
Abstract
Abstract
Background:
Femoral hernias in young children are relatively rare and can be difficult to diagnose as they are often mistaken for inguinal hernias. Although a few reports have described laparoscopic techniques, most traditional repair methods still focus on an open approach using either an inguinal or crural incision. Here we describe a laparoscopic-assisted technique that is buttressed by a cigarette of mesh for the repair of this uncommon pediatric entity.
Subjects and Methods:
We report three consecutive cases of children with femoral hernias repaired with only two small incisions: a 5-mm umbilical incision for a 30° camera and a 1-cm groin incision for dissection and ligation of the hernia sac. After sac ligation, the repair was buttressed with a small mesh cigarette.
Results:
Using this approach, right femoral hernias were repaired without complication in three children, between 8 and 9 years of age. Two patients had ipsilateral indirect inguinal hernias. No contralateral groin hernias were identified in any of the patients. Operative time averaged 40 minutes, recovery time was quick, and follow-up at 6 months revealed good cosmesis.
Conclusions:
This laparoscopic-assisted approach to pediatric femoral hernia repair with a small mesh plug is a safe, effective, and efficient technique. Because only two incisions are required, postoperative pain is minimal, and cosmesis is excellent. Nonetheless, more patients and longer follow-up will be required to accurately judge the long-term implications of this novel technique.
Introduction
The repair of femoral hernias has traditionally been undertaken in an open fashion via either an inguinal or crural incision,5,8–10 with just a few reports utilizing laparoscopic techniques.11–14 Recurrence rates can be high, perhaps because femoral hernias may involve a fascial defect of significant size.1,4,7 Thus, the typical approach of simple high ligation of the hernia sac used for indirect inguinal hernias may be inadequate for permanent femoral hernia repair. Here, we describe a laparoscopic-assisted technique that is buttressed by a small cigarette of mesh and requires only two incisions for the repair of this uncommon pediatric entity.
Patients and Methods
Patients
Over a 5-month period, 3 patients underwent our laparoscopic-assisted approach to femoral hernia repair. Two boys were referred by their pediatricians for an intermittent bulge located medially in the right groin. Both boys underwent a preoperative groin ultrasound to confirm the medial location of the hernia. They were scheduled for laparoscopic exploration with repair of their femoral hernias. One of these patients had previously undergone an open repair of a right indirect inguinal hernia.
The third patient presented with a right groin bulge noted when she coughed while waking up from general anesthesia after undergoing an uncomplicated appendectomy for nonperforated appendicitis. The patient was kept intubated while consent for laparoscopic-assisted hernia repair was obtained.
Surgical technique
After induction of general anesthesia, all patients received a dose of a prophylactic antibiotic. A 5-mm, 30° laparoscope was placed in the umbilicus to visualize the inguinal area bilaterally. A right-sided femoral hernia was identified in all 3 patients (Fig. 1). The laparoscope was advanced and placed into the femoral hernia sac in order to transilluminate the abdominal wall above the sac. A 1-cm skin incision was made with a 15-blade scalpel over the defect. Via the skin incision, the sac was grasped, dissected free of the surrounding tissue, twisted 360°, suture ligated with 3-0 Vicryl™ suture (Ethicon, Cincinnati, OH), and divided. A 2-×3-cm piece of monofilament polypropylene mesh (Prolene™; Ethicon) was rolled into a cigarette and sutured into shape with a 3-0 polypropylene stitch (Prolene) (Fig. 2). This piece of mesh was then stitched to the pectineal and inguinal ligaments with 3-0 Prolene in order to completely close the hernia defect (Fig. 3). Absorbable suture was used to close the subcutaneous tissue (interrupted 3-0 Vicryl) and skin (subcuticular 4-0 Monocryl™; Ethicon). The umbilical fascial incision was closed with a figure-of-eight 2-0 Vicryl stitch, and the skin was closed with simple plain gut stitches.
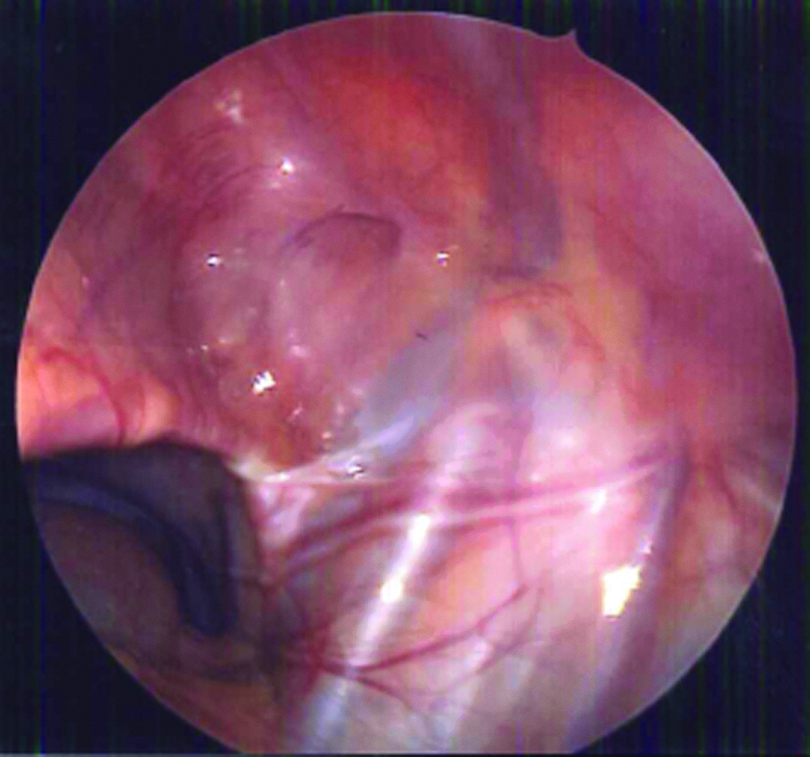
Right femoral hernia, laparoscopic view.
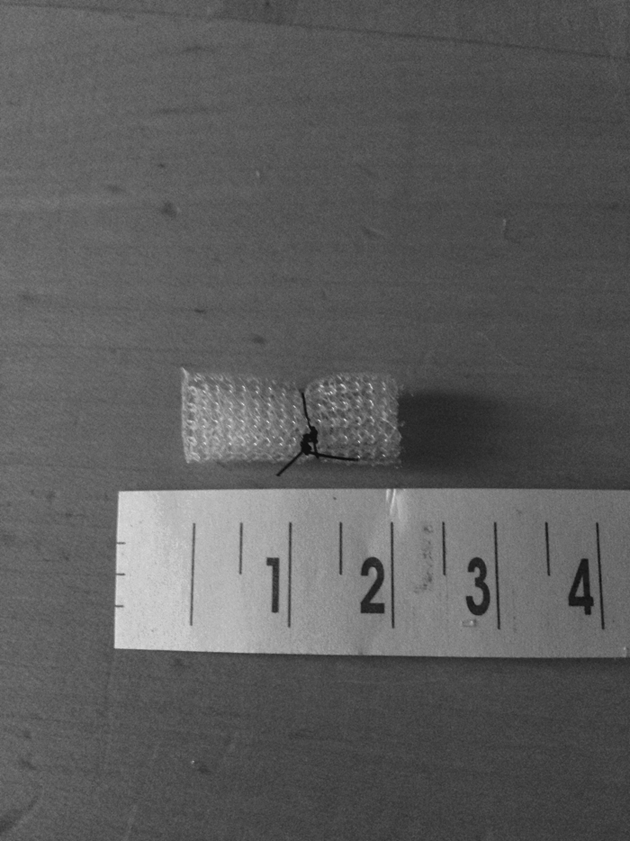
A 2-×3-cm piece of monofilament polypropylene mesh (Prolene; Ethicon) rolled into a cigarette and sutured into shape with a 3-0 polypropylene stitch (Prolene).
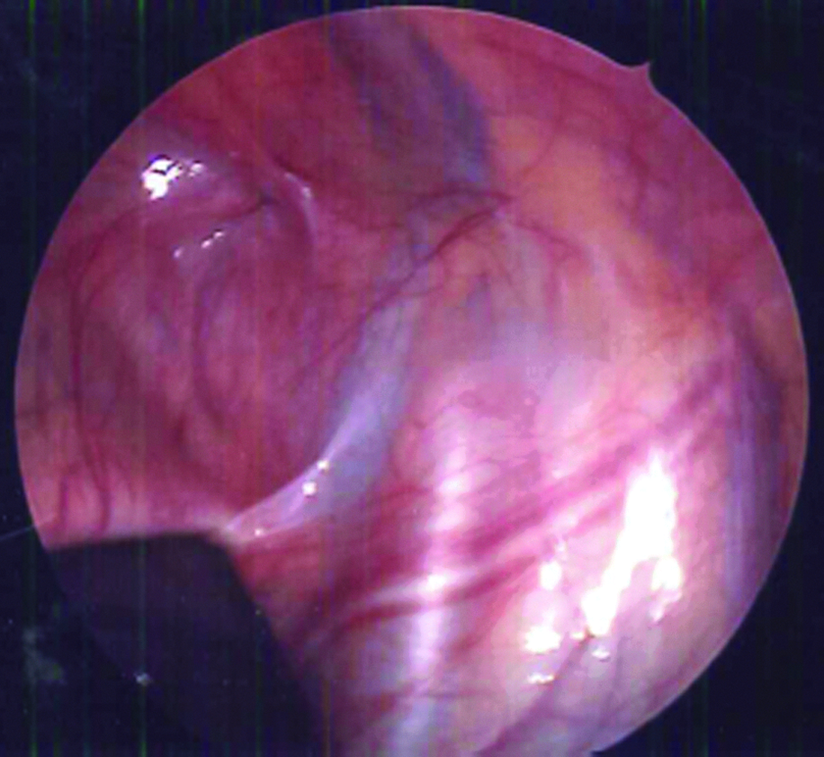
Right femoral hernia after repair, laparoscopic view.
Results
Our technique was used successfully to repair right femoral hernias in 3 patients: two boys and one girl between 8 and 9 years of age (mean, 8.5 years). Ipsilateral indirect inguinal hernias were present in 2 patients: one had been repaired previously, and one was identified during laparoscopic exploration of the right inguinal area. The indirect inguinal hernia identified intraoperatively was repaired in the laparoscopic-assisted fashion described by Dutta et al. 15 No left-sided hernias, inguinal or femoral, were found. Patients were ready for discharge on the day of surgery and had uneventful recoveries. Follow-up at 6 months revealed excellent cosmesis, without recurrence.
Discussion
Femoral hernias, which make up only approximately 1% of all pediatric hernias in the groin,1–4 pose a twofold challenge for surgeons. First, femoral hernias are prone to misdiagnosis because of their relative rarity. Indirect inguinal hernias are a much more common cause of reducible groin masses in children and may occur simultaneously with femoral hernias,4,8 as noted in 2 of our 3 patients. Thus, as the less likely diagnosis, femoral hernias may easily be missed in favor of repair of an indirect inguinal hernia, particularly when an open technique is used. Second, unlike pediatric indirect inguinal hernias, femoral hernias have an associated fascial defect that requires closure. Therefore, techniques that consist of hernia sac ligation alone may not be sufficient for long-term repair and might contribute to the high recurrence rates, which may range from 2% to 13%, for femoral hernia repair, whether open or laparoscopic.3,12
Although a standard approach to femoral hernias would necessarily involve narrowing the femoral canal to close the abdominal wall defect, there is still no consensus on what the simplest, most efficacious, and durable approach would be.
Recent reports have focused primarily on techniques that include laparoscopic groin exploration with femoral hernia repair.11–14 Although laparoscopy may help reduce the rate of missed diagnoses, closure of the fascial defect must still be addressed. Thus far, the reported laparoscopic and laparoscopic-assisted approaches mainly describe ligation of the femoral hernia sac with use of the proximal portion as a “plug” for the abdominal wall defect.11–14 The use of a natural biologic plug caused by the scarring of a ligated hernia sac or umbilical ligament to repair a hernia defect has been reported elsewhere as well.16,17 However, follow-up in these cases is insufficient to determine whether scarring from the native tissue will provide a long-term durable repair. Instead, we suggest that the addition of a mesh plug, as has been described for open repairs, 9 will provide the most permanent seal for a femoral hernia defect.
In our approach, we combine a laparoscopic exploration to evaluate both inguinal regions with the use of an infrainguinal incision for direct dissection of the femoral hernia sac and closure of the defect with a permanent plug of mesh. The external dissection, when coupled with laparoscopic guidance, reduces the size of the incision and the risk of injury to adjacent structures such as the femoral vessels. It also obviates the need for the additional incisions that would be required for a purely laparoscopic dissection of the sac. 13 Furthermore, the “cigarette” we form out of polypropylene mesh provides a more permanent plug for the abdominal wall defect. We hope that this will reduce the likelihood of recurrence of the hernia. Because the defect is directly visualized both internally and externally, it can be evaluated and palpated so that our plug can be tailored to fit the size of the fascial gap. In this way, only a modest size of mesh need be used to reduce concerns of foreign-body placement in pediatric patients.
Conclusions
We have described a laparoscopic-assisted approach to pediatric femoral hernia repair that is straightforward, safe, efficacious, and efficient. The addition of laparoscopy to a traditional open approach aids in the diagnosis and localization of the femoral hernia sac, as well as provides the ability to examine the contralateral groin for hernias. Because dissection of the hernia sac is performed externally, only two incisions are required, for the camera and the hernia itself. The addition of a small mesh plug buttresses and secures the remaining abdominal wall defect, which is associated with a femoral hernia. More patients and longer follow-up are essential to accurately judge the long-term implications of this novel technique.
Footnotes
Disclosure Statement
No competing financial interests exist.