
Abstract
Abstract
Background:
Laparoscopic repair of congenital duodenal obstruction has become popularized over the past decade. Comparative data on outcomes, however, are sparse. We hypothesized that laparoscopic repair of congenital duodenal obstruction could be performed with similar outcomes to traditional open repair.
Patients and Methods:
Medical records for all cases of congenital duodenal obstruction from 2005 to 2011 at three academic teaching hospitals were retrospectively reviewed. Patients were excluded from the analysis if they had confounding surgical diseases, did not have duodenoduodenostomy during the first hospital admission, had the repair performed before transfer from a referring hospital, or weighed less than 1.7 kg at the time of surgery. Analysis was performed as intention to treat, with laparoscopic converted to open cases included in the laparoscopic group.
Results:
Sixty-four cases were included in the analysis (44 open, 20 laparoscopic). Baseline characteristics were similar between the two groups with the exception that the open group, on average, underwent repair later than the laparoscopic group (6 days versus 4 days, respectively). Seven laparoscopic cases were converted to an open procedure (35%), most commonly for difficulty in exposing the decompressed distal duodenum. Laparoscopic repair did take significantly longer than open repair (145 minutes versus 96 minutes, respectively), but clinical outcomes were similar. Complications were rare and were similar between methods of repair. Two patients in the laparoscopic group required subsequent open revision.
Conclusions:
Laparoscopic duodenoduodenostomy for congenital duodenal obstruction is a technically challenging procedure with a steep learning curve. Despite a relatively high conversion rate, clinical outcomes remained similar to the traditional open repair in selected patients.
Introduction
We hypothesized that laparoscopic repair of congenital duodenal obstruction could be performed with similar outcomes to the traditional open repair across multiple centers. Additionally, we hypothesized that the learning curve for this procedure would be steep and that conversion rate and outcomes would vary as a function of surgeon experience with the procedure.
Patients and Methods
Retrospective review of patient records from 2005 to 2011 was performed at three major teaching hospitals after Institutional Review Board approvals. The protocol for this study was given Children's Hospital Los Angeles Human Subjects Approval number CCI-11-00136.
Patient demographics, comorbidities, operative details, and postoperative outcomes and complications were recorded.
Patient identification and selection
Patients were identified using several database techniques. Hospital billing registries were queried for discharge diagnosis of intestinal atresia (ICD-9 Code 751.1) or congenital anomalies of pancreas (ICD-9 Code 751.7), and operative reports were reviewed to exclude patients with jejunal, ileal, or colonic atresia, as well as pancreatic anomalies not leading to duodenal obstruction. Finally, operating room case databases were reviewed for procedure description of “duodenoduodenostomy.”
Patients were excluded from analysis based on factors that would either (1) impact suitability for laparoscopic repair and introduce selection bias or (2) impact and potentially confound postoperative outcomes. Although laparoscopic repair has been performed in patients as small as 1.3 kg,3,4 patients who weighed less than 1.7 kg at the time of surgery were deemed unlikely to undergo attempted laparoscopic repair at our respective centers. Other exclusion criteria included repair not performed on initial hospitalization (delayed presentation), confounding surgical conditions (e.g., tracheoesophageal fistula) that would prolong hospital course, and initial treatment with side-to-side duodenojejunostomy. Patients who had already undergone duodenoduodenostomy before transfer to one of the institutions were also excluded from the analysis.
Operative technique
Operative approach was determined by the attending surgeon. Open treatment was performed via a traditional transverse laparotomy. Laparoscopic approach was not standardized between surgeons or between centers but was generally performed with three or four trocars placed in variable positions, depending on surgeon preference. Duodenoduodenostomy was generally performed using the diamond-shaped technique of Kimura et al. 9 All cases utilized laparoscopic suturing with intracorporeal knot tying. Two sutures were generally used in a running fashion, one each for the posterior and anterior rows. Evaluation for distal atresia was not routinely performed, and when it was done, it was not uniform. Methods used included either nasoduodenal or transabdominal placement of a small feeding tube for distal irrigation. Postoperative contrast studies were not routinely used in either group. A standardized postoperative feeding regimen was not implemented at any of the centers.
Statistical analysis
All comparative analyses were performed as intention to treat. Cases started laparoscopically that were converted to open procedures were included in the laparoscopic group. Binary frequency data were compared using Fisher's exact test, and continuous variables were compared using the Mann–Whitney U test. Categorical data were compared using two-tailed chi-squared analysis for independence with Yates's correction for frequencies of <5. Univariate logistic regression was used to identify predictors of conversion to laparotomy. Multivariate regression analysis was not possible because the number of conversion events was insufficient to study more than one variable without unacceptable risk of Type II error. A P value of <.05 per comparison was considered statistically significant.
Results
Ninety-eight patients with congenital duodenal obstruction were identified. Thirty-four patients were excluded: repair before admission, 16; less than 1.7 kg, 4; delayed presentation, 4; primary side-to-side duodenojejunostomy, 2; concomitant tracheoesophageal fistula, 4; congenital diaphragmatic hernia, 2; gastroschisis, 1; and biliary atresia, 1. Sixty-four cases met the criteria for analysis (44 open, 20 laparoscopic).
Baseline characteristics were similar between laparoscopic and open groups with the exception that the open group, on average, underwent repair 2 days later than the laparoscopic group (Table 1). Laparoscopic repair has increased in relative frequency over time (Fig. 1) (r2=0.41). Usage of laparoscopy varied considerably among centers (15%–57%). Etiology of duodenal obstruction was similar between groups (Table 2). Operative procedure (duodenoduodenostomy or excision of duodenal web) and additional procedures (gastrostomy tube and correction of malrotation) were used with similar frequencies in both groups (Table 3).
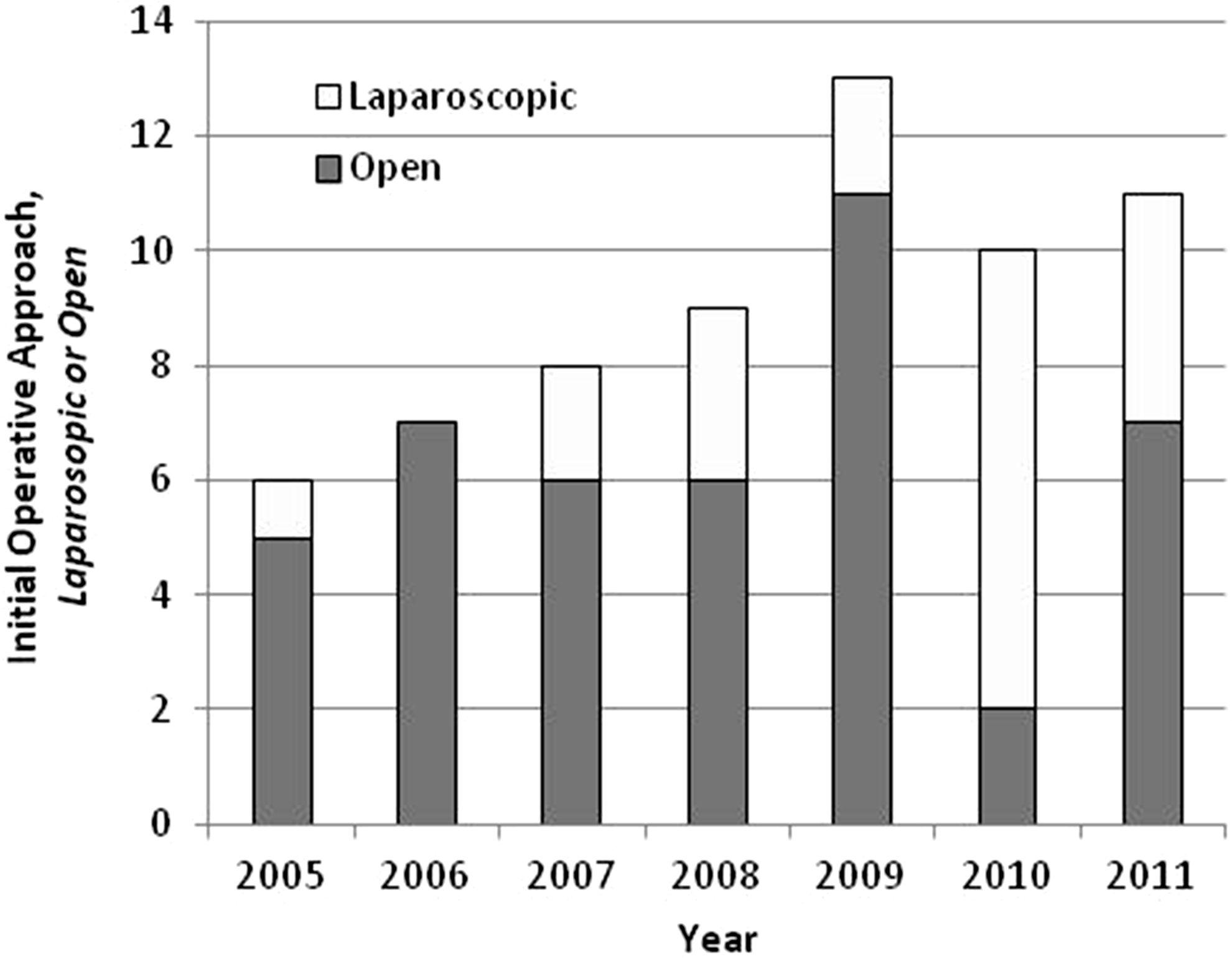
Laparoscopic and open correction of congenital duodenal obstruction by year.
Data are median (range) values.
Calculated by Mann–Whitney U test.
Data are frequency (%).
Calculated by chi-squared goodness of fit (with Yates's correction).
Data are expressed as frequency (%).
Calculated by Fisher's exact test.
Short-term clinical outcomes and overall complications are shown in Table 4. Compared with the open technique, laparoscopic repair was associated with significantly longer operative times. Despite this longer operative time, time to feeding, ventilator days, time to discharge, and complications were similar to those in the open group. Surgeon experience did not correlate with time to feeding or length of stay (r2<0.03). Short-term complications were rare and were similar between methods of repair. Two patients in the laparoscopic group required subsequent re-exploration via laparotomy for persistent or recurrent obstruction. One patient was re-explored 2 weeks postoperatively and found to have a missed duodenal web. A second patient developed an anastomotic stricture 1 year postoperatively that required open revision.
Data are median (range) values or frequency (%).
Calculated by Mann–Whitney U test.
Calculated by Fisher's exact test.
Seven laparoscopic cases required conversion to an open procedure (35%), most commonly for difficulty in exposing the decompressed distal duodenum (n=4). Other indications for conversion included atresia in the third portion of the duodenum (n=1), concern for additional distal atresia (n=1), and thermal injury to the distal duodenum (n=1). Conversion rate was lowest in the two centers that used the laparoscopic approach in more than 50% of cases (21% versus 66% in the third center). Conversion rate correlated with surgeon experience, although the trend was not statistically significant (Fig. 2) (r2=0.23, P=.12). Patients converted to laparotomy weighed significantly less at the time of surgery than those whose procedures were completed laparoscopically (Table 5).
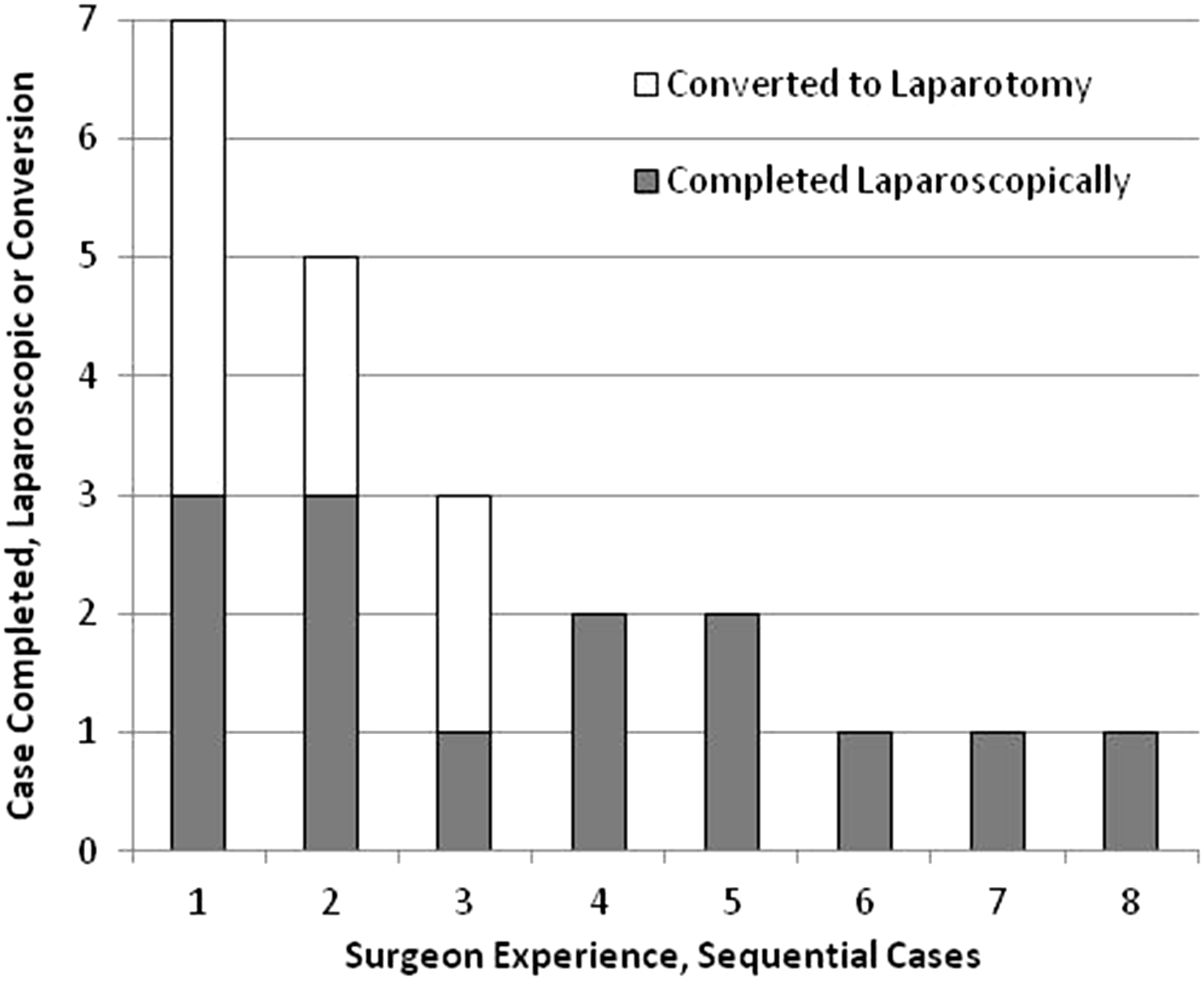
Conversion rate by surgeon experience. The x-axis represents consecutive attempts at laparoscopic repair of congenital duodenal obstruction over time for an individual surgeon. All conversions were within the first 3 cases of any individual surgeon's experience, demonstrating the early learning curve of procedure.
Data are median (range) values or frequency (%).
Calculated by Mann–Whitney U test.
Calculated by Fisher's exact test.
Calculated by chi-squared goodness of fit with Yates's correction.
Discussion
This study represents an early experience with the implementation of laparoscopic correction of congenital duodenal obstruction across three institutions. To our knowledge, this is the first study comparing the outcomes between laparoscopic and open repair of congenital duodenal obstruction in a multicenter fashion. The procedure has historically been regarded as technically challenging. Both Hill et al. 7 and Burgmeier and Schier 3 reported that more than a quarter of their cases were converted to open. In our current series, we experienced a 35% rate of conversion to laparotomy. Conversion to laparotomy and surgeon experience with laparoscopic repair of congenital duodenal obstruction seemed to correlate, but the relationship was not statistically significant and likely represented a Type II error. We believe this high rate of conversion is largely due to the learning curve because all the conversions occurred during the first 3 cases of any individual surgeon's experience. Furthermore, the overall experience of each individual surgeon varied widely among the surgeons in this study, which may have contributed to our higher conversion rate.
The operative time in our laparoscopic series appeared to be longer than in other reported contemporary series. This may be related to our intention-to-treat analysis combined with the higher conversion rate. With this intention-to-treat analysis, the higher rate of conversion to open procedures (35% in our series versus 0%–26% in other series) definitely prolonged the apparent overall operative time. Additionally, we included all concomitant procedures (e.g., gastrostomy placement and correction of malrotation) in our total operative time, whereas prior series only reported time for the duodenoduodenostomy portion of the procedure.3,4,7,8
Despite longer operative times and a higher conversion rate, overall outcomes, including postoperative ventilatory requirement, intensive care unit stay, wound complications, postoperative time to feeding, and time to discharge, were similar to those of traditional open repair in our institutions. Compared with other series, however, median time to initiation of feeds and achievement of full feeds in our study group were 2–5 days longer.7,8,10 Despite this delay, our overall length of stay (median, 20 days) was similar to those of most other laparoscopic series except that of Spilde et al. 8 (12.9 days). It is unclear why time to feeding is not shorter in the laparoscopic group, other than to attribute this to our own feeding practices. Although none of our centers used a standardized postoperative feeding protocol, our general practice was to wait until resolution of bilious drainage from the nasogastric tube. In contrast, Spilde et al. 8 reported early initiation of feeds following routine upper gastrointestinal contrast studies in their laparoscopic group, despite bilious nasogastric drainage. Some surgeons may initiate feeding earlier in the laparoscopic group because of the perceived “noninvasiveness” of the procedure.
Proposed benefits of laparoscopy that were not specifically measured in this study include reduced postoperative pain and improved cosmesis. The retrospective nature of the study precluded adequate evaluation of cosmesis. Nonetheless, in addition to the surgical attending staff, most parents were quite satisfied by the cosmetic outcome of the laparoscopic repair. The retrospective design also made it difficult to adequately assess pain and need for narcotics in the postoperative period, particularly given the significant proportion of patients with Down's syndrome in the study. These patients generally represent a challenge in the intensive care unit relative to postoperative sedation. In many instances, narcotics were used as a sedative in combination with more traditional anxiolytic agents (midazolam, dexmedetomidine); therefore, it was not possible to differentiate indications for narcotic administration for pain versus sedation. We were not surprised to find that although narcotic usage varied highly between patients in both the open and laparoscopic groups, it was not significantly different—although whether this represents a lack of difference in postoperative pain is unclear.
This study is limited by its retrospective nature and susceptibility to selection bias. We attempted to minimize this selection bias by excluding patients too small to be considered for a laparoscopic approach in our institutions and patients presenting later in life (who tend to be less technically challenging, are more likely to be approached laparoscopically, and generally have better postoperative outcomes). Furthermore, we excluded patients with concomitant surgical diseases that would prolong postoperative feeding and overall hospital course. An additional limitation is that operative technique was not standardized across surgeons or across centers. Furthermore, the relatively small number of patients and low number of complications make it impossible to determine whether differences in safety really exist. Despite these limitations, this study reflects a real-world application of minimally invasive techniques without a detectable detrimental effect on patient outcomes. Because of the intention-to-treat analysis, the outcomes of the laparoscopic group were somewhat skewed by 35% of the patients undergoing laparotomy and may not adequately reflect the benefits of the laparoscopic approach. We expect that as experience is gained and conversion rate decreases, these outcomes will improve.
Conclusions
Laparoscopic duodenoduodenostomy for congenital duodenal obstruction is a technically challenging procedure with a steep learning curve. Despite a relatively high conversion rate, clinical outcomes remained similar to those with the traditional open repair in selected patients. This laparoscopic technique can be safely applied across multiple centers with similar outcomes to traditional open repair and the cosmetic benefits associated with laparoscopy. As surgeon and institutional experience grows, outcomes with the laparoscopic technique will likely improve. Longitudinal study as more centers implement this technique is warranted.
Author Contributions
All authors participated in the study design. A.R.J. and S.S.S. acquired the data. A.R.J. performed statistical analysis. A.J.R., S.S.S., and N.X.N. performed data analysis and interpretation. A.R.J. and S.S.S. drafted the manuscript. D.M.A., M.B.T., P.K.F., C.E.S., K.W., and N.X.N. performed critical review and revision. A.R.J. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
Disclosure Statement
No competing financial interests exist.