
Abstract
Abstract
Background:
The laparoscopic Kasai operation has been under debate for a long time. In this study, we described our experience in laparoscopic portoenterostomy for biliary atresia
Subjects and Methods:
The operative experience in 25 cases of laparoscopic portoenterostomy for biliary atresia since January 2011 was reviewed. For the procedure, operative cholangiography was first performed for diagnosis. Laparoscopic Kasai portoenterostomy was performed as in the open manner. Electrocoagulation hemostasis was avoided at the porta, where bleeding was controlled with direct compression only. The Roux loop was fashioned outside of the abdominal cavity through the umbilical incision, and portoenterostomy was performed with absorbable sutures.
Results:
All cases underwent the operation successfully without conversion to open surgery. The average time of operation was 180–285 minutes (mean, 208 minutes), and the blood loss was 15–30 mL. Twenty-two (88%) patients had bile drainage postoperatively as indicated by their stool color. Jaundice was alleviated in 21 (84%) patients, with total bilirubin decreased by a third. Follow-up extended from 3 months to 2 years after the operation. Jaundice had completely subsided in 14 (56%) cases, with a normal level of bilirubin. Seven patients had an initial decrease in bilirubin, but jaundice returned because of cholangitis. Two patients died because their parents refused liver transplantation. Two cases underwent successful liver transplants.
Conclusions:
Laparoscopic portoenterostomy for biliary atresia is safe and feasible. It has the advantage of clearer vision, precise operation, and less operative trauma. In our experience, the outcome of this surgery is as good as open surgery if the surgeons are well experienced.
Introduction
B
Subjects and Methods
Subjects
From January 2011 to December 2012, 25 consecutive infants with BA underwent laparoscopic Kasai portoenterostomy at our institution. All portoenterostomies were performed by the same surgeons with experience in minimally invasive surgery. The 25 children (11 boys and 14 girls) had a mean age of 72 days (range, 46–123 days) at operation. One of the 25 patients had type II BA, and the other 24 had type III. Liver function and liver ultrasonic inspection were performed preoperatively.
Surgical technique
Laparoscopy is performed with the patient in a supine frog position. A 10-mm port is introduced paraumbilically. Two 3-mm trocars are inserted at the right upper and middle abdomen, respectively. Laparoscopic examination is performed. Usually, a contracted gallbladder associated with a fibrotic extrahepatic duct is identified. In the case of doubtful patency of the extrahepatic duct, operative cholangiography is performed to check the patency of the extrahepatic bile duct. After the diagnosis of BA is confirmed (Fig. 1), a 5-mm trocar is inserted into the left upper quadrant. Then the ligamentum teres hepatis and the liver are suspended, and the porta hepatis is exposured. The gallbladder is removed after transection of the porta hepatis tissue. Resection of the fibrous cord by an electrotome is prohibited, and hemostasis by electrocautery should be avoided. Bleeding from the liver surface is controlled by direct pressure. The proximal jejunum is delivered through an enlarged paraumbilical incision. A 35-cm jejunum is used to fashion the Roux loop outside the abdominal cavity. Then it is returned into the peritoneal cavity, the 35-cm Roux-en-Y loop is passed retrocolically to the hilum, and the uninterrupted end-to-side anastomosis is completed with the side of the jejunal loop (Fig. 2–5).

Cholangiography.
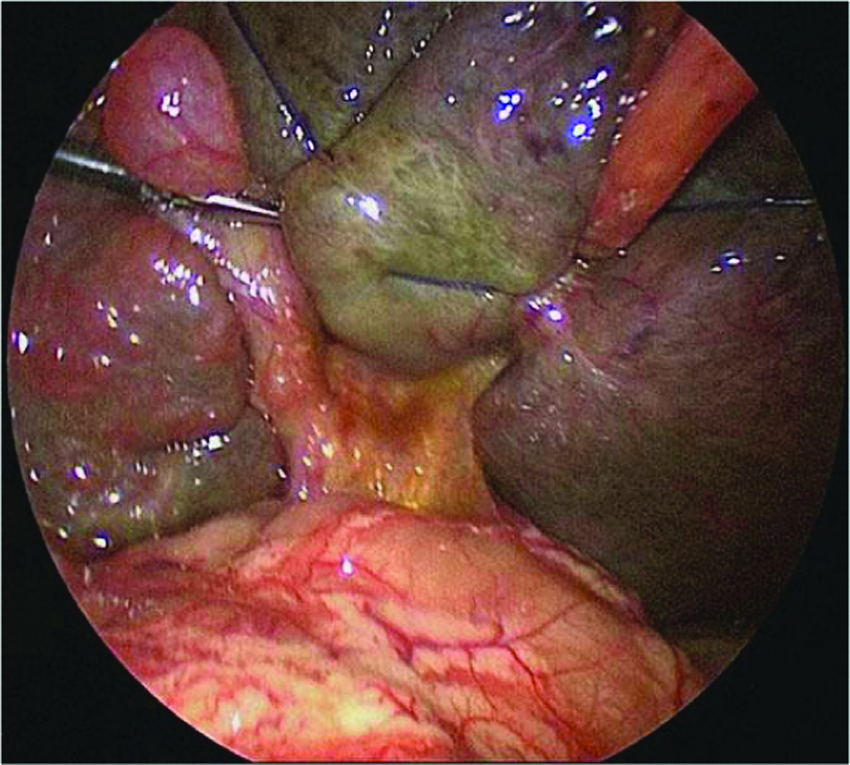
Exposure of the porta hepatis.
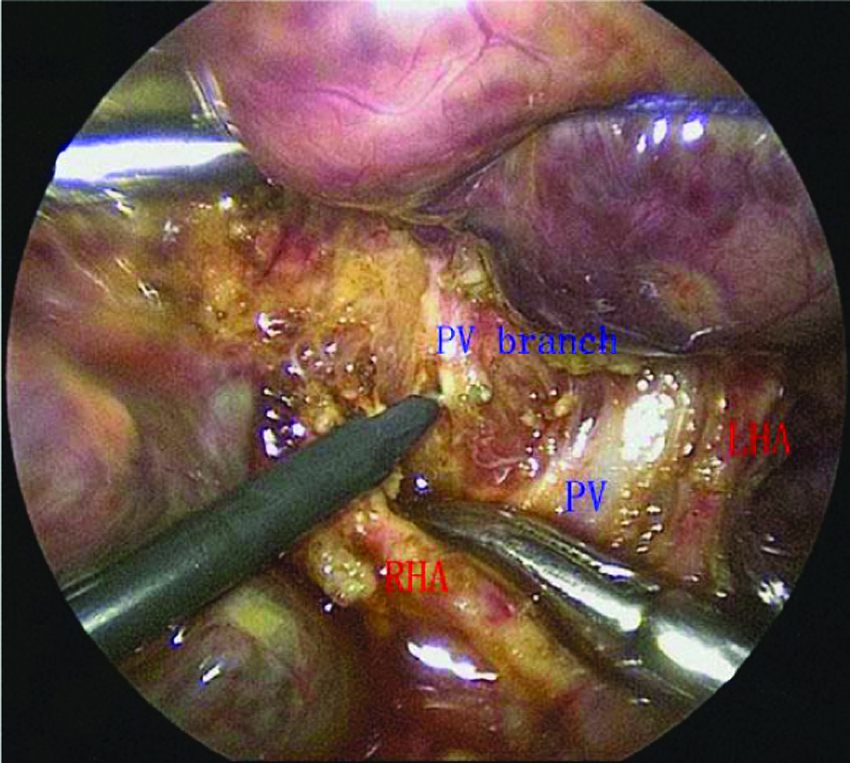
Tiny branches of the portal vein are distinguished around the block.
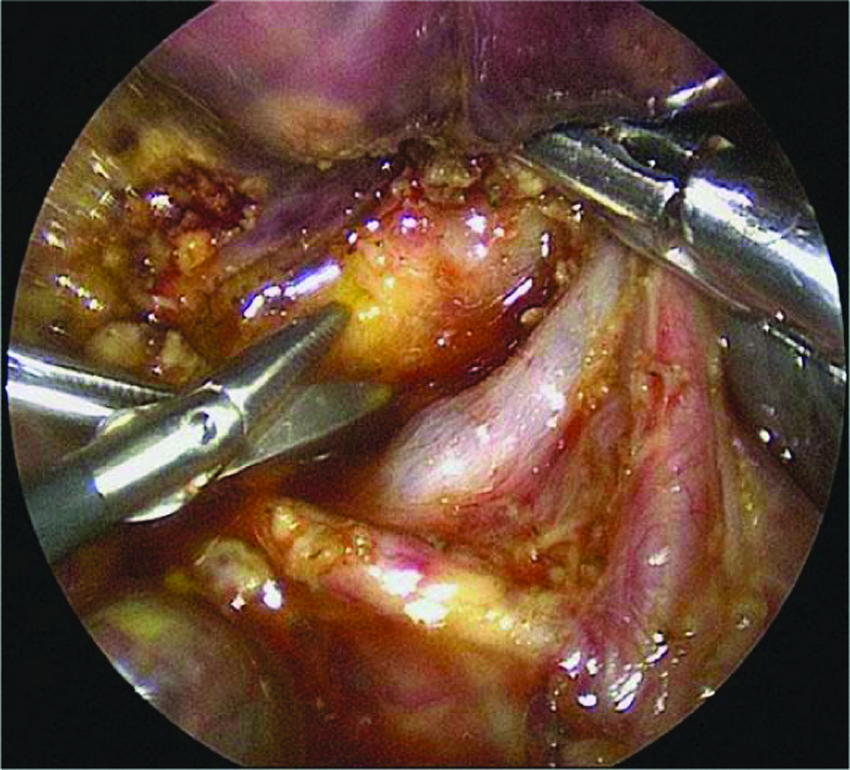
Resection of the fibrous cord.
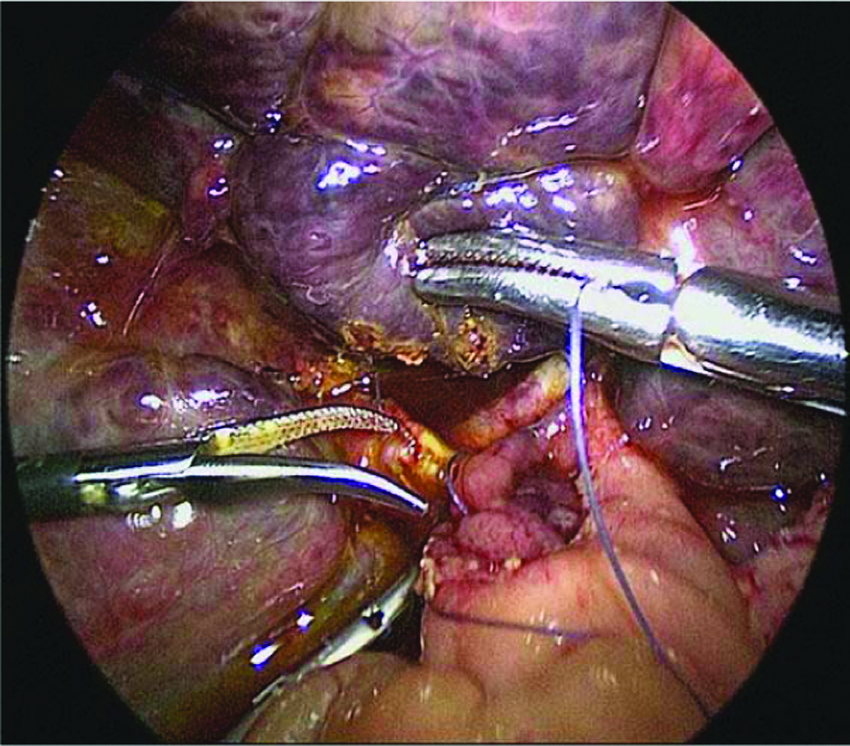
Portoenterostomy was completed with the side of the jejunal loop.
Medication
Intravenous antibiotics are used for 1 or 2 months and then stopped, after which antibiotics are taken orally, lasting for 6 months. Steroid is taken beginning 3 days after surgery (4 mg/kg/day), and we reduce the dose gradually 2 weeks later, lasting for 3 months.
Results
The operative time ranged from 180 to 285 minutes (mean, 208 minutes). It was evident from our operative times that the learning curve reached a plateau after Case 9 (Fig. 6). The amount of bleeding during the operations was between 10 and 20 mL; intraoperative blood transfusion was performed when necessary. Twenty-two (88%) patients had bile drainage postoperatively as indicated by their stool color. Jaundice was alleviated in 21 (84%) patients, with the level of total serum bilirubin decreased by a third. With follow-up of 3–24 months, 14 patients (56%) were free of jaundice, with the direct serum bilirubin level <20 μmol/L 1 year later, and no liver transplantation was needed. The jaundice of 12 patients (48%) declined by an unsatisfactory amount: 7 had an initial decrease in serum bilirubin, but jaundice recurred because of cholangitis; 2 patients died because their parents refused liver transplantation; and 2 cases underwent successful liver transplant. All cases underwent the operation successfully without conversion to open surgery. Postoperative wound dehiscence, intestinal obstruction, and other complications did not occur. The incision scar was not obvious.
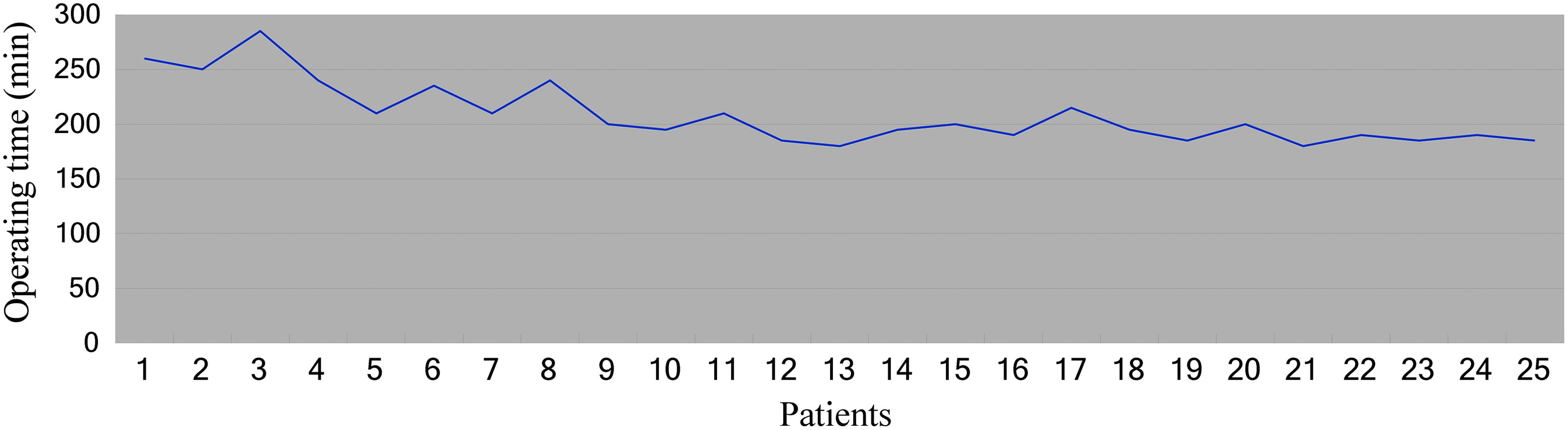
Operating times in 25 cases of biliary atresia.
Discussion
BA is a very serious liver disease in infants. The only method to treat BA is surgery. Up until now, Kasai radical surgery is still the mainstay of treatment in BA, and the only treatment for later-period patients or Kasai radical surgery failure cases is liver transplantation. After Esteves et al. 4 reported Kasai laparoscopic surgery first in 2002, more and more surgeons have accomplished it successfully.5–8 Lots of controversy exists about laparoscopic Kasai portoenterostomy, which emphasized electrocoagulation and exposure of the visual field. 3
The key point of the Kasai procedure is to completely cut off the hepatic portal fiber block in order to make one side of the section reach to the liver parenchyma next to the entrance of the portal vein, lengthwise up to the level of the portal vein posterior paries. What is more, the depth and length of resection are also very important: too shallow may cause the resection not to reach the correct intrahepatic bile duct, whereas too deep may damage the liver parenchyma and influence the anastomotic healing. In general, when the fiber block is resected in portal hepatis, the liver surface holds only a very thin capsula. 9 Second, electrocoagulation should be used with caution to stop the section from bleeding, especially at the left and right hepatic ducts into the liver parenchyma; using article gauze to oppress hemostasis can also achieve a certain effect. To accomplish this target in traditional surgery, surgeons cut a larger incision and pull the liver out of the body to operate on with the help of surgical magnifier. 10
We considered that an elaborate and accurate operation dominated in determining the effect of surgery. At the beginning of this surgery, we used laparoscopic exploration and cholangiography to diagnose and then do the Kasai laparotomy surgery. We found that, during the hepatic portal fiber block separation, we can barely distinguish tiny branches of portal vein around the block by the naked eye, so the resection of the fiber block will easily cause bleeding. We have tried to operate with a laparoscope; consequently, we can see the relation between tiny vessels around the fiber block and portal vein very clearly (Fig. 3). Before the resection, if we do the electrocoagulation of those tiny vessels with a coagulation hook, it will not cause bleeding at all. Oppression hemostasis after resection of the fiber block by gauze can achieve the ideal hemostatic effect. We discovered, during the surgery, bile often oozing from the center of the fiber block and at the 2 and 10 o'clock positions of the visual field, which is consistent with some scholars' common view. When we are dealing with the circum tissue of fiber block, we found there was neither superfine bile nor bile leakage. We believe that staunch with electrocoagulation is feasible, but we will not do that when resecting the fiber block in order to avoid damage to superfine bile ducts. In the 25 cases we have completed, macrovascular damage does not appear, and no case required conversion to laparotomy.
The operative difficulties of laparoscopic surgery are visual field exposure and manipulation. All of the BA patients' livers were swollen, and the laparoscopic operative space is very narrow, so the operation has certain difficulties. Our new achievements are the tricks in our experience of how to resect the fiber block and how to expose the porta. We hang the ligamentum teres hepatis, gallbladder, or liver tissue to expose visual field more clearly (Fig. 2). First, we cut the fiber block from the middle of the vertical line to the liver capsule (Fig. 4) and then along both sides of the liver capsule extending up into the liver at the right and left hepatic arteries. The operation and anastomosis surgery have a certain degree of difficulty, and surgeons need extensive laparoscope skills and must have practiced laparoscopic biliary surgery experience.
According to our postoperative short-term observations, 88% of patients had bilious stool, and 84% of patients had significantly reduced bilirubin levels after a month, consistent with the laparotomy effect, indicating that the surgical operation achieved its purpose. The follow-up time of our patients is too short to know the long-term effect, which will require further observation.
Also learned from our experience is that not every patient can undergo Kasai surgery. In the laparoscopic bile duct exploration, we saw some patients with BA do not have a fiber block at the hepatic portal or that the fiber block is very small. We believe that, in this condition, the Kasai procedure surgery will not work, which means the bile drainage cannot be set up, so the portoenterostomy will cause greater damage to patients. Liver transplantation is the most effective treatment for these patients. And, in this case, laparoscopic exploration has more obvious advantages than laparotomy exploration.
The prognosis of BA is a complex process. The short-term effect reflects the degree of the fiber block resection, and there is a close connection among the long-term effect and the type of BA, area of fiber block, the preoperative level of liver dysfunction, liver fibrosis, and the occurrence of cholangitis.
Laparoscopic portoenterostomy for BA is safe and feasible. It has the advantage of clearer vision, precise operation, and less operative trauma. In our experience, the outcome of this surgery is as good as open surgery if the surgeons are well experienced.
Footnotes
Disclosure Statement
No competing financial interests exist.