
Abstract
Abstract
Background:
Ultrasonic surgery can dissect structures and divide vessels by the effect produced by vibrations in the tissues. It is believed to be less traumatic than the more commonly used monopolar electrosurgery (ELC). Laparoscopic techniques are being used increasingly in surgical conditions complicated by peritonitis. This randomized study compares the acute inflammatory and systemic immune response after laparoscopic cholecystectomy in patients with acute calculous cholecystitis, complicated by peritonitis, performed using either ultrasonic energy or ELC.
Patients and Methods:
Forty-three patients, scheduled for laparoscopic cholecystectomy, were randomly assigned to treatment using either an ultrasonic device (UC) (n=22 patients) or ELC (n=21 patients). Bacteremia, endotoxemia, white blood cells, the peripheral lymphocyte subpopulation, human leukocyte antigen-DR (HLA-DR), neutrophil-elastase, interleukin-6 and -1, and C-reactive protein (CRP) were investigated.
Results:
Significantly higher concentration of systemic endotoxin, neutrophil, neutrophil-elastase, interleukin-6 and -1, and CRP were detected intraoperatively and/or postoperatively in the ELC group of patients in comparison with the UC group (P<.05). A statistically significant change in HLA-DR expression was recorded on postoperative Day 1 as a reduction of this antigen expressed on the monocyte surface in patients from the ELC group; no changes were noted in UC patients (P<.05). We recorded 4 patients (22.2%) who developed an intraabdominal abscess in the ELC group and 1 (4%) in the UC group (P<.05).
Conclusions:
Laparoscopic cholecystectomy after biliary peritonitis, conducted by ELC, increased the incidence of bacteremia and systemic inflammation compared with the UC group. Early enhanced postoperative systemic inflammation may cause lower transient immunologic defense in the ELC group, leading to enhanced sepsis.
Introduction
S
Several studies have evaluated blood cells, cytokines, cortisol, catecholamines, acute-phase proteins, and cell-mediated immunity to try to quantify and compare the inflammatory and immunologic changes after laparoscopic and open cholecystectomy.3–10 These researchers also observed that serum markers of tissue trauma were significantly higher in the laparotomy group.3–10 One study showed no differences between laparoscopic and “mini” open cholecystectomy. 11
Ultrasonic surgery can dissect structures and divide vessels by the effect produced by vibrations in the tissues. It is believed to be less traumatic than the more commonly used monopolar electrosurgery (ELC).
Minimal heat production in the Harmonic® (Ethicon Endo-Surgery, Blue Ash, OH) scalpel leads to a minimal zone of thermal injury and better healing compared with electrosurgery and lasers. 12 Holub et al. 13 reported that the histopathology laboratory had also found less tissue damage in the uterus and round ligament when the ultrasonically activated scalpel was compared with electrosurgery. Moreover, the advantage of the ultrasonic technique 13 included less charring and plume, better visualization, and fewer thermal injuries, particularly with respect to the important surrounding pelvic structures. Electrosurgery was demonstrated to be superior to the Harmonic scalpel in cases of larger fibromas as well as better in terms of cost-effectiveness.
One randomized study compared the systemic immune response after laparoscopic cholecystectomy performed using either ultrasonic energy or ELC. 14 The authors concluded that the Harmonic scalpel and ELC are equally traumatic in terms of activation of the systemic immune response. 14
Laparoscopic techniques are being used increasingly in surgical conditions complicated by diffuse or localized peritonitis. It is important to note that in the literature there are no studies on stress response after laparoscopic cholecystectomy by ultrasonic versus electrocautery dissection for acute calculous cholecystitis, complicated by biliary peritonitis.
For this reason we decided to compare, in a prospective, randomized study, the acute inflammatory reaction and immune response to the Harmonic scalpel and electrosurgery in laparoscopic cholecystectomy in patients with acute calculous cholecystitis, complicated by peritonitis.
Patients and Methods
From May 2005 to May 2012, we studied, in a prospective randomized study, 43 patients consecutively (26 women, 17 men; mean age, 58 years), who showed intraoperatively biliary peritonitis with acute calculous cholecystitis. Bile peritonitis is an inflammatory, irritative response to the abnormal presence of bile and bacteria in the peritoneal cavity. 15 These patients were a subset from a larger number of 618 patients who were admitted presenting similar preoperative findings: acute upper abdominal pain with tenderness and involuntary guarding under the right hypochondrium and/or into the flank; temperature of >38°C, leukocytosis of >10×109/L, or both; and ultrasonographic evidence (thickened gallbladder wall, edematous gallbladder wall, presence of gallstones, ultrasonographic Murphy's sign, and pericholecystis and/or Douglas space fluid collection). Three patients had hypotension. These diagnostic criteria suggest acute calculous cholecystitis eventually complicated by peritonitis. According to a computer-generated table of random numbers, all patients were randomly divided into two groups (Table 1): in the first group the dissection was conducted by ELC; in the second group the dissection was conducted by an ultrasonic device (UC) (ultrasonically activated shears). Randomization was performed by an independent computer consultant. Both the patient and the surgeon were informed about the kind of approach just before the intervention.
Data are mean values (range) except as indicated.
Three patients (7%) were converted to open surgery.
One patient (4%) was converted to open surgery.
P<.05 (by Student's t test).
ASA, American Society of Anesthesiologists; ELC, monopolar electrosurgery; F, female; M, male; UC, ultrasonic device.
The diagnosis of biliary peritonitis was confirmed intraoperatively in 43 patients (6.9%): 28 patients had rupture of the gallbladder, 13 had a gangrenous gallbladder, and 2 had biliary peritonitis without perforation.
Criteria for exclusion were as follows: acute cholangitis or other acute inflammation; current or recent (6 months) acute pancreatitis; hematologic disorder; anticoagulant treatment; current or recent (6 months) thromboembolic disorders; renal, hepatic, rheumatic, or vascular disease; pregnancy; recent (6 months) surgery; or current or recent (3 years) malignancy. We also excluded patients taking corticosteroid drugs or other drugs that may affect their immunological responses. Selected patients (n=21) with clinical suspicion of common bile duct stones were subjected to preoperative endoscopic retrograde cholangiopancreatography. When common bile duct stones were discovered (15 cases), endoscopic sphincterotomy was performed, and ductal clearance achieved before operation. All 21 of these patients were excluded from the study. Therefore there were no indications for intraoperative cholangiography in either group.
During the study period, the ultrasound generator used was the Ultracision® (Ethicon Endo-Surgery), and the electrodissector used was the Erbotom ICC 350 (ERBE Elektromedizin GmbH, Tübingen, Germany). The laparoscopic cholecystectomy has been performed using the standard technique with four-trocar incisions and 14 mm Hg CO2 pneumoperitoneum.
All procedures were performed by surgeons experienced in hepatobiliary surgery and laparoscopic advanced surgery (co-authors G.A. and F.C.).
Peritoneal lavage was performed with at least 4 L of warm normal saline or until the aspirate appeared clear.
The study protocol was approved by the Ethics Committee of the Faculty of Medicine of the University of L'Aquila, and informed consent was obtained from every patient. The patients were classified as Grade I or II, according to the American Society of Anesthesiologists (ASA) grading system. 16
The initial supportive treatment during the acute phase was the same for both groups of patients. All patients received intravenous fluid infusion, intravenous antibiotics (cefotaxime, 2 g every 8 hours; tobramycin, 100 mg every 12 hours), a proton pump inhibitor (omeprazole, 40 mg i.v. every 24 hours), and, for pain relief, ketorolac tromethamine (30 mg i.m. every 6 hours). There were no indications for blood transfusion.
Anesthesia was induced in both groups using the same procedure. Pre-anesthesia was accomplished using atropine (0.01 mg/kg) plus promethazine (0.5 mg/kg). Anesthesia induction was done using sodium thiopental (5 mg/kg) and atracurium (0.5 mg/kg). Tracheal intubation and assisted ventilation were done using nitrogen dioxide/oxygen 2:1. After intubation, anesthesia was maintained with oxygen in air, sevoflurane, and remifentanil (0.25 μg/kg/minute).
Laparoscopic cholecystectomy was performed as soon as possible, within 12 hours of admission. Four patients (10%) were converted to open surgery. These patients were excluded from the study. As shown in Table 1, age, sex, ASA grade, and hospitalization were comparable in the two groups, but the intervals for anesthesia and operation were significantly shorter in the UC group (P<.05).
Blood samples were collected from all patients before operation and at Days 1, 3, and 6 after operation. Serum concentrations of interleukin (IL)-1 and IL-6 were measured at 0, 30, 60, 90, 120, and 180 minutes, at 4, 6, 12, and 24 hours, and then daily (8 a.m.) until postoperative Day 6.
To determine the severity of peritoneal contamination, undiluted peritoneal fluid was aspirated from the Douglas space at surgery for quantitative bacterial and endotoxin assays. Furthermore, an immediate bacterial assay was performed.
All samples were tested for total white blood cell (WBC) count, WBC population (neutrophils and total lymphocytes), T-helper lymphocytes (CD4), T-suppressor lymphocytes (CD8), natural killer lymphocytes (CD16 and CD56), pan B cell antigen (CD20), T-cell receptor gamma/delta, and the T-helper/T-suppressor ratio (CD4/CD8).
Human leukocyte antigen-DR (HLA-DR) of peripheral monocytes was measured by a cytofluorimetric method. The elastase concentration was measured with the method of Hafner et al. 17 C-reactive protein (CRP), IL-1, and IL-6 were measured with enzyme-linked immunosorbent assay tests.
Statistical analysis
A statistical analysis was performed using Student's t test, and P values of <.05 were considered to be significant. The values were expressed as the mean and standard deviation. Areas under the curves in two groups were compared using the Mann–Whitney U test. The magnitude of changes in each metabolic variable (areas under the curve) was compared by Pearson's correlation coefficient (r). An α Bonferroni–Holm adjustment was applied when appropriate.
Results
There was no difference in patients' mean age and sex between the two groups.
Postoperative hospitalization was comparable in the two groups, but intervals for anesthesia and operation were shorter for the UC group (P<.05) (Table 1). There was also no difference between the two groups of patients in terms of preoperative clinical (severity and duration of symptoms), biochemical (WBC count), and radiological (ultrasound) features of acute cholecystitis.
The two groups were comparable in the severity of peritoneal contamination as indicated by the viable bacterial count (ELC group, 96% of cultures positive; UC group, 92%) and endotoxin level (ELC group, 36.52±7.18 pg/mL; UC group, 38.16±8.66 pg/mL).
We recorded 1 patient (4%) who developed an intraabdominal abscess in the UC group (ASA 2) and 4 (22.2%) in the ELC group (ASA 1, 1 patients; ASA 2, 3 patients) (P<.05) (Table 1). Clinical and ultrasonographic findings demonstrated subphrenic abscess in all cases. Expression of the monocyte antigen HLA-DR, which was low 1 day after the operation, remained low even 5 days postoperatively; it normalized 8 days after the operation. In patients number 2 and number 5, HLA-DR normalized 11 days after operation.
Severe leukocytosis (range, 14,600–18,100/mL) was observed only in the ELC group but not in the UC group, mostly due to an increment of neutrophils (Fig. 1) on Days 1 and 3 (P<.05). This value returned to the normal range within 2–3 days in the UC group and 4–6 days in the ELC group. Other WBC types showed no significant variation. Concerning the lymphocyte subpopulations, there were no differences between the two groups of patients before and after the operation.
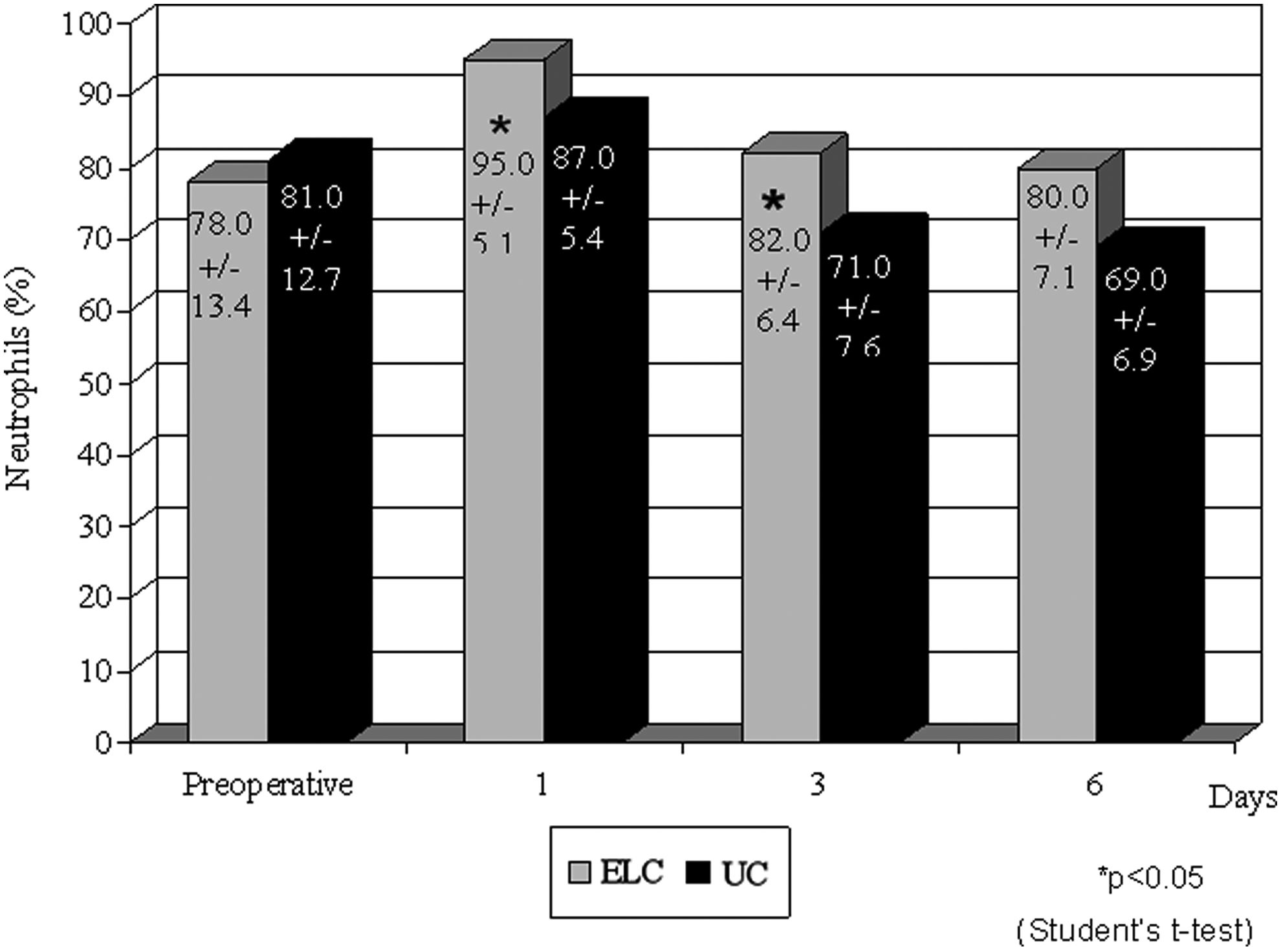
Neutrophil concentration in the monopolar electrosurgery (ELC) and ultrasonic device (UC) groups. Data are mean±standard deviation values. *P<.05 for Days 1 and 3 by Student's t test.
A statistically significant change in HLA-DR expression was recorded on postoperative Day 1 as a reduction of this antigen expressed on the monocyte surface in patients from the ELC group; no changes were noted in UC patients (Fig. 2) (P<.05). In this case HLA-DR expression returned to normal values within 6 days after the operation. Finally, the ages of the patients did not affect HLA-DR expression in either group.
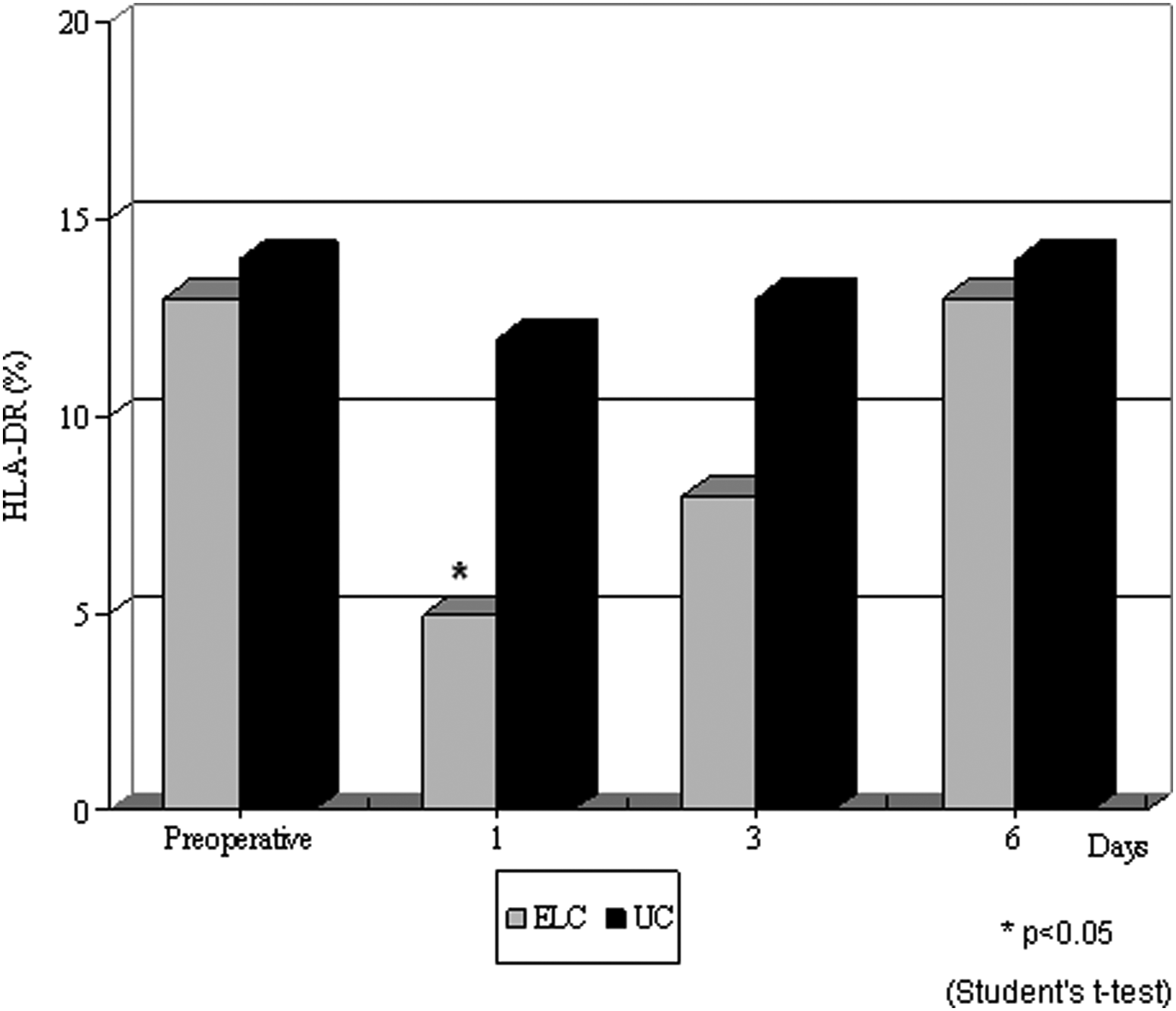
Human leukocyte antigen-DR (HLA-DR) expression in the monopolar electrosurgery (ELC) and ultrasonic device (UC) groups. Data are mean±standard deviation values. *P<.05 for Day 1 by Student's t test.
A statistically significant change in plasma elastase concentration was recorded postoperatively on Days 1, 3, and 6 as an increase in the level of this neutral proteinase from the ELC group compared with the UC group (Fig. 3) (P<.05). In the ELC group the plasma elastase concentration returned to normal values within 12 days after the operation. Finally, the ages of patients did not affect the neutrophil elastase concentration in either group.
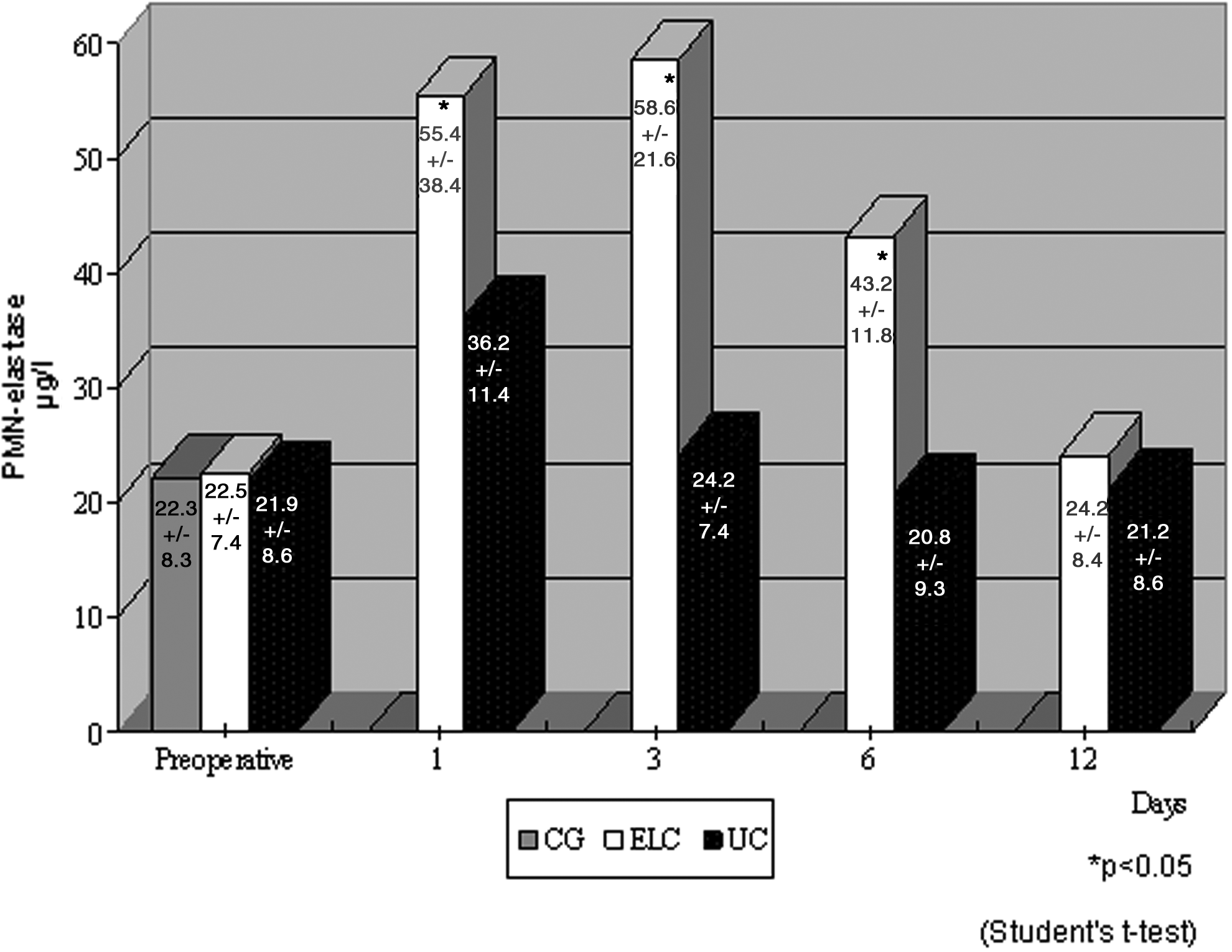
Plasma (polymorphonuclear [PMN]) elastase concentration in the control group (CG) and the monopolar electrosurgery (ELC) and ultrasonic device (UC) groups. Data are mean±standard deviation values. *P<.05 for Days 1, 3, and 6 by Student's t test.
Before the operation, serum levels of IL-1 and IL-6 were not significantly different between the two groups. Figures 4 and 5 show the chronological change in serum levels of IL-1 and IL-6, respectively, after surgery. In the ELC group, serum IL-1 and IL-6 levels began to significantly increase as early as 1 hour after the beginning of the operation, revealing a peak at the sixth hour (approximately 4 hours after the operation) and, thereafter, declining to preoperative levels by 6 days. On the other hand, in the UC group patients, the increase in serum IL-1 and IL-6 levels was delayed, and the peak values were significantly lower than those in the ELC group (r>0.75, P<.05).
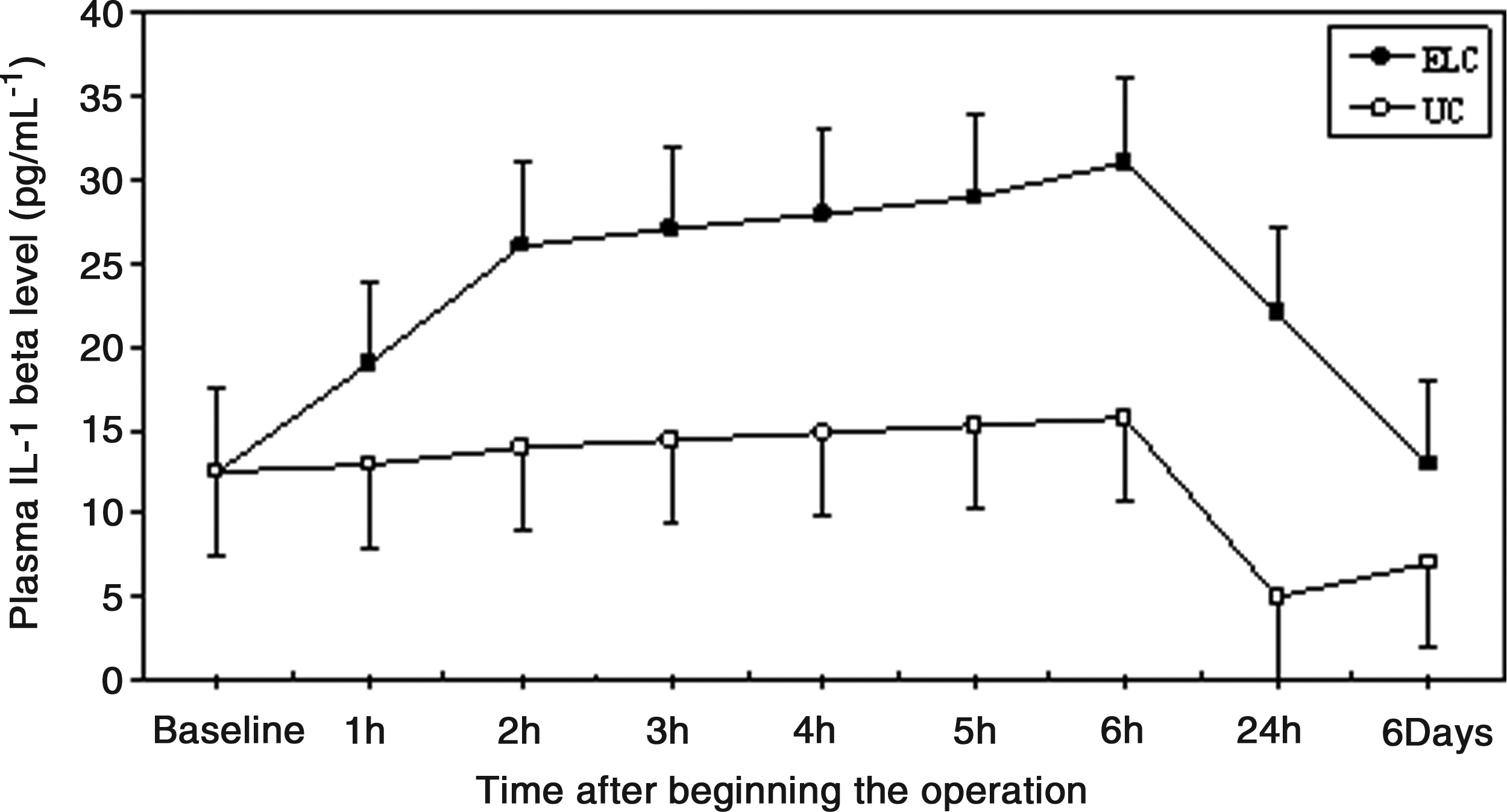
Plasma interleukin (IL)-1β in the monopolar electrosurgery (ELC) and ultrasonic device (UC) groups. There were significant differences between the two groups: r>0.75, P<.05 (by Mann–Whitney U tests and Pearson's correlation coefficient).
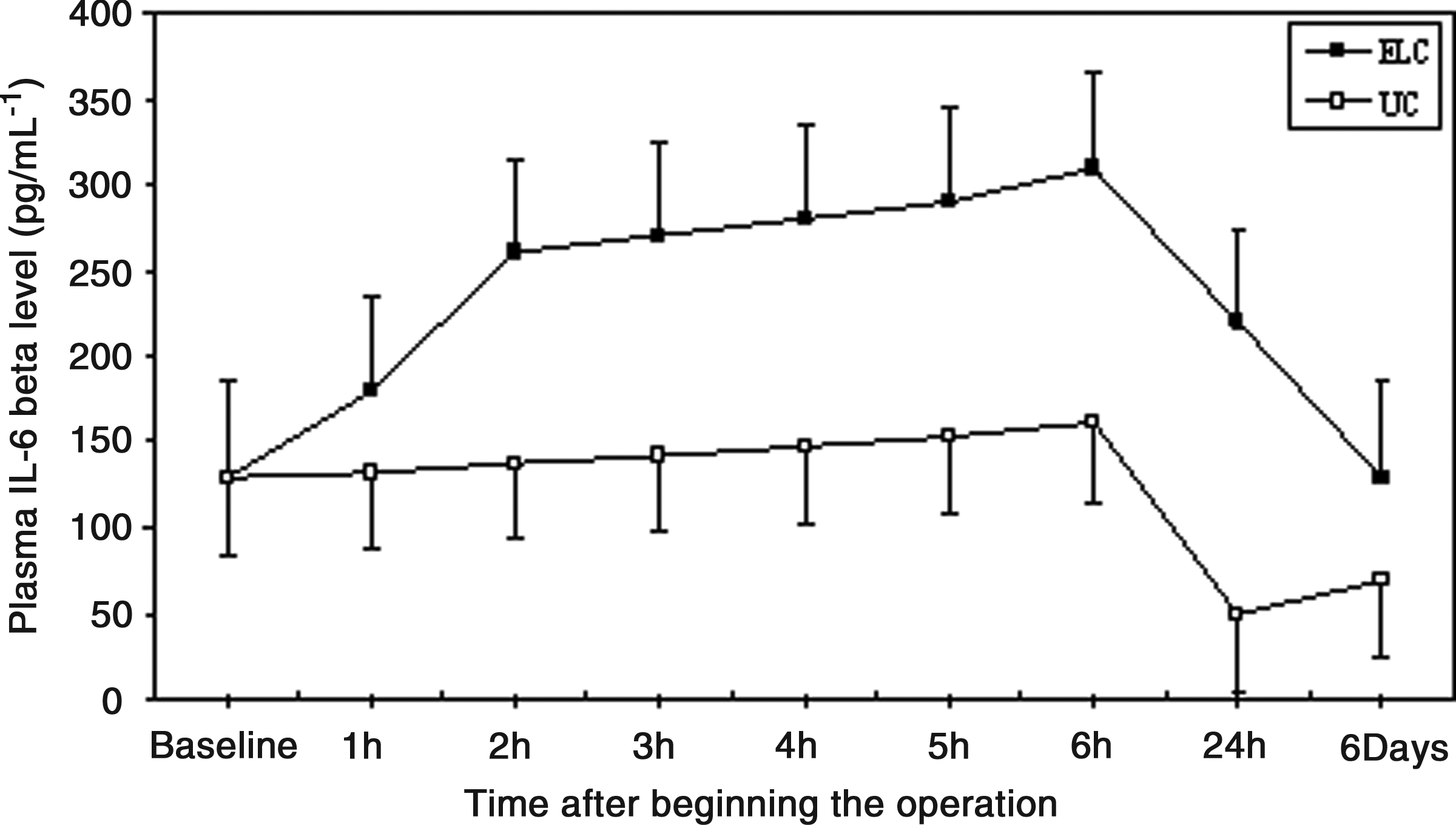
Plasma interleukin (IL)-6β levels in the monopolar electrosurgery (ELC) and ultrasonic device (UC) groups. There were significant differences between the two groups: r>0.75, P<.05 (by Mann–Whitney U tests and Pearson's correlation coefficient).
The mean values of serum CRP on postoperative Days 1 and 3 were also lower in the UC group than in the ELC group (r>0.69, P<.05) (Fig. 6). In this case the CRP concentration returned to normal values within 6 days after the operation.
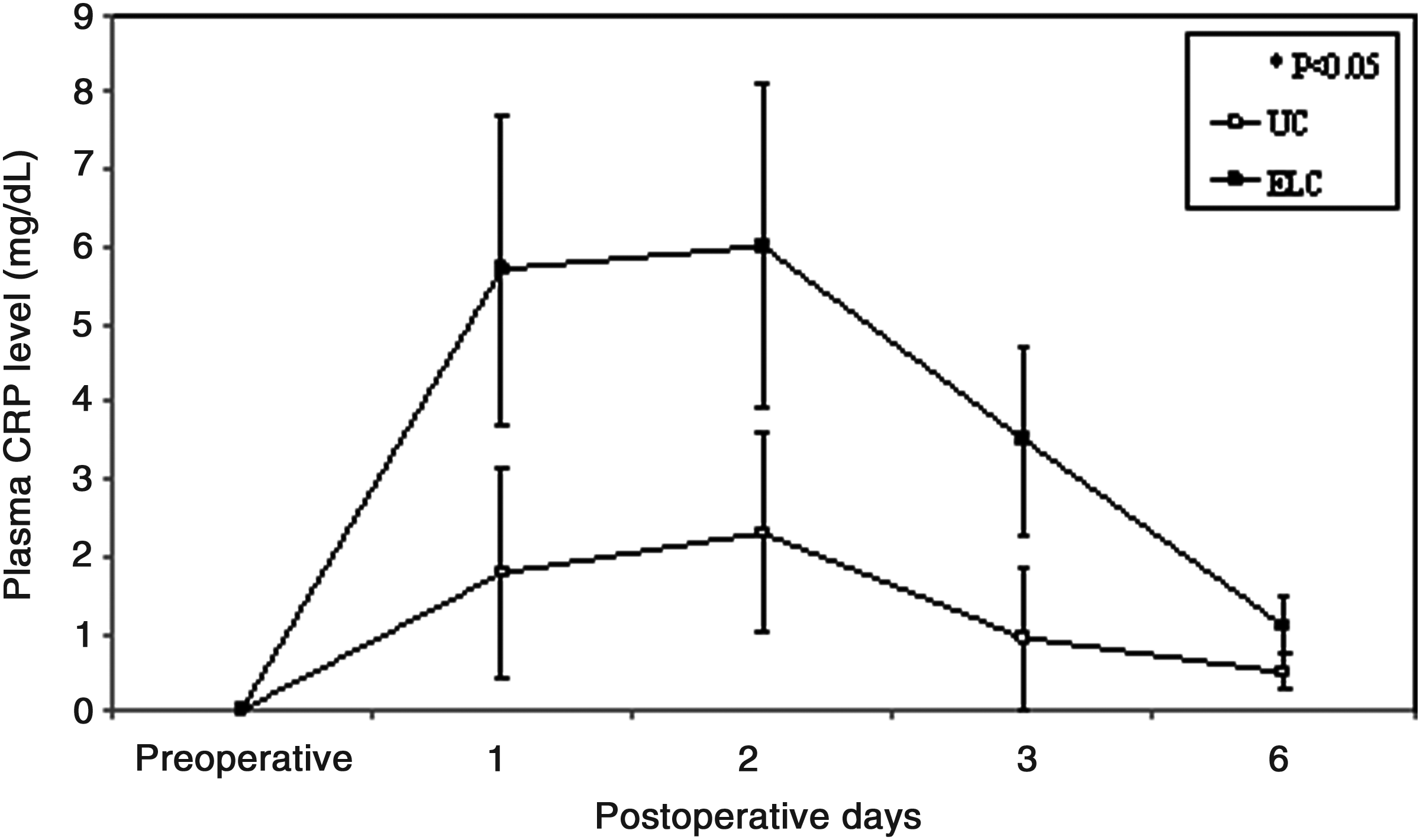
Plasma concentration of C-reactive protein (CRP) in the monopolar electrosurgery (ELC) and ultrasonic device (UC) groups. Data are mean±standard deviation values. There were significant differences between the two groups: r>0.69, P<.05 (Mann–Whitney U tests and Pearson's correlation coefficient).
The number of blood cultures positive for microorganisms was increased in the ELC group compared with the UC group (P<.05). There was no difference in bacteremia between the groups 1 week after the intervention. Microbiological analysis of blood cultures detected eight different bacterial species in the ELC group and four species in the UC group.
The systemic endotoxin concentration rose significantly during the course of surgery but returned to near baseline by 48 hours (Fig. 7). Systemic concentrations of endotoxin were higher in the ELC group at all intraoperative sampling times but reached significance only when the gallbladder was removed (ELC group, 35.76±7.21 pg/mL; UC group, 15.63±3.54 pg/mL; P<.05) (Fig. 7).
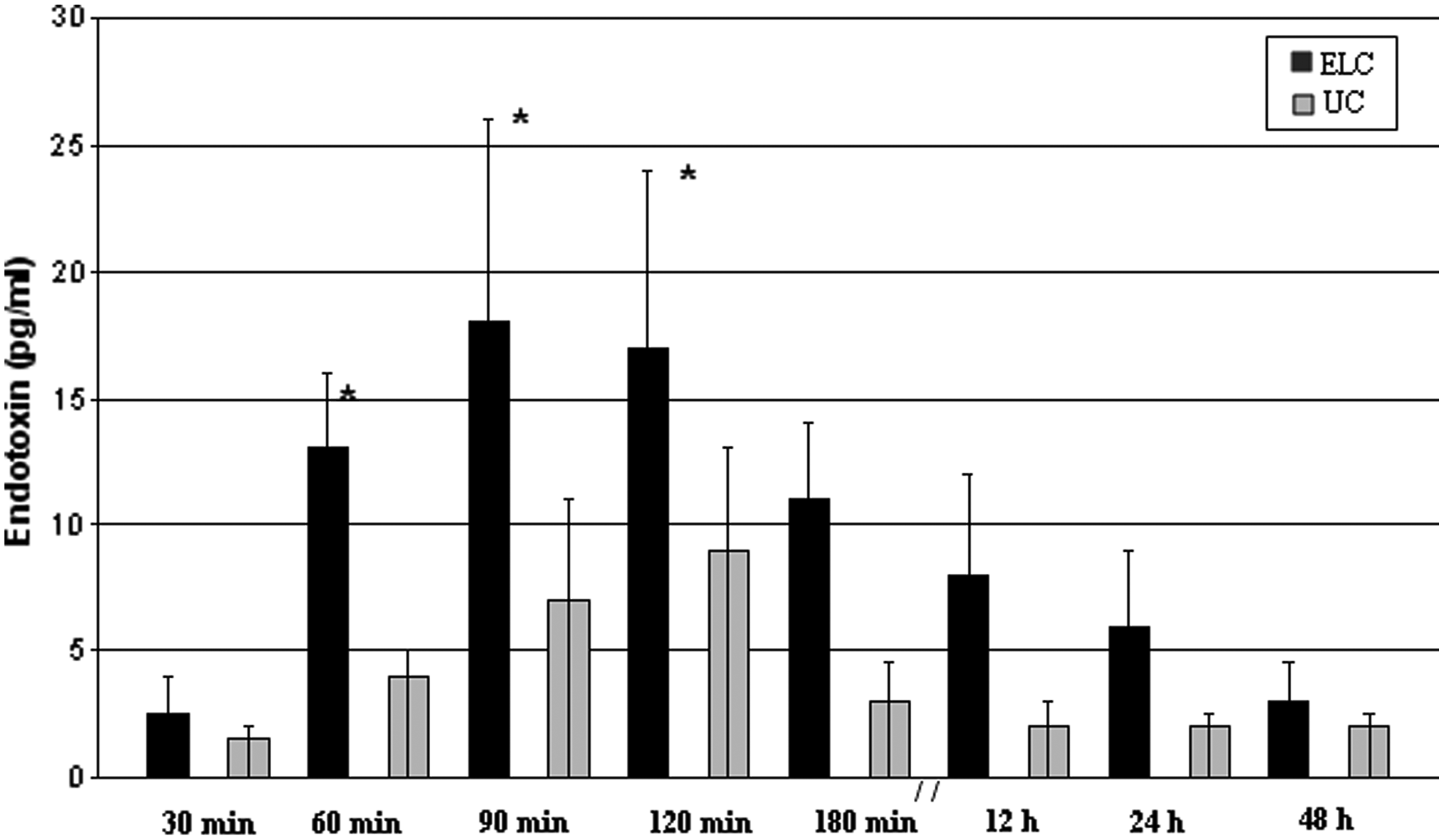
Systemic endotoxin concentration in the monopolar electrosurgery (ELC) and ultrasonic device (UC) groups. Data are mean±standard error of the mean values. *P<.05 for differences between the two groups at 60, 90, and 120 minutes.
Follow-up after 1 and 6 months, a routine procedure for all patients who undergo cholecystectomy in our hospital, showed five simple wound infections in the ELC group (three Grade I and two Grade II). These infections developed later than 10 days after surgery (from 8 to 14 days).
Discussion
Surgical trauma, tissue injury, infection, and inflammation are followed by a release of cytokines from monocytes, macrophages, fibroblasts, and endothelial cells of damaged tissue. The major cytokine is IL-6. Receptors for IL-6 are found in cells with various functions, and when activated by this cytokine, they release secondary substances that mediate inflammation and tissue remodeling.
IL-6 induces specific hepatic proteins, the most important of which is CRP.18,19 CRP is the most extensively studied acute-phase response protein following trauma and surgery. CRP levels usually rise approximately 4–12 hours after surgery and peak at 24–72 hours, remaining raised thereafter for about 2 weeks. 20 The expression of IL-6 is believed to be directly proportional to the extent of surgical trauma. 21 Both IL-6 and CRP have been shown to correlate with the severity of tissue trauma, blood loss, and duration of surgical procedure.18,19,22
Laparoscopic surgery is believed to lessen surgical trauma and thus cause less disturbance of immune function. The usual physiological reaction to injury, surgical or nonsurgical, is an early rise in stress hormone levels together with a decrease in cellular immune response. The latter manifests as a reduction in lymphocyte and macrophage interaction, decreased activity of natural killer cells, decreased lymphocyte and neutrophil chemotaxis, and a reduction in delayed-type hypersensitivity. Polymorphonuclear leukocytes play a key role in the host defense against invading microorganisms. Surgical stress affects polymorphonuclear leukocyte function during the postoperative period.18,23 Despite a few contradictory reports, systemic immunity appears to be better preserved after laparoscopic surgery than after open surgery. However, the applicability of animal studies to the clinical situation and the clinical significance of better-preserved immunity in terms of postsurgical outcome require further elucidation. 23
During surgical stress, adrenergic activation occurs in both the adrenal medulla and peripheral symphathetic neurons, and release of corticotrophin, cortisol, and catecholamines follows. The site, extent, and duration of surgery, as well as the patient's position and type of anesthesia, may all contribute to the degree of adrenergic-symphathetic response during laparoscopy; an increase in arterial tension of carbon dioxide was closely associated with adrenergic-symphathetic activation.24,25
In our opinion the results obtained through this study can be explained by the activation of adrenergic response in both groups. This response is due both to the minimally invasive laparoscopic approach and to the increased concentration of carbon dioxide in arterial blood after pneumoperitoneum. These two elements should make the different adrenergic response in the two groups not significant.
Laparoscopic cholecystectomy has gained rapid acceptance based on clinical grounds. Patients benefit from faster recovery, decreased pain, and quicker return to normal activities.26–29
The impact of surgical stress on the immune response is a possible predictive factor of a patient's clinical outcome.30–33 Laparoscopic surgery induces less trauma and is therefore less aggravating for the immune system.5–9,34,35
Laparoscopic surgery is increasingly used for intraabdominal disease complicated by inflammatory processes and peritonitis. It has been demonstrated that laparoscopic is superior to conventional open appendicectomy in terms of postoperative complications and recovery in prospective randomized trials. 36 Furthermore, laparoscopic management of perforated peptic ulcers has been reported to be simple and followed by a short recovery time.37,38
In the present study no difference in perioperative clinical parameters (age, ASA grade, and blood loss) between the studied groups was found. Our results show that laparoscopic cholecystectomy in patients with acute calculous cholecystitis, complicated by peritonitis, whether performed by electrosurgery or by Harmonic scalpel, is associated with a significant stress response, with increases in the biochemical markers measured, but the UC group was superior to the ELC group in terms of postoperative systemic inflammation as well as intraperitoneal abscess formation. In fact, the immunologic status was better preserved, and the systemic inflammatory response was lower in the UC group compared with the ELC group. The number of positive blood cultures was significantly higher in the ELC group compared with the UC group at 1 hour after intervention.
Moreover, in the ELC group we observed a postoperative decrease in expression of HLA-DR on peripheral monocytes. Patients who underwent laparoscopic cholecystectomy with the Harmonic scalpel showed no significant difference in the activity of HLA-DR expression considering the pre- and postoperative values. Previous studies have demonstrated the crucial role of this antigen in assessing the activity of the immune system. 39 HLA-DR antigen expression on monocytes has an important role in antigen presentation to lymphocytes, particularly T-helper lymphocytes 39 ; in fact, these cells require both HLA-DR and exogenic antigens on the macrophage surface to initiate proliferation. Moreover, studies have shown that HLA-DR is related to the surgical trauma and that the occurrence of postoperative sepsis is strongly correlated with less expression of the HLA-DR of peripheral monocytes. 4 Because HLA-DR expression is not significantly affected by age, sex, or race, this antigen can be considered of crucial significance in the postoperative monitoring of surgical patients. 39
Neutrophil function has been examined by measuring elastase (polymorphonuclear). Neutrophil elastase is one of the major enzymes present in neutrophils and is up-regulated during activation. 40 During the surgical procedures there is a massive release of elastase from the neutrophils, 40 along with other proteinases. Therefore measurement of the elastase–α1-proteinase inhibitor complex might be a useful indicator of the degree of surgical trauma. 10 In our study, in the ELC group we observed a postoperative increase of plasma elastase concentration. In the UC group the patients showed no significant difference in the activity of leukocyte elastase considering the pre- and postoperative values. Therefore it is conceivable that they maintain an adequate immune response even during the early postoperative phase, when the risk of infection is higher.
Concerning other serologic parameters (B- and T-lymphocyte subpopulations) in our study, no significant differences were observed between the two groups of patients and within patients of each group, considering the pre- and postoperative values.
IL-1, IL-6, and CRP showed significantly higher values in the ELC group 1 hour after intervention; levels peaked at the sixth hour (approximately 4 hours after the operation).
Endotoxin is a potent stimulator of release of cytokines such as IL-6 and tumor necrosis factor. These inflammatory mediators play an important role in the pathogenesis of systemic inflammatory response syndrome and multiple organ dysfunction syndrome. 41 In our study systemic concentrations of endotoxin were higher in the ELC group. This supports the clinical findings in this study. Intraperitoneal abscess formation was detected in 4 patients after laparoscopic cholecystectomy conducted by ELC and was significantly higher in this group compared with the UC group.
Classically, skin test responses are associated with T-cell-related immunologic function. It is thought that this would indicate any attenuated related response in this lymphocyte population for patients undergoing laparoscopic procedures. However, it must be appreciated that skin test responsiveness is a complex immune system that involves multiple interactions among lymphocytes at lymphocyte subpopulations. Any disturbance at any aspect of this immunologic cascade could affect the response. Although several studies have shown that laparoscopic groups maintain the skin test response better than laparotomy groups, it is unknown at this time which specific component is responsible for the preserved cellular immunologic function response.3,22
Therefore it is conceivable that patients undergoing laparoscopic cholecystectomy maintain an adequate immune response even during the early postoperative phase, when the risk of infection is higher. It is interesting that in our study we detected 4 cases of postoperative intraperitoneal abscess in the ELC group and only 1 in the UC group (P<.05).
The complete documentation of postoperative complications is a laborious undertaking. In many studies only the in-hospital period is analyzed. Because this interval is significantly shorter after laparoscopic operations, it is difficult to interpret the results of these studies. Considerable numbers of complications occur only after the patient has been discharged. 42 Jakeways and Carli 42 suggested that the follow-up of patients in randomized trials be continued for several weeks into the postoperative period. Therefore we have attempted to see all patients again 1 and 6 months after surgery and can report five wound infections (three Grade I and two Grade II) only in the ELC group.
In conclusion, laparoscopic cholecystectomy after biliary peritonitis, conducted by ELC, increased the incidence of bacteremia and systemic inflammation compared with the UC group. Early enhanced postoperative systemic inflammation may cause lower transient immunologic defense in the ELC group, leading to enhanced sepsis in these patients.
Footnotes
Disclosure Statement
No competing financial interests exist.