
Abstract
Abstract
Background:
Endoscopic thyroid surgery is gaining wide acceptance; however, existing endoscopic methods for thyroidectomy have shown several limitations. Recently, a transoral technique using video assistance and endoscopy has been reported for thyroidectomy. The aim of this study was to define a new technique of transoral thyroidectomy using a mandibular periosteal approach to complement other types of natural orifice surgery and minimally invasive surgery.
Materials and Methods:
Transoral periosteal thyroidectomies were performed in seven living pigs to evaluate the feasibility and safety of the new approach. Total thyroidectomies were performed in all animals. Follow-up examinations were carried out for 7 days and followed by autopsy.
Results:
Through three trocars in the mandibular periosteal area, it was possible to create a working space under the platysma muscle and to reach the pretracheal area. Total thyroidectomies were also performed via the transoral, mandibular periosteal approach without complications in seven orally intubated living pigs. Postoperatively, the white blood cell count remained normal in all cases. On the postoperative sacrifice of the pigs, three locally encapsulated seromas were observed. Both recurrent laryngeal nerves were intact in all cases.
Conclusions:
Transoral periosteal thyroidectomy could be feasible and safe.
Introduction
T
Transoral thyroidectomy was recently introduced for minimally invasive thyroid resection. Witzel et al. 4 were the first to attempt this procedure by using a single access port with an accessory anterior neck port in 2008. This procedure is still experimental and in fact is a hybrid approach because it is not a totally transoral approach. Since then, Wilhelm and co-workers introduced the transoral, video-assisted thyroidectomy technique, which is an entirely transoral endoscopic approach and therefore a natural orifice surgery.5–8 Karakas et al. 9 were the first to perform transoral thyroid and parathyroid surgery using a lateral sublingual approach. Richmon et al. 10 also introduced a transoral technique for robotic thyroidectomy using the transoral, video-assisted thyroidectomy method.
Recently, Wilhelm and Metzig 8 reported a clinical study of transoral thyroidectomy in 8 patients. We believe that their procedure is the most feasible and successful surgery of all the previously mentioned methods. However, this technique does carry some risk to the mental nerve from the lateral gingival–buccal port placement, as well as risk to Wharton's duct and the upper teeth and nose due to placement of the midline port.
We developed a mandibular periosteal approach that does not limit the movement of endoscopic instruments and minimizes the risk of injury to the upper teeth, nose, and mental nerves. We evaluated the procedure in a short-term survival animal trial to prove the safety of the new technique.
Materials and Methods
Subjects
Permission to perform this experimental trial was obtained from the Korea University Institutional Animal Care and Use Committee (Seoul, Korea) under protocol number KUIACUC-2011-150 (August 17, 2011). Seven pigs (race: country pig–large black–Hampshire), weighing 30–40 kg, were used to evaluate the feasibility and safety of the minimally invasive endoscopic approach to the anterior neck region through the transoral approach.
Anesthesia
Preoperatively, the pigs were fasted for 12 hours. After intramuscular pre-anesthetic medication with xylazine (Rompun®; Bayer, Leverkusen, Germany) (1 mg/kg) and zolazepam/tiletamine (Zoletil®; Virbac S.A., Carros, France) (7 mg/kg), the pigs were then placed on an operating table in the supine position with their necks extended. Afterward, a pulse oximeter and electrocardiogram were attached. The pigs were intravenously cannulated at the auricular vein and received a continuous intravenous infusion of lactated Ringer's solution at 5 mL/kg/hour throughout the operation. Vecuronium (bolus dose of 0.15 mg/kg) was injected for muscle relaxation. After that, the pigs were intubated with a standard cuffed endotracheal tube (Portex®; Smiths Medical, Watford, United Kingdom). The size of the endotracheal tube was determined by visual inspection of the larynx and confirmed by the ability to pass the tube without resistance. We used a 6-mm internal diameter endotracheal tube in all cases. The endotracheal tube cuff was inflated with the minimum amount of air that still allowed a small air leak. Tidal volume and respiratory rate were set at 8 mL/kg and 15 breaths/minute, respectively. After oral intubation, intravenous prophylactic antibiotics in the form of a single shot of 1500 mg of cefuroxime were applied.
Laboratory tests
We performed laboratory tests (white blood cell counts, free thyroxine [T4] level, and thyroid-stimulating hormone [TSH] level) preoperatively and at postoperative day 7.
Operative methods
All endoscopic procedures were performed using conventional laparoscopic instruments (Ethicon Endo Surgery, a Johnson & Johnson Company, Cincinnati, OH) and a 30° endoscope (Visera system; Olympus Medical, Tokyo, Japan). We performed transoral thyroidectomy in four pigs using four ports (Fig. 1) and in three pigs using three ports.

Port placement for the transoral periosteal thyroidectomy in the swine model. All trocars and instruments are shown in place.
Port placement and flap dissection
A critical component of this study was making the incisions for port placement. The incisions for all four ports were made through the mandibular periosteum with a periosteal elevator. Using this mandibular periosteal approach, we avoided injury to Wharton's duct or transaction of the mentalis muscle. For the camera port, a 2-cm incision was made by a crevicular incision into the buccal surface of the central incisors. We extended the bilateral vertical incisions into the alveolar mucosa and raised mucoperiosteal flaps on the buccal surface at the midline using a periosteal elevator. Dissection continued around the inferior aspect of the mandible until the subplatysmal plane was identified. By this technique, the camera port had access through the periosteum of the mandible. The dissection plane was made naturally at the subplatysmal area without any artificial force required. For the working port, we made another 1.5-cm incision in the midline of the lingual surface in the same manner as the camera port incision. To avoid injury to the mental nerves, two more 0.8-cm incisions were made in the gingival–buccal sulcus at the level of the first molar. Dissection proceeded along the periosteum of the mandible into the submental area.
We placed 5-mm bariatric cannulae in the two lateral incisions and 12-mm bariatric cannulae in the two midline incisions. A 30° endoscope was advanced through the 12-mm camera port of the buccal surface at midline into the submental, subplatysmal area. While creating the working space and performing the right thyroidectomy, the operator used the midline port on the lingual surface and the left lateral port, and the assistant used the right lateral port. For the left thyroidectomy, the midline port in the lingual surface and the right lateral port were used by the operator. After CO2 insufflation (4–6 mm Hg), a working space was made in the subplatysmal plane that extended up to the suprasternal notch inferiorly and to the medial border of the sternocleidomastoid muscles laterally (Fig. 2).
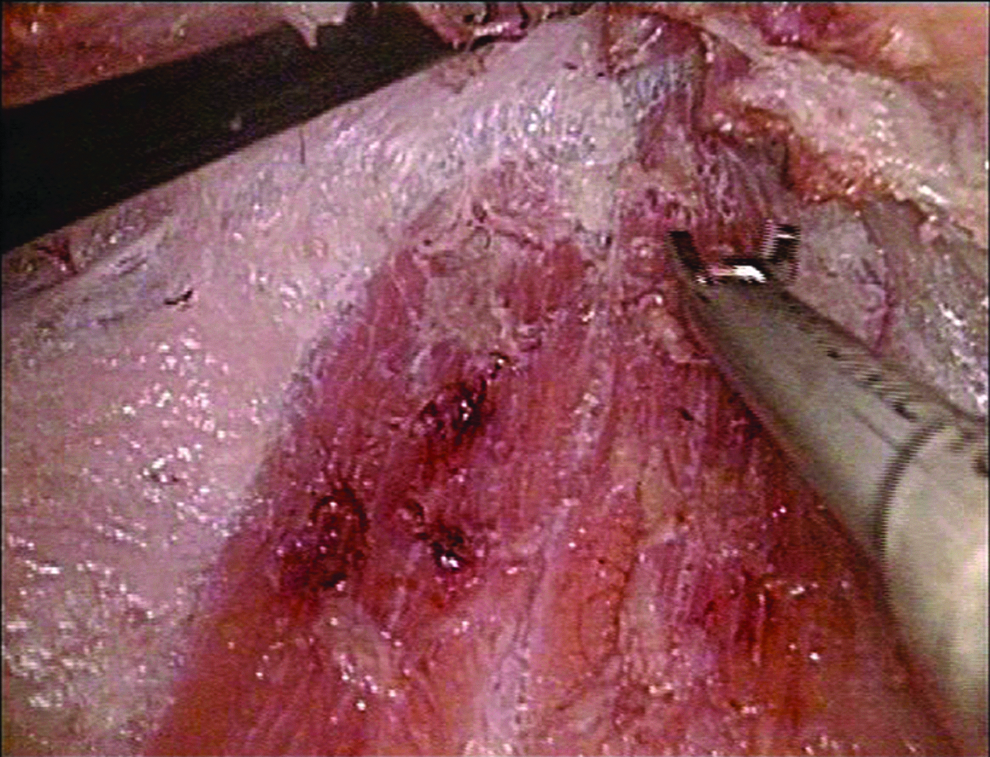
Dissection of the subplatysmal flap. During transoral periosteal thyroidectomy, this is the access to the subplatysmal area. The operator dissects the flap using a Harmonic scalpel. The muscle on the bottom of this photograph is strap muscle.
Operative methods
The anatomical relations in pigs and humans are very similar, especially regarding the thyroid region and the recurrent laryngeal nerve. However, the porcine thyroid is smaller than the human thyroid and is positioned mainly at the anterior portion of the trachea rather than the lateral portion of the trachea. Thus the thyroid is less intimately involved with the recurrent laryngeal nerve in swine. Therefore, after the thyroidectomy, we performed additional dissection to find both recurrent laryngeal nerves in the swine experiments.
The resected specimen was removed transorally from the operative field through a midline incision in the lingual or buccal surface. After thyroidectomy, we visualized an intact mentalis muscle and closed the midline incisions by suturing the interdental papillae together.
Using four ports, surgeons were able to more smoothly manipulate the thyroid and surrounding tissues and to control bleeding more easily than when using only three ports. However, there is a risk of injury to the nose and upper teeth due to the midline port placement in the lingual surface. This port also limits movement and induces collisions with other ports. Therefore, we attempted a transoral periosteal thyroidectomy in three pigs using only three ports (without the midline port in the lingual surface). In this method, the operator performed the thyroidectomy using two lateral ports and a midline port in the buccal surface, which was used for endoscope access. Even with only three ports, we were able to perform a total thyroidectomy and central lymph node dissection successfully, without any collisions between instruments. After the procedure, we dissected the anterior neck and found that both recurrent laryngeal nerves were intact. In the fourth case, we inserted a Jackson–Pratt drain at two fingerbreadths above from the sternal notch on the anterior neck.
Postoperative follow-up
We observed that the animals woke up breathing spontaneously within 3 hours postoperatively. For the next 2 days, all animals were observed to establish pain reactions and reinstitute oral feeding. Possible pain reactions were estimated based on their social behavior in the sty. Normally, the animals fought with each other, especially during feeding. On postoperative day 7, all animals were anesthetized and orally intubated with an EMG endotracheal tube. We checked the incision sites in the oral cavity and the anterior cervical region. During examination, we checked both recurrent laryngeal nerves using intraoperative neuromonitoring.
Results
In swine experiments, we evaluated the feasibility and safety of the minimally invasive endoscopic approach to neck surgery through the oral cavity. Details of each pig are given in Table 1. In each case, the anterior neck could be reached endoscopically without a problem. There was no bleeding that required surgical intervention or conversion to an open procedure. The mean total operative time was 122.9 minutes (range, 92–139 minutes). The average weight of the thyroid specimens was 4.5 g. Total thyroidectomy was performed completely in all seven swine. During the postoperative period, abnormal behaviors related to pain or complications were not observed, and oral intake was good in all swine. We found that all 14 recurrent laryngeal nerves were intact within operative fields and during postoperative examinations (Figs. 3 and 4).
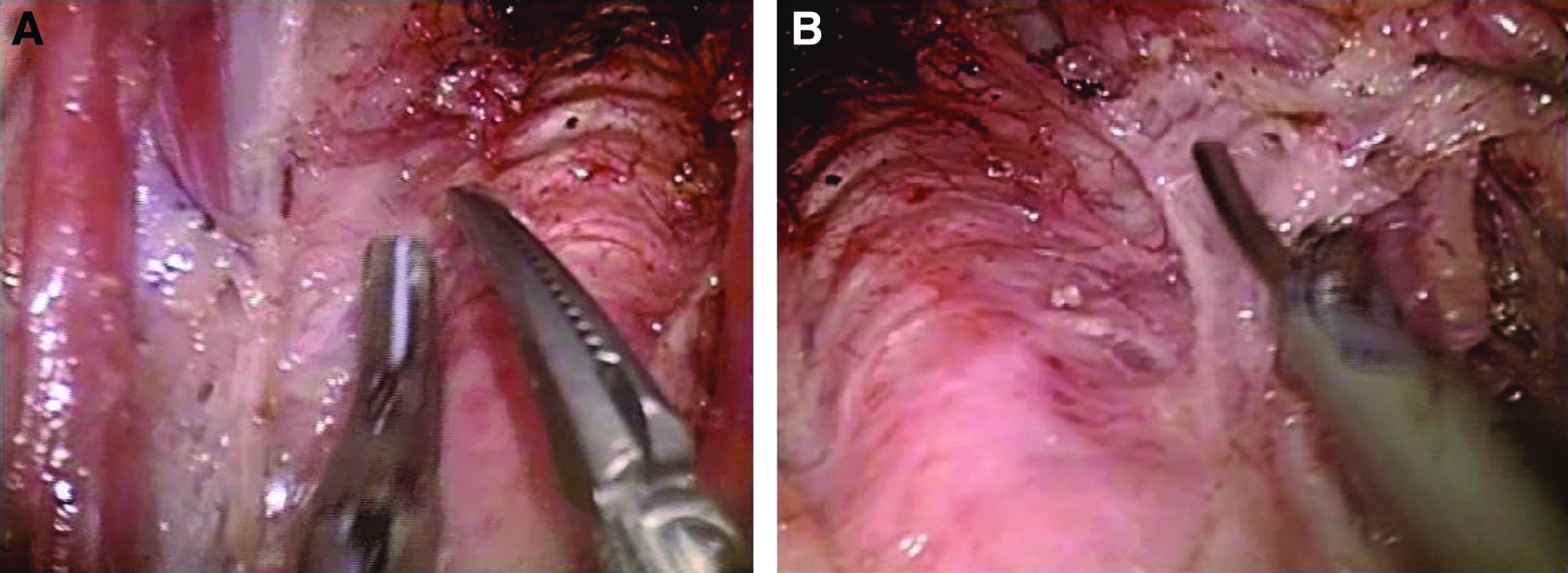
Recurrent laryngeal nerve during transoral periosteal thyroidectomy in the swine model:

Intraoperative neuromonitoring during examination at postoperative day 7. APS, automatic periodic stimulation; RLN, recurrent laryngeal nerve; Vagus N., vagus nerve.
L, left; R, right; T4, thyroxine; WBC, white blood cell.
In laboratory findings, white blood cell counts were normal in six swine. However, in the first case, the white blood cell count was increased at postoperative day 7. It was likely related to an infected seroma (70 mL) that we observed in the subplatysmal area. Seromas (30 mL and 50 mL, respectively) were also observed in the second and third cases (Fig. 5A). So, from the fourth case on, we inserted a Jackson–Pratt drain in the operative field (Fig. 5B). After that, we did not observe any other seromas or infections.
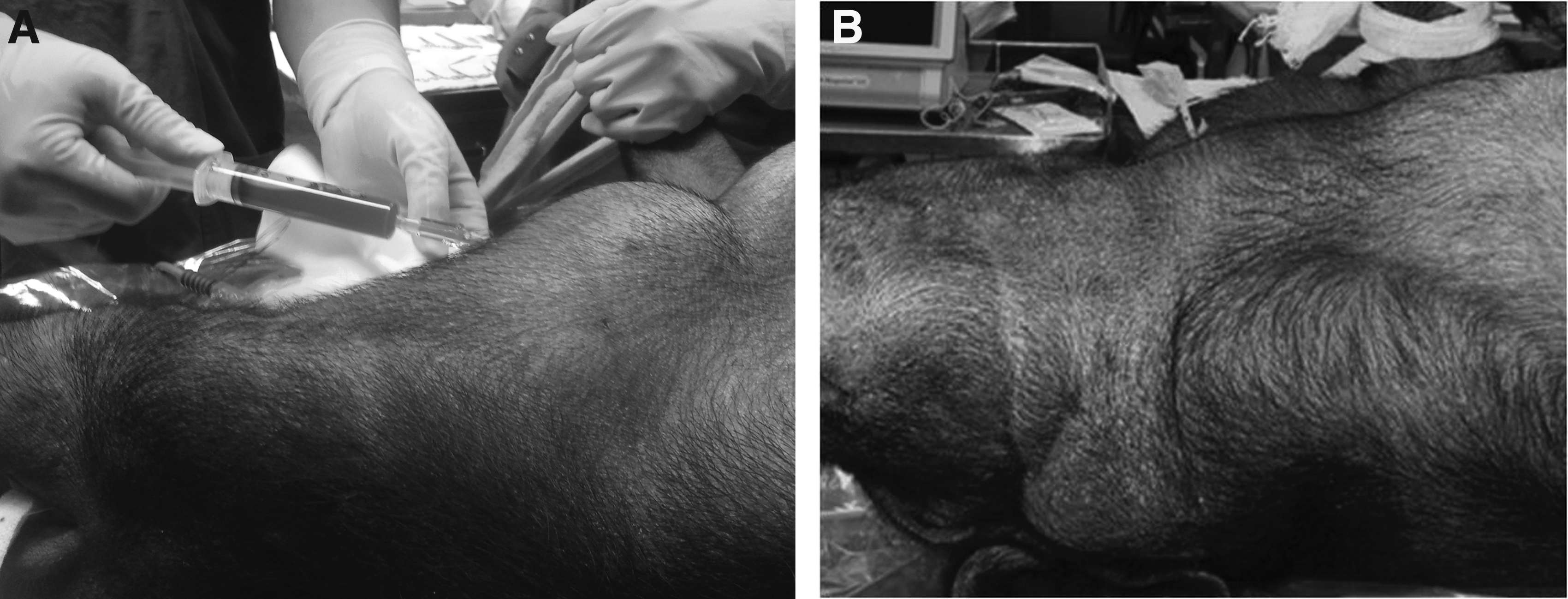
Photographs of the external appearance of swine at postoperative day 7:
We also checked free T4 and TSH levels. Preoperative free T4 levels varied from 4.0 to 4.5 μg/dL. In all seven swine, the postoperative free T4 level decreased to below 0.3 μg/dL. Preoperatively and postoperatively, TSH levels in all seven swine were below 0.5 μg/dL. It seems that normal TSH levels in swine are lower than in humans. We did not observe any injuries to structures in the oral cavity during the procedures or intraoral wound complications during examination at postoperative day 7.
Histological examination of resected specimens was performed. After hematoxylin and eosin staining, we observed the simple cuboidal epithelium lining the follicles, called thyroid follicles (Fig. 6A). In the fifth case, we resected one lymph node in the central neck region (Fig. 6B).
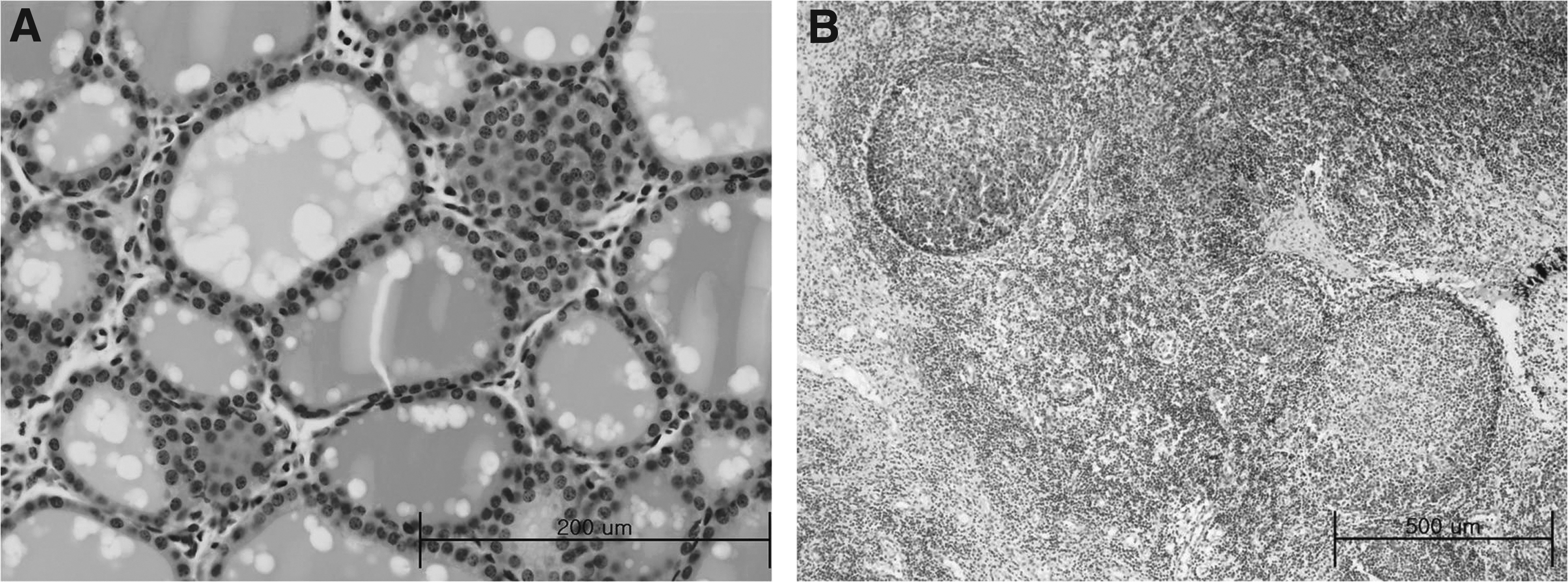
Histological examination of porcine
As in the cadaver experiments, we performed transoral thyroidectomy using four ports and three ports in the swine experiments. Because swine have very large and heavy mandibles, the working port in the lingual surface at the midline had severe limitations in range of motion. Therefore, three-port transoral thyroidectomy was more reasonable in swine experiments.
Discussion
Several studies have been published regarding transoral neck surgery, in particular thyroidectomy. These transoral thyroid approaches are based on the concept of natural orifice, transluminal endoscopic surgery. However, there are some limitations in previous methods of transoral thyroidectomy. A potentially major complication is injury to the mental nerve by the lateral ports used in these procedures.3,4 Wharton's duct could also be damaged by the placement of the midline port.2,7 Many other structures in the oral cavity can be injured as well, such as the upper teeth and nose. To overcome these limitations, we developed a new technique for transoral thyroidectomy using a mandibular periosteal approach.
All ports were made through the mandibular periosteum using a periosteal elevator to avoid transaction of the mentalis muscle or damage to Wharton's duct. The major advantage of a mandibular periosteal approach is easy access to the subplatysmal area. In other methods of endoscopic thyroidectomies, it is very difficult to access the correct plane under the platysmal muscle. However, we can freely access the subplatysmal area through the mandibular periosteum by a periosteal elevator.
This is the first animal study of transoral thyroidectomy using four ports. All previous transoral thyroidectomies have been performed using three or fewer ports.1,4,5,8 All four ports were placed intraorally, and no scars were visible. Of the four ports, one was for the camera, one was used by the active surgeon, and the third port was used by the assisting surgeon; the last port was purely for assisting. Without an additional assisting port, methods using three ports have a critical limitation because excessive retraction of the thyroid and other tissues is essential during the procedure in order to identify accurate surgical planes. Excessive retraction of the thyroid and tissues leads to severe complications, such as injury of the recurrent laryngeal nerve or bleeding. In contrast, surgeons using a four-port method can smoothly manipulate the thyroid and surrounding tissues without extreme retraction. Moreover, by using four ports, the surgeon can more easily respond to bleeding.
When four ports are used, the midline port is typically placed in the posterior aspect of the mandible, which can impinge on the maxillary teeth and nose. This port thus has a limitation of movement. Furthermore, in patients in whom the maxilla is larger than the mandible, it is nearly impossible to make the incision or flap for the posterior midline port. Therefore, we performed transoral thyroidectomy using three ports. There were no severe collisions between instruments. However, as previously mentioned, it is not possible to avoid excessive retraction of the thyroid and tissues without an additional assisting port. Nevertheless, after the procedure, we found that both recurrent laryngeal nerves were intact in all pigs, as well as the mental nerves and other important structures in the anterior neck region. Therefore, transoral periosteal thyroidectomy using both four and three ports appears to be feasible.
We performed this new transoral periosteal thyroidectomy in swine to prove the safety of the methods. None of the swine had any severe infections. Only one pig had an infected seroma, and two had sterile seromas, but after drain insertion, there were no seromas in the operative field. Therefore, so long as prophylactic antibiotics are given and drain insertion is performed, infection can be controlled after a transoral endoscopic surgery. However, because of the small sample size, we cannot draw strong conclusions about the risk of infection in transoral thyroidectomy. In all swine models, total thyroidectomies were completely performed, and on the postoperative examinations, both recurrent laryngeal nerves were intact. So we have shown that transoral periosteal thyroidectomy can be performed safely.
This method is still in a developmental stage, and further studies are needed to evaluate its safety. Furthermore, this transoral technique carries the risk of infection in the anterior neck region. A normally clean operation may become a clean-contaminated surgical intervention due to the spreading of oral microflora during neck exploration. The next logical step would be implementation of transoral thyroidectomy in a prospectively controlled clinical setting. For clinical trials, the development of a safety device to protect structures in the oral cavity will also be required.
Conclusions
This swine study of transoral periosteal thyroidectomy has shown that this method might be feasible and effective for thyroid surgery. For the application of this method to humans, further investigation, like an animal study or prospective clinical trial, will be needed to prove the safety of this technique.
Footnotes
Acknowledgment
The research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science, and Technology (2012R1A1A1013413) and supported by a Korea University grant (K1325271).
Disclosure Statement
No competing financial interests exist.