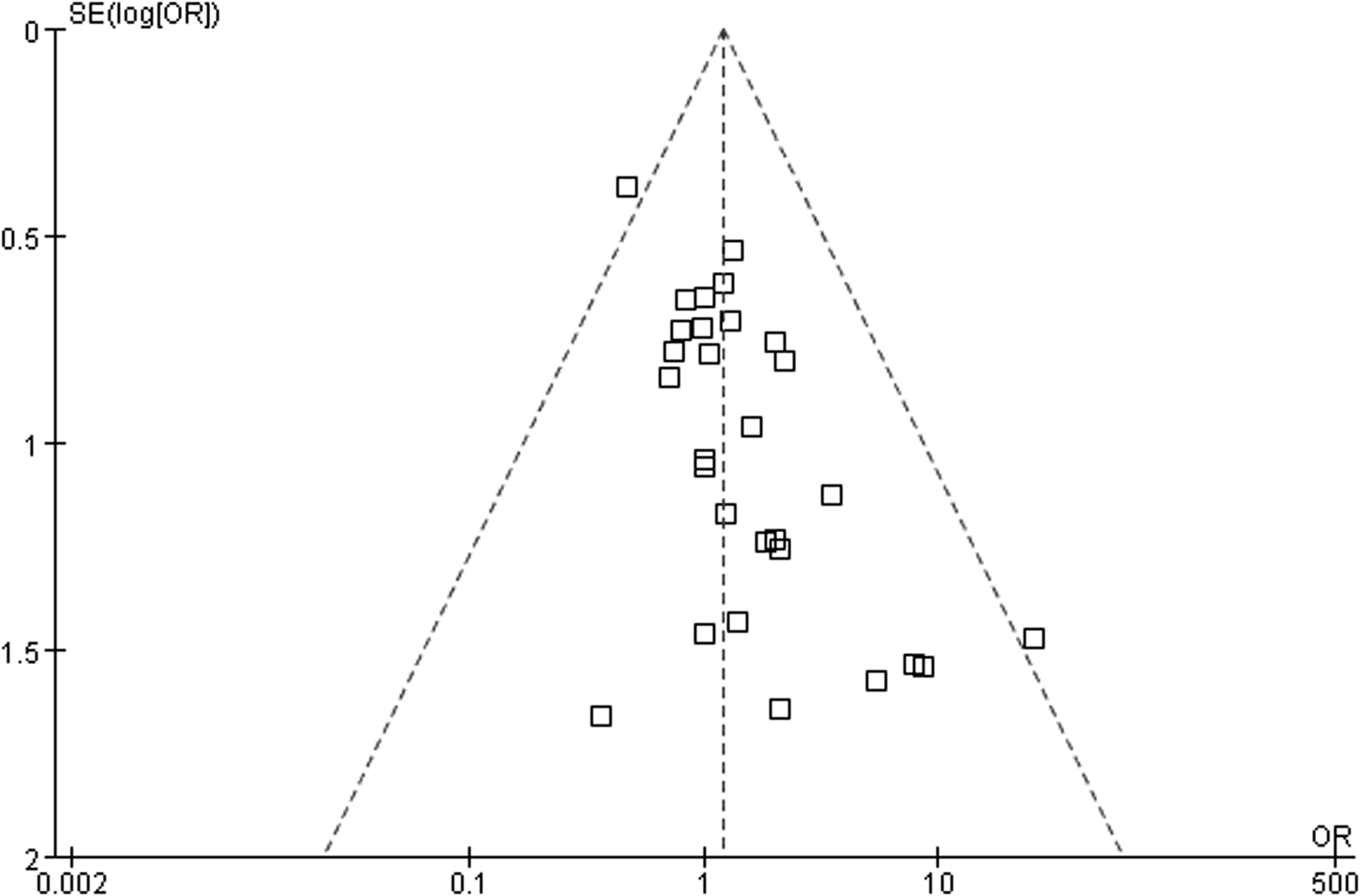
Funnel plot of overall complications in included studies, showing no publication bias. OR, odds ratio; SE, standard error.
Discussion
During the past few years, the evolution of minimally invasive approaches represents one of the most significant advances in the field of general surgery. The laparoscopic approach has been associated with a reduction in postoperative pain, fewer complications, faster recovery, and shorter hospital stay compared with the open counterpart.60,61 Laparoscopic removal of a gallbladder through a single periumbilical skin incision was first performed in 1997 by Navarra et al. 62 Several meta-analyses have been published and have reported satisfactory outcomes based on the feasibility and safety of SPLC compared with CMLC. However, these previous meta-analyses may have been limited by the small sample sizes and methodological defects,8–12 which were not sufficient for evaluation of this novel surgical intervention.
This study summarizes the largest available dataset for comparison between SPLC and CMLC. The results demonstrated that SPLC was associated with longer operative time and higher conversion rates but shorter hospital stay and better cosmetic outcomes than those with CMLC. Postoperative VAS pain scores and overall or specific complications were comparable between the two groups. The findings from sensitivity and subgroup analysis of either RCTs or high-quality NRCSs are consistent with the overall analysis, implying the credibility of our results. Our results concurred with the majority of the outcomes from previous meta-analyses and highlight the obvious advantages of SPLC.
SPLC is a challenging technique for both surgeons and the surgical team; however, it can be performed safely by experienced laparoscopic surgeons, with results that are comparable to those of CMLC. There are several disadvantages of this novel procedure. First, one obvious disadvantage of SPLC is that it requires a longer operative time than CMLC because of loss of triangulation and poor handling due to interference of devices at the same skin incision. 49 Body mass index is another factor that may prolong the operative time.30,51 Even though a surgeon's initial cases using SPLC might require longer operative times, the experience attained can shorten this in future cases. In the current study, the operative times between the two groups were statistically different; the mean operative time in the SPLC group was 16.1 minutes longer than that of the CMLC group.
Second, the SPLC procedure is associated with a high risk of technique failure. The rate of SPLC conversion to CMLC or an open procedure was documented in 19 studies and ranged from 0% to 51.7%, mainly because of the inability to adequately expose the anatomical structures, 41 severe adhesions, 49 and technical difficulties. 31
Third, postoperative incisional hernia is another disadvantage of SPLC. To prevent an incisional umbilical hernia, the incision must be carefully closed. In general, removal of the gallbladder is easier by SPLC than by CMLC. Wang et al. 11 reported that the incidence of incisional hernia in an SPLC group was obviously higher than that in a CMLC group. Contradictory results were found in studies performed by Sajid et al., 10 Markar et al., 9 and Trastulli et al. 8 This systematic review and meta-analysis demonstrated that there was no significant difference in surgical site hernias between the two groups by pooled analysis.
Finally, although experience is essential to avoid increased rates of morbidity in any surgical procedure, the effect of the learning curve in SPLC does not seem to be the most important factor in minimizing the possibility of iatrogenic bile duct injuries because most are related to anatomical misdiagnoses and lapses from the basic principles of biliary surgery. 63 Recently, a world review published by Joseph et al. 64 reported that there was an increase in the bile duct injury rates during the SPLC procedure compared with historical rates during the CMLC procedure. However, in the current study, there was no significant difference between the two groups by pooled analysis.
This meta-analysis has several limitations that must be taken into account. First, the strengths and limitations of meta-analytical techniques have been a source of considerable debate. Supporters of these techniques argue that meta-analyses are excellent tools for identifying the causes of variability and inconsistencies between studies; however, some detractors of this technique argue that meta-analyses reinforce inherent systematic biases in studies and produce spurious statistical stability, thereby discouraging further research. 65 Second, heterogeneity may influence the precision of overall effect sizes or may exaggerate the overall effect sizes in some outcome measures, even if the random model was used. The sample size of this study was not large enough to distinguish the differences in outcome measures of bile duct injury and QoL between the SPLC and CMLC groups. Third, the types of techniques and instruments used in SPLC, such as conventional, articulating, and flexible or articulating, vary among different studies. The pooled analysis outcome may be inaccurate because of the various instruments used; however, we could not obtain enough information to further evaluate these instruments separately. Finally, most important parameters, such as cosmetic satisfaction results, were found to be greater in patients who had undergone SPLC, but these results should be considered with caution because the analyses included only eight trials, and the results require confirmation in further high-quality randomized trials.
In conclusion, this study showed that SPLC is a safe alternative to CMLC. Although SPLC may be associated with longer operative times and higher conversion rates, patients who undergo SPLC may benefit from shorter hospital stays and better cosmetic outcomes. To strengthen the clinical evidence, more high-quality clinical trials examining different factors are necessary.
Footnotes
Acknowledgments
We would like to thank the staff and colleagues in the Chinese Cochrane Centre for their help and support. This study was supported by the Science and Technology Support Project of Sichuan Province (grant 2009FC0093) and the Natural Science Foundation of China (grants 81200551 and 81270841).
Author Contributions
H.W. and J.Q. designed the study. J.Q. and H.Y. conducted the majority of the study and wrote the manuscript. S.C. and Z.H. edited the manuscript. P.H. offered suggestions for this work.
Disclosure Statement
No competing financial interests exist.