
Abstract
Abstract
Objectives:
The use of magnets in transumbilical cholecystectomy (TUC) improves triangulation and achieves an optimal critical view. Nonetheless, the tendency of the magnets to collide hinders the process. In order to simplify the surgical technique, we developed a hybrid model with a single magnet and a curved grasper.
Patients and Methods:
All TUCs performed with a hybrid strategy in our pediatric population between September 2009 and July 2012 were retrospectively reviewed. Of 260 surgical procedures in which at least one magnet was used, 87 were TUCs. Of those, 62 were hybrid: 33 in adults and 29 in pediatric patients. The technique combines a magnet and a curved grasper. Through a transumbilical incision, we placed a 12-mm trocar and another flexible 5-mm trocar. The laparoscope with the working channel used the 12-mm trocar. The magnetic grasper was introduced to the abdominal cavity using the working channel to provide cephalic retraction of the gallbladder fundus. Across the flexible trocar, the assistant manipulated the curved grasper to mobilize the infundibulum. The surgeon operated through the working channel of the laparoscope.
Results:
In this pediatric population, the mean age was 14 years (range, 4–17 years), and mean weight was 50 kg (range, 18–90 kg); 65% were girls. Mean operative time was 62 minutes. All procedures achieved a critical view of safety with no instrumental collision. There were no intraoperative or postoperative complications. The hospital stay was 1.4±0.6 days, and the median follow-up was 201 days.
Conclusions:
A hybrid technique, combining magnets and a curved grasper, simplifies transumbilical surgery. It seems feasible and safe for TUC and potentially reproducible.
Introduction
Recent reports from our group have examined the feasibility and safety of magnet-assisted transumbilical surgery in a range of operations, showing adequate triangulation and effective retraction of target organs.5–7 Still, this novel technique during TUC requires the use of two magnets, which increases procedural complexity, chiefly because of the risk of magnet collision (especially in the pediatric population). In an effort to further simplify the procedure, we modified our approach with magnet-assisted TUC using a hybrid technique with only one magnet and a curve grasper. The aim of the preliminary study is to report the feasibility and safety of this hybrid technique during TUC in a pediatric population.
Patients and Methods
We conducted a retrospective review of all pediatric patients undergoing magnet-assisted TUC between September 2009 and July 2012. Of 260 magnet-assisted surgical procedures performed, 87 were TUC. Of those, 62 (71.2%) were performed with a hybrid strategy: 33 in adults and 29 in pediatric patients.
The diagnosis of gallbladder disease was made based on history and physical examination, and preoperative imaging was left to the discretion of the operating surgeon. In general, patients with prior abdominal operations, with hemodynamic instability, or with low body weight (<15 kg) were not considered candidates for the magnet-assisted TUC technique. Charts were reviewed for presenting history, patient demographics, intraoperative diagnosis, operative time, operative conversions, length of hospital stay, and in-hospital complications.
Operative technique
With the patient under general anesthesia, a 12-mm trocar and a 5-mm flexible trocar were inserted at the umbilical base using the Hassan technique. The peritoneal cavity was insufflated to 10 mm Hg with CO2. Through the 12-mm trocar, we introduced an 11-mm, 0° laparoscope with a 27-cm-long, 6-mm working channel (Karl Storz, Tuttlingen, Germany). A spring-loaded alligator grasper attached to an 11-mm neodymium magnet (Imanlap, Buenos Aires, Argentina) was then deployed to the abdominal cavity through this trocar. A powerful external magnet (Imanlap) controlled the internal magnet by magnetic forces transmitted across the abdominal wall. Next, we introduced a nonmagnetic, custom-made surgical tool (Thomas forceps; Imanlap) through the scope's working channel. This tool opened and closed the jaws of the internal magnet. The internal magnet grasped the gallbladder fundus and provided dynamic traction by repositioning the external magnet on the abdominal wall. Varying the distance between the external magnet and the abdominal wall regulated the amount of force that was transmitted to the internal magnet. After adequate exposure was obtained, the external magnet was fixed in place with a self-retaining retractor. Subsequently, we introduced a 5-mm×45-cm (Imanlap) nonmagnetic curved grasper into the abdominal cavity across the flexible trocar. This grasper mobilized the infundibulum, generating the necessary countertraction to visualize the triangle of Calot and obtain an adequate critical view (Figs. 1–3). Once the surgical field is exposed, each 5-mm instrument (dissection forceps, scissors, hook, Harmonic® [Ethicon Endo-surgery, Cincinnati, OH] scalpel, clips, suction probe, needle handle, etc.) can be passed through the working channel of the laparoscope to complete dissection, ligation, and section of the cystic duct and vessels along with gallbladder dissection in the usual way that the traditional laparoscopic cholecystectomy is performed. In the case of a patient requiring an imaging study of the biliary tree, a percutaneous puncture was done at the right subcostal area with a 14-gauge Abbocath™ catheter (Abbott Laboratories, Abbott Park, IL) and a double-lumen pediatric feeding tube.
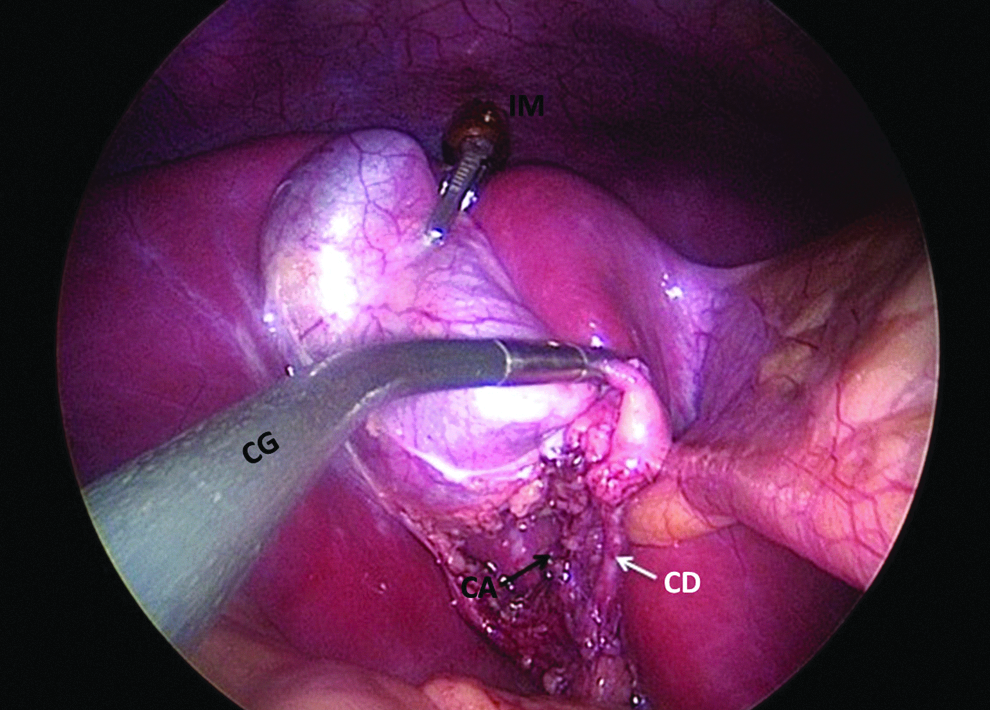
Intraoperative photograph. Both the internal magnet (IM) and the curve grasper (CG) provide traction to the gallbladder and open the triangle of Calot while the dissection is performed through the operative laparoscope. CA, cystic artery; CD, cystic duct.
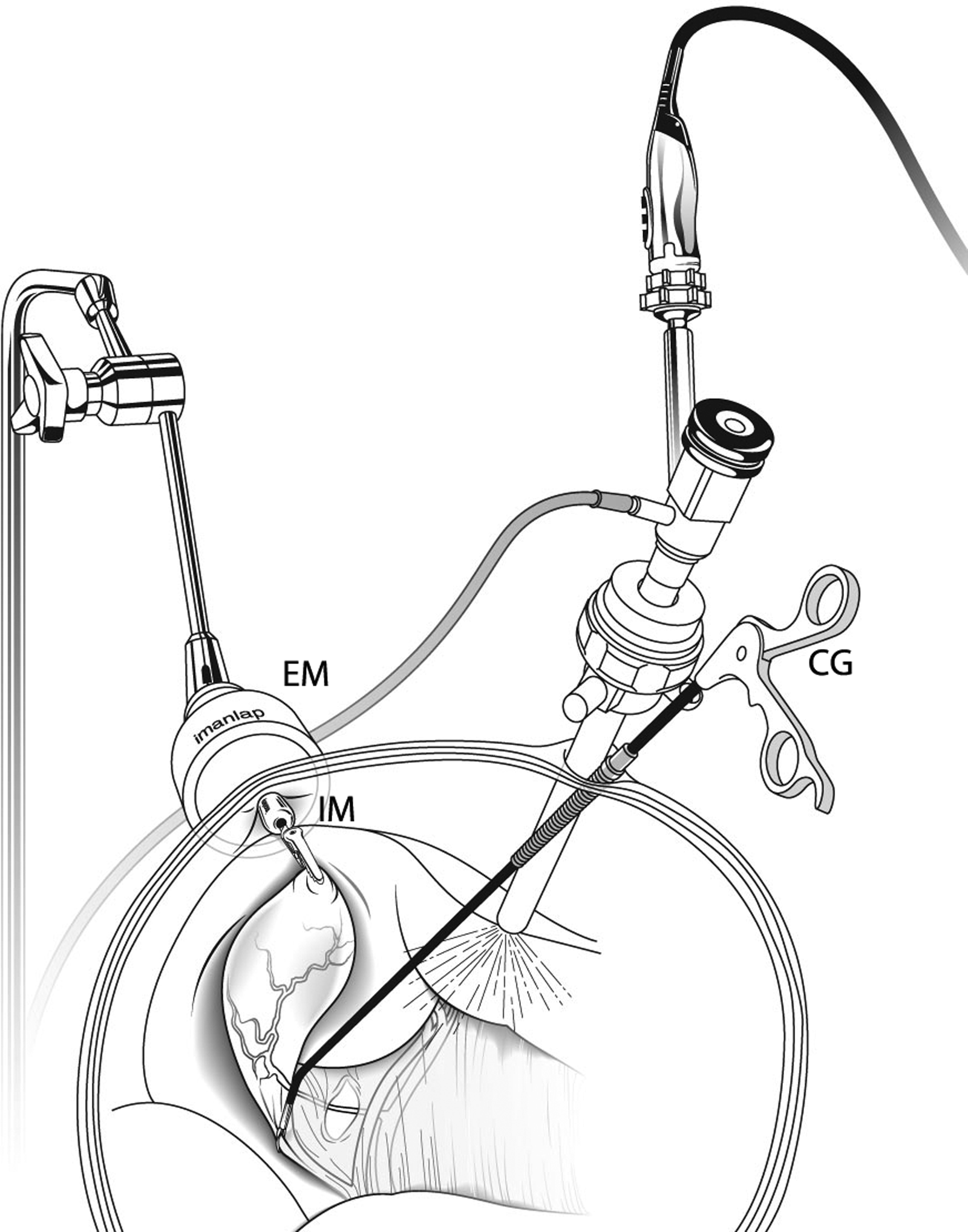
Drawing illustrating the hybrid transumbilical cholecystectomy technique. Note the external magnet (EM) controlling the internal magnet (IM). The magnetic grasper is retracting the fundus, while the curve grasper (CG) mobilizes the infundibulum.

The external view shows the two umbilical ports. The flexible trocar is placed inferiorly at the umbilical incision to prevent interference between the operator and the assistant.
Oral intake was resumed ad libitum, and early ambulation was encouraged. Requirements for discharge from the hospital were as follows: afebrile for 24 hours, eating a regular diet, and adequate pain control with oral analgesics. The wound was inspected every day during the hospital stay and on postoperative Day 7 at the outpatient clinic.
Results
Of the 260 magnetic-assisted laparoscopic surgeries performed, 29 were pediatric patients (11 boys and 18 girls) who underwent hybrid TUC during the 23-month study period. The mean age was 14 years, with ages ranging from 4 to 17 years. The mean weight was 50±24 kg (range, 18–90 kg), and operative time was 62 minutes (range, 50–70 minutes). The mean hospital stay was 1.4±0.6 days, and the median follow-up was 201 days (range, 42–429 days).
All of the operations were uneventful and completed through the transumbilical route, with no need to convert to open surgery or to add a second port. At the follow-up visit, the umbilical incisions had healed with no complications, leaving no visible scar.
In all cases, the primary operator as well as the assistants handled the magnet devices easily and did not experience problems during triangulation. In 2 cases, we performed an intraoperative cholangiography because of a suspected choledocholithiasis. Both imaging studies were normal, and no additional biliary tract instrumentation was needed.
Discussion
Laparoscopic surgery has become the gold standard for many operations because of faster recovery, less pain, and better cosmetic results compared with open surgery. Several innovative surgical techniques have been shown to minimize the number and size of the abdominal incisions, including natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) and single-incision laparoscopic surgery (SILS).2,3,8 Although surgeons initially accepted NOTES, the adoption of this technique was very slow because it requires visceral injury to access the peritoneal cavity. Alternatively, SILS is gaining in popularity; however, current available techniques may often lead to inadequate triangulation and have poor ergonomics.2,3
Prior experience with magnetic-assisted laparoscopic surgery in adult and pediatric population has shown the safety, feasibility, and efficacy of this surgical technique. 7 In that experience, the adjunctive use of magnets enabled us either to reduce the number of ports needed or to perform transumbilical surgery. Our group first performed magnetic-assisted TUC with two magnets in both pediatric and adult patients, but it was cumbersome because of the potential for magnet collision, and we felt it was too complex to gain widespread adoption. The present study demonstrates the safety and efficacy of a hybrid technique during TUC in a pediatric population, showing adequate triangulation and optimal visualization of the critical view in all patients. In addition, there were no conversions to either open or laparoscopic (conventional) surgery, and no patient had an intraoperative or in-hospital complication. The hybrid technique utilizes an additional transumbilical (flexible) port where the second operator introduces and manipulates a curve grasper while the first operator is holding the laparoscope. In this fashion, we eliminated the need for a second internal magnet retractor without adding complexity to the procedure.
Our operative time was 62 minutes, which compares favorably with the time recently reported by Chandler and co-workers in a pediatric population undergoing conventional laparoscopic cholecystectomy (77 minutes) or TUC (68 minutes).9,10 In addition, the absence of intraoperative complications or superficial wound infections in the present study appears encouraging.
Several additional technical advantages of the use of internal magnetic retractors are worth mentioning. First, the internal magnet retractor is atraumatic, minimizing the risk for gallbladder perforation. The latter may constitute an advantage over other grasper systems or the use of sutures for organ retraction. Second, other deployable grasps require fixation to the level of the fascia, whereas the magnet retractor can be moved freely within the abdominal cavity. Repositioning of the magnet retractor to modify the traction force vector does not require additional insertion of a surgical tool into the abdomen, which per se constitutes a significant advantage over the currently available deployable grasps. Certainly, limiting this latter surgical gesture to a minimum prevents visual field obstruction and tool clashing and may eventually lower the risk of vessel or bowel perforation. Furthermore, the use of a magnet retractor allows retraction from extreme angulated positions, whereas currently available deployable mini-grasps systems usually cannot. In the case of the internal magnet falling out of range, the operator should move the external magnet around the abdomen to regain full control of the internal magnet. In our experience, this maneuver has always been successful. Second, deployment of the magnet reduces the number of surgical tools occupying part of the umbilical access, which facilitates the procedure. Third, available deployable grasps have limited strength of retraction, although in the case of the magnet retractor the strength of retraction is only dependent on the magnetic power. The operator can increase substantially the strength of retraction by augmenting the magnetic power of the external magnet or by using larger external magnets.
In our preliminary experience, we had adequate visualization of the critical angle in all cases. In order to avoid visual field obstruction, we combined the use of an operative scope and deployable magnetic retractors along with an additional port for the curve grasper that runs parallel to the operative scope. With this strategy, the surgeon only uses the working channel for clipping, dissection, and cutting. The absence of vascular or biliary complications in the present study may likely reflect adequate field visualization. There are potential limitations to our technique. It requires the use of dedicated magnetic devices and long surgical tools. Additionally, we also lengthened the Thomas forceps to allow for adequate reach through the scope. In addition, hybrid and non-hybrid magnetic-assisted techniques might not accommodate the internal magnet in small patients. Future manufacture of smaller magnets may allow this procedure in smaller patients. Lastly, magnet-assisted surgery entails the use of nonmagnetic surgical tools.
In conclusion, hybrid TUC is safe and effective in children. Similar to conventional laparoscopy, the hybrid technique possesses excellent ergonomics and provides adequate triangulation and the critical view, while eliminating permanent scars. The technique appears a practical solution to the poor ergonomics that are common in other SILS techniques.
Footnotes
Disclosure Statement
No competing financial interests exist.